Download as docx, pdf, or txt
You might also like
- Marquez - Case Study 4Document4 pagesMarquez - Case Study 4Caren MarquezNo ratings yet
- Marquez - Case Study 3Document6 pagesMarquez - Case Study 3Caren MarquezNo ratings yet
- Marquez - Case Study 122Document5 pagesMarquez - Case Study 122Caren MarquezNo ratings yet
- Case Study Chapter 33Document3 pagesCase Study Chapter 33Anjae GariandoNo ratings yet
- Marquez - Case Study 120Document4 pagesMarquez - Case Study 120Caren Marquez100% (1)
- Case Study: Chapter 10 Pediatric DisordersDocument6 pagesCase Study: Chapter 10 Pediatric DisordersRica AvendañoNo ratings yet
- Peds Presentation MeningitisDocument20 pagesPeds Presentation Meningitisapi-533578725No ratings yet
- Nurse Practitioner Board ReviewFrom EverandNurse Practitioner Board ReviewRating: 5 out of 5 stars5/5 (1)
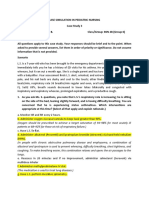
- Case Simulation 3 in Pediatric NursingDocument3 pagesCase Simulation 3 in Pediatric NursingCaren Marquez100% (1)
- NCP For Ectopic PregnancyDocument4 pagesNCP For Ectopic PregnancyClarissa_Dante_735850% (4)
- Nursing Review BulletsDocument125 pagesNursing Review BulletsROBERT C. REÑA, BSN, RN, MAN (ue)96% (46)
- Community Assessment PaperDocument6 pagesCommunity Assessment Paperapi-543558169No ratings yet
- Contemporary Orthodontics, 5th EditionDocument2 pagesContemporary Orthodontics, 5th EditionAasharAshrafNo ratings yet
- TeratologyDocument34 pagesTeratologyธิติวุฒิ แสงคล้อย100% (1)
- Intestnal ObstructionDocument4 pagesIntestnal ObstructionRenea Joy ArruejoNo ratings yet
- Case Study - Hematology 1 PDFDocument21 pagesCase Study - Hematology 1 PDFMaria Lyn Ocariza ArandiaNo ratings yet
- Intravenous Therapy in Clinical PracticeDocument8 pagesIntravenous Therapy in Clinical PracticeTyron Rigor Silos100% (1)
- DX Intracranial Pressure PDFDocument8 pagesDX Intracranial Pressure PDFSherree HayesNo ratings yet
- Postpartal Discharge InstructionsDocument3 pagesPostpartal Discharge InstructionsDuchess Juliane Jose MirambelNo ratings yet
- Hypovolemic Shock Sample NCPDocument14 pagesHypovolemic Shock Sample NCPRENEROSE TORRES100% (1)
- NCP 3rd ROTATIONDocument17 pagesNCP 3rd ROTATIONMarie Ashley CasiaNo ratings yet
- Subjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Document5 pagesSubjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Erle Gray CadangenNo ratings yet
- Nursing Review BulletsDocument53 pagesNursing Review BulletscauldroNo ratings yet
- Electolyte ImbalanceDocument2 pagesElectolyte ImbalanceFouzia GillNo ratings yet
- Sample Case Pres - ScenarioDocument15 pagesSample Case Pres - ScenariogustomonglemonNo ratings yet
- Nle BulletsDocument53 pagesNle BulletsdjhemzNo ratings yet
- Case Study 2Document19 pagesCase Study 2Sumit Singh100% (1)
- Casia-Research Topic-Kawasaki SyndromeDocument10 pagesCasia-Research Topic-Kawasaki SyndromeMarie Ashley CasiaNo ratings yet
- Risk NCP - PESCADERO 4CDocument1 pageRisk NCP - PESCADERO 4COrlando VillanuevaNo ratings yet
- Campugan, Jay NCP PT 14-08-2023Document8 pagesCampugan, Jay NCP PT 14-08-2023Flower Flower FlowerNo ratings yet
- Case Simu 104Document4 pagesCase Simu 104Princess Levie CenizaNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale Evaluation Subjective: Noc: NIC: Fluid ManagementDocument10 pagesCues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale Evaluation Subjective: Noc: NIC: Fluid ManagementSkyla FiestaNo ratings yet
- Nursing Care Plan: IndependentDocument1 pageNursing Care Plan: IndependentJay Mar BabateNo ratings yet
- Gonzaga Rlems - NCPDocument3 pagesGonzaga Rlems - NCPShaynne Wencille A. GONZAGANo ratings yet
- Pediatric Meningitis Case StudyDocument5 pagesPediatric Meningitis Case StudyCheska PalomaNo ratings yet
- Gi-Rle - NCP For Deficient Fluid VolumeDocument2 pagesGi-Rle - NCP For Deficient Fluid VolumeEvangeline Villa de Gracia100% (1)
- Agn NCPDocument6 pagesAgn NCPJewel AnneNo ratings yet
- Ischemic StrokeDocument25 pagesIschemic Strokebcdpqyck8xNo ratings yet
- Planning Intervention Rationale Evaluation: Nursing Care Plan Problem DiagnosisDocument2 pagesPlanning Intervention Rationale Evaluation: Nursing Care Plan Problem DiagnosisRicardo Dela CruzNo ratings yet
- NCP Example Pre EclampsiaDocument6 pagesNCP Example Pre EclampsiaChristian Joseph OpianaNo ratings yet
- NCP PediatricDocument5 pagesNCP PediatricSL Hanna NebridaNo ratings yet
- Salva, R.D NCP & Drug Study (Isph - Gs Pediaward)Document7 pagesSalva, R.D NCP & Drug Study (Isph - Gs Pediaward)Rae Dominick Aquino SalvaNo ratings yet
- BETLOGDocument12 pagesBETLOGlucerodommmmNo ratings yet
- NCP ModsDocument5 pagesNCP ModsErryl Justine AdvinculaNo ratings yet
- Diverticulitis Case StudyDocument2 pagesDiverticulitis Case StudyAhmad RizkiNo ratings yet
- Nursing Care PlanDocument12 pagesNursing Care Plankeishaaa29100% (6)
- Resource Unit On Drugs and IVF's: College of NursingDocument7 pagesResource Unit On Drugs and IVF's: College of NursingJ Michael EscaraNo ratings yet
- Nursing Care Plan RepairedDocument4 pagesNursing Care Plan RepairedNiña Mae MarasiganNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationDocument4 pagesNursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationAngelica Charisse BuliganNo ratings yet
- Pae Risk of InfectionDocument3 pagesPae Risk of InfectionScribdTranslationsNo ratings yet
- MS Soapie #1Document2 pagesMS Soapie #1Fatima KateNo ratings yet
- TTP Care Plan 1 JevansDocument8 pagesTTP Care Plan 1 Jevansapi-439893609No ratings yet
- DX Spine Injury PDFDocument5 pagesDX Spine Injury PDFSherree HayesNo ratings yet
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- Prince NCPDocument9 pagesPrince NCPALVARADO, KRISTINE JOYNo ratings yet
- Intussuception Is A Condition in Which Part of The Intestine Folds Into The Section Next To ItDocument3 pagesIntussuception Is A Condition in Which Part of The Intestine Folds Into The Section Next To ItEduard GarchitorenaNo ratings yet
- CASE ANALYSIS IMMUNITY (Operaña, Ellayza)Document5 pagesCASE ANALYSIS IMMUNITY (Operaña, Ellayza)OPERAñA ELLAYZA RB DECANONo ratings yet
- NCP PediaDocument9 pagesNCP Pediajuworski1No ratings yet
- CAT Tool, Nursing Care PlanDocument7 pagesCAT Tool, Nursing Care Planpriyanshikataria1020No ratings yet
- CASE STUDY PPT Group1 - Revised WithoutvideoDocument34 pagesCASE STUDY PPT Group1 - Revised WithoutvideoSamantha BolanteNo ratings yet
- Case Study Jim SandersonDocument6 pagesCase Study Jim SandersonJessica McAlexanderNo ratings yet
- Care Plan Number 2Document5 pagesCare Plan Number 2Teddy mc Bones100% (1)
- Presentation Dengue FeverDocument21 pagesPresentation Dengue Feverpolarbear12121250% (2)
- Nursing Care Plan For Mother:: Sno Assessment Diagnosis Planning Implementation EvaluationDocument4 pagesNursing Care Plan For Mother:: Sno Assessment Diagnosis Planning Implementation Evaluationmishti100% (1)
- Related Learning Experience Fundamentals in Nursing 4 RotationDocument3 pagesRelated Learning Experience Fundamentals in Nursing 4 RotationMark Eliezer CulasingNo ratings yet
- User's Guide to Inflammation, Arthritis, and Aging: Learn How Diet and Supplements Can Reduce Inflammation and Slow the Aging ProcessFrom EverandUser's Guide to Inflammation, Arthritis, and Aging: Learn How Diet and Supplements Can Reduce Inflammation and Slow the Aging ProcessNo ratings yet
- Nursing Diagnosis Objectives Nursing Interventions Rationale Risk For InjuryDocument1 pageNursing Diagnosis Objectives Nursing Interventions Rationale Risk For InjuryCaren MarquezNo ratings yet
- Marquez - Case Study 114Document6 pagesMarquez - Case Study 114Caren MarquezNo ratings yet
- Case Study 2Document12 pagesCase Study 2Caren MarquezNo ratings yet
- Case StudyDocument7 pagesCase StudyCaren MarquezNo ratings yet
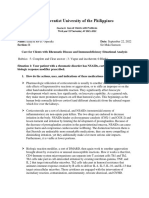
- Informatics and Nursing Sensitive Quality Indicators: Name Institution Date CourseDocument5 pagesInformatics and Nursing Sensitive Quality Indicators: Name Institution Date CourseKevin SangNo ratings yet
- A Field Manual of Camel Diseases Traditional and Modern Health Care For The DromedaryDocument273 pagesA Field Manual of Camel Diseases Traditional and Modern Health Care For The DromedaryHenrique100% (3)
- VenoferDocument13 pagesVenoferLuciano H.Vivas M.No ratings yet
- Daftar Pustaka ReferatDocument2 pagesDaftar Pustaka ReferatBetharlitha PurLikaNo ratings yet
- Nemio Brochure MCAUS0642Document4 pagesNemio Brochure MCAUS0642Engineer AwaisNo ratings yet
- U.S. Department of Defense: Enlisting Open-Source ApplicationsDocument6 pagesU.S. Department of Defense: Enlisting Open-Source Applicationstanmoy8554No ratings yet
- Application and Eligibility - Medical Council of Canada - Le Conseil Médical Du CanadaDocument2 pagesApplication and Eligibility - Medical Council of Canada - Le Conseil Médical Du CanadaJimmyTungNo ratings yet
- Uterine Prolapse and Its Homeopathic Cure - Bashir Mahmud ElliasDocument2 pagesUterine Prolapse and Its Homeopathic Cure - Bashir Mahmud ElliasBashir Mahmud ElliasNo ratings yet
- BHME-102 UNIT 1 AND 2 11-10-18 (1) IgnouDocument55 pagesBHME-102 UNIT 1 AND 2 11-10-18 (1) IgnouShalini MalhotraNo ratings yet
- Case Study - Intestinal Resection and Anastomosis in A DogDocument13 pagesCase Study - Intestinal Resection and Anastomosis in A Dogapi-301746262No ratings yet
- West Sherburne TribuneDocument14 pagesWest Sherburne TribunewestribNo ratings yet
- Kindergarten RhymesDocument15 pagesKindergarten RhymesAkshit R Shah100% (1)
- Analisis Jurnal RCTDocument10 pagesAnalisis Jurnal RCTAdelia Dwi KusumaNo ratings yet
- Knowledge, Attitude and Perception Regarding Halal Pharmaceuticals, Among Academicians in Various Universities of MalaysiaDocument12 pagesKnowledge, Attitude and Perception Regarding Halal Pharmaceuticals, Among Academicians in Various Universities of MalaysiaHera RamayantiNo ratings yet
- New Trends in TuberculosisDocument36 pagesNew Trends in TuberculosisJaid Mulla UTNo ratings yet
- Professional Services, Inc. vs. Agana, G.R. No. 126297, February 11, 2008Document11 pagesProfessional Services, Inc. vs. Agana, G.R. No. 126297, February 11, 2008Raikha D. BarraNo ratings yet
- Bates Test Bank Chapter 3 PDFDocument3 pagesBates Test Bank Chapter 3 PDFJoseph De JoyaNo ratings yet
- PROPOSED PUERTO PRINCESA HEALTH CENTER: Enhancing Tuberculosis Patient Detection and CareDocument7 pagesPROPOSED PUERTO PRINCESA HEALTH CENTER: Enhancing Tuberculosis Patient Detection and CareJaerald CruzNo ratings yet
- Diagnosa Dokter Mata 2021-2023Document14 pagesDiagnosa Dokter Mata 2021-2023RSUD MatramanNo ratings yet
- Dermasim PDFDocument3 pagesDermasim PDFSilent ScreamNo ratings yet
- Benzo Withdrawal SyndromeDocument7 pagesBenzo Withdrawal SyndromeWernerNo ratings yet
- BPPVDocument8 pagesBPPVAshish GuptaNo ratings yet
- Physical Assessment Health AssessmentDocument6 pagesPhysical Assessment Health AssessmentADOLF FRUELAN HIDALGONo ratings yet
- Caring For Rabbits 1995Document11 pagesCaring For Rabbits 1995Dario Luengo GevaraNo ratings yet
- Approved: Tertiary HospitalsDocument26 pagesApproved: Tertiary Hospitalsmurtada gubaNo ratings yet
- M 4Document19 pagesM 4Ritika JangraNo ratings yet
- Management of Lymphatic Malformations in ChildrenDocument8 pagesManagement of Lymphatic Malformations in ChildrenAyuRosemeiliaDewiNo ratings yet