Download as doc, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- GCAA Air Law ReviewDocument43 pagesGCAA Air Law ReviewAnonymous BiosaDDZVH100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Combining Convolutional Neural Network With Recursive Neural Network For Blood Cell Image ClassificationDocument2 pagesCombining Convolutional Neural Network With Recursive Neural Network For Blood Cell Image ClassificationAnonymous 1aqlkZNo ratings yet
- Isuzu Exp Ubs Workshop Manual Part 3Document20 pagesIsuzu Exp Ubs Workshop Manual Part 3hope100% (61)
- Parasitology For DummiesDocument8 pagesParasitology For DummiesimranNo ratings yet
- LABOR LAW I - Finals Case DigestsDocument8 pagesLABOR LAW I - Finals Case DigestsLDNo ratings yet
- Back To NatureDocument10 pagesBack To NaturetattoNo ratings yet
- Training and Development FGHGH GDocument82 pagesTraining and Development FGHGH GMichael WellsNo ratings yet
- Ben Senouci Douidi: Certificate of AchievementDocument2 pagesBen Senouci Douidi: Certificate of AchievementDakota624No ratings yet
- Itp Equipment (Static)Document5 pagesItp Equipment (Static)Rajeev KumarNo ratings yet
- ME-52023 Internal Combustion Engines: Technological University (Hmawbi) Department of Mechanical EngineeringDocument25 pagesME-52023 Internal Combustion Engines: Technological University (Hmawbi) Department of Mechanical EngineeringSi Thu Aung100% (1)
- Roygbiv Love, Simon: Troye SivanDocument6 pagesRoygbiv Love, Simon: Troye SivanJuliana AbanadorNo ratings yet
- Unit-4 A2Document18 pagesUnit-4 A2ismaeel247No ratings yet
- CIS Electrical Standard Rev 001Document46 pagesCIS Electrical Standard Rev 001Tarek AbulailNo ratings yet
- The Relationship Between Self-Concept and Academic AchievementDocument63 pagesThe Relationship Between Self-Concept and Academic Achievementڤوتري جنتايوNo ratings yet
- Kirloskar Brothers LimitedDocument36 pagesKirloskar Brothers Limitedgopalakrishnannrm1202No ratings yet
- TC PRR021 51309288 225 DatasheetDocument133 pagesTC PRR021 51309288 225 DatasheetSalim MohamedNo ratings yet
- The Role of The Individual in The Coming Era of Process-Based Therapy (Articulo Examen Final)Document14 pagesThe Role of The Individual in The Coming Era of Process-Based Therapy (Articulo Examen Final)Cristian Steven Cabezas JoyaNo ratings yet
- Clariant - Hydroperm RPU New Liq C - FTDocument4 pagesClariant - Hydroperm RPU New Liq C - FTAna AntunesNo ratings yet
- AREVA T&D Product RangeDocument10 pagesAREVA T&D Product RangeEduardo SolanoNo ratings yet
- Business Name Mobile Number AddressDocument6 pagesBusiness Name Mobile Number AddressAbhedya JakkanwarNo ratings yet
- Exam - DRRRDocument3 pagesExam - DRRRmycah hagadNo ratings yet
- Santosh - Sep - 2021Document1 pageSantosh - Sep - 2021santoshkumarNo ratings yet
- NO Nama Obat Satua N Harga E-Katalog PT Bernofarm (Diskon) PT Mahakam PT Fahrenheit/ Yarindo (Diskon) PT Dexa MedikaDocument3 pagesNO Nama Obat Satua N Harga E-Katalog PT Bernofarm (Diskon) PT Mahakam PT Fahrenheit/ Yarindo (Diskon) PT Dexa MedikaAyu Agnesia PutriNo ratings yet
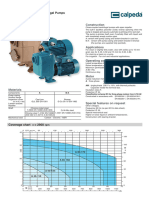
- 1 - A 40-110A - B Self-Priming Centrifugal PumpDocument6 pages1 - A 40-110A - B Self-Priming Centrifugal Pump3dpshabbirNo ratings yet
- Recount Text MATERI X TSM 3 TGL 142019Document3 pagesRecount Text MATERI X TSM 3 TGL 142019smkn 8 jemberNo ratings yet
- Engl FulllDocument27 pagesEngl FullljamesisaiahlallaNo ratings yet
- Sem - Ii Pharmacology Lab ManualDocument36 pagesSem - Ii Pharmacology Lab ManualLokesh MahataNo ratings yet
- Exercise Test Weight Reps Set Interval Tonnage Cutoff 1Rm 5Rm Squat Bench Row Press Deadlift Smallest Plates Available Match Prs in Week #Document7 pagesExercise Test Weight Reps Set Interval Tonnage Cutoff 1Rm 5Rm Squat Bench Row Press Deadlift Smallest Plates Available Match Prs in Week #Chelsea ClarkNo ratings yet
- Criminal Justice Reform ActDocument5 pagesCriminal Justice Reform ActDNAinfoNewYork100% (1)
- Plaster of Paris and Other Fracture Immobilizations: Icrc Physiotherapy Reference ManualDocument107 pagesPlaster of Paris and Other Fracture Immobilizations: Icrc Physiotherapy Reference ManualNur Anish Amira SalimNo ratings yet