Download as pdf or txt
You might also like
- Introduction To Wireline Log Analysis, Baker Atlas, 2002Document321 pagesIntroduction To Wireline Log Analysis, Baker Atlas, 2002Anonymous Xy309m9Sm967% (3)
- Predmaint UgDocument620 pagesPredmaint UgAhad MunawarNo ratings yet
- Blind Flange Design Calculation As Per Asme Section Vii Division - 1Document4 pagesBlind Flange Design Calculation As Per Asme Section Vii Division - 1mukesh100% (2)
- Insulinom PDFDocument11 pagesInsulinom PDFverdi33No ratings yet
- AACE Clinical Case ReportsDocument4 pagesAACE Clinical Case ReportsShuaib AhmedNo ratings yet
- Insulinoma de Páncreas Que Imita EpilepsiaDocument6 pagesInsulinoma de Páncreas Que Imita EpilepsiaSergio Andres Siado GuerreroNo ratings yet
- Case Presentation - 3Document27 pagesCase Presentation - 3AmalNo ratings yet
- ClarezaDocument6 pagesClarezaDinda SaviraNo ratings yet
- He 2001Document8 pagesHe 2001afifahridhahumairahhNo ratings yet
- Tubular Ileal Duplication Causing Small Bowel Obstruction in A ChildDocument5 pagesTubular Ileal Duplication Causing Small Bowel Obstruction in A ChildDiego Leonardo Herrera OjedaNo ratings yet
- Case Report 3Document4 pagesCase Report 3Fika Wilda AnggraeniNo ratings yet
- Cancer - June 1979 - Diasio - Adenocarcinoma of The Pancreas Associated With Hypoglycemia Case Report and Review of TheDocument8 pagesCancer - June 1979 - Diasio - Adenocarcinoma of The Pancreas Associated With Hypoglycemia Case Report and Review of Theabdullah shamshirNo ratings yet
- AACE Clinical Case Reports: Nami Safai Haeri, MD, Hussain Mahmud, MD, Mary T. Korytkowski, MDDocument3 pagesAACE Clinical Case Reports: Nami Safai Haeri, MD, Hussain Mahmud, MD, Mary T. Korytkowski, MDShuaib AhmedNo ratings yet
- Zhang Et Al - 2019 - Subacute Combined Degeneration, Pernicious Anemia and Gastric NeuroendocrineDocument4 pagesZhang Et Al - 2019 - Subacute Combined Degeneration, Pernicious Anemia and Gastric NeuroendocrineJuli Dwi PrasetyonoNo ratings yet
- Jejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of LiteratureDocument6 pagesJejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of Literatureellya theresiaNo ratings yet
- AACE Clinical Case Reports: Ebtihal Y. Alyusuf, MBBS, Aishah A. Ekhzaimy, MD, Juan A. Rivera, MDDocument5 pagesAACE Clinical Case Reports: Ebtihal Y. Alyusuf, MBBS, Aishah A. Ekhzaimy, MD, Juan A. Rivera, MDalingh98No ratings yet
- Management of Aplastic Anemia in PregnancyDocument4 pagesManagement of Aplastic Anemia in PregnancyAhmad NajmiNo ratings yet
- Journal of DiabetesDocument6 pagesJournal of DiabetesSartika Rizky HapsariNo ratings yet
- Perioperative Anesthetic Management of Intestinal Pseudo-Obstruction As A Complication of PheochromocytomaDocument4 pagesPerioperative Anesthetic Management of Intestinal Pseudo-Obstruction As A Complication of Pheochromocytomaceneh5695weizixu.com xNo ratings yet
- Idiopathic Giant Pancreatic PseudocystDocument5 pagesIdiopathic Giant Pancreatic PseudocystRoxana ElenaNo ratings yet
- Congenital Hyperinsulinism of The Newborn: A Case ReportDocument6 pagesCongenital Hyperinsulinism of The Newborn: A Case ReportEdi SetiawanNo ratings yet
- Peritoneal Tuberculosis: The Great Mimicker: Case StudyDocument5 pagesPeritoneal Tuberculosis: The Great Mimicker: Case StudyDumitru RadulescuNo ratings yet
- Pi Is 0272638698001097Document6 pagesPi Is 0272638698001097Mita AdrianiNo ratings yet
- Acitrom Induced Pseudo-Obstruction A Case ReportDocument2 pagesAcitrom Induced Pseudo-Obstruction A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Medicine: Refractory Hyponatremia in Neuromyelitis Optica in A Pediatric PatientDocument4 pagesMedicine: Refractory Hyponatremia in Neuromyelitis Optica in A Pediatric PatientMesan KoNo ratings yet
- GlucagonomaDocument5 pagesGlucagonomacarloshgmedeirosNo ratings yet
- Case Study 39-Year-Old Women Diagnosed As Solitary Rectal Ulcer SyndromeDocument5 pagesCase Study 39-Year-Old Women Diagnosed As Solitary Rectal Ulcer SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1999-07 - Intraductal Papillary-Mucinous Tumor of The Pancreas - Presentation in A Young Adult PDFDocument4 pages1999-07 - Intraductal Papillary-Mucinous Tumor of The Pancreas - Presentation in A Young Adult PDFNawzad SulayvaniNo ratings yet
- Sindrom Nefrotik CairanDocument4 pagesSindrom Nefrotik CairanNanang ApriyantoNo ratings yet
- Gi 1Document3 pagesGi 1Syifa' FauziyahNo ratings yet
- 28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDocument5 pages28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDesi HutapeaNo ratings yet
- en Papilla Vaters Tumor in Elderly An InterDocument5 pagesen Papilla Vaters Tumor in Elderly An InterAyip Bahsan AlBantaniNo ratings yet
- P0710 1116 Acute Liver Failure Due To Severe.767Document1 pageP0710 1116 Acute Liver Failure Due To Severe.767Marselya GaniNo ratings yet
- Case 101Document14 pagesCase 101Marj MendezNo ratings yet
- Frantz TumorDocument5 pagesFrantz TumorAndu1991No ratings yet
- Perinatal Transient Myeloproliferative Disorder in Trisomy 21Document11 pagesPerinatal Transient Myeloproliferative Disorder in Trisomy 21Carina SuarezNo ratings yet
- Calcagno 2018Document10 pagesCalcagno 2018cut normaya putriNo ratings yet
- Acute Appendicitis in A Patient With Systemic Lupus ErythematosusDocument4 pagesAcute Appendicitis in A Patient With Systemic Lupus ErythematosusJessicaNo ratings yet
- Case Report: Scleredema Diabeticorum in A Patient With Type 2 Diabetes MellitusDocument5 pagesCase Report: Scleredema Diabeticorum in A Patient With Type 2 Diabetes MellitusKerin ArdyNo ratings yet
- Pregnancy Complicated by Abdominopelvic Hydatid Disease: Shakun Tyagi, Chanchal Singh, Reva Tripathi, Yedla MalaDocument3 pagesPregnancy Complicated by Abdominopelvic Hydatid Disease: Shakun Tyagi, Chanchal Singh, Reva Tripathi, Yedla MalaMohamed KamalNo ratings yet
- Primary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportDocument6 pagesPrimary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportRais KhairuddinNo ratings yet
- Tumor - Duodenal - 2022Document4 pagesTumor - Duodenal - 2022Berenice SanchezNo ratings yet
- Gallbladder Carcinoma Presenting As Right Upper Quadrant Pain: A Case ReportDocument19 pagesGallbladder Carcinoma Presenting As Right Upper Quadrant Pain: A Case ReportMacky YongcoNo ratings yet
- 5551 13868 1 PBDocument6 pages5551 13868 1 PBNanaNo ratings yet
- Multiple Episodes of Hypoglycemia Secondary To An Insulinoma Case ReportDocument4 pagesMultiple Episodes of Hypoglycemia Secondary To An Insulinoma Case ReportmiguelNo ratings yet
- 18 9513 IngDocument2 pages18 9513 Inggizem özcanNo ratings yet
- Unusual Presentation of Pancreatic Insulinoma:a Case ReportDocument5 pagesUnusual Presentation of Pancreatic Insulinoma:a Case ReportIJAR JOURNALNo ratings yet
- E Posters PDFDocument349 pagesE Posters PDFpriyadikkalaNo ratings yet
- 1 PBDocument3 pages1 PBMartynaNo ratings yet
- Acute Fatty Liver of Pregnancy: Rare, But Potentially FatalDocument4 pagesAcute Fatty Liver of Pregnancy: Rare, But Potentially FataleeeeeeNo ratings yet
- Diagnosis and Management of Klatskin Tumor: April 2010Document6 pagesDiagnosis and Management of Klatskin Tumor: April 2010Feby Kurnia PutriNo ratings yet
- Hepatic Glycogenosis Associated With Type 1 Diabetes (A Case Report)Document5 pagesHepatic Glycogenosis Associated With Type 1 Diabetes (A Case Report)IJAR JOURNALNo ratings yet
- Submandibular Gland Excision Submandibular Gland Excision Submandibular Gland Excision Submandibular Gland Excision Submandibular Gland ExcisionDocument4 pagesSubmandibular Gland Excision Submandibular Gland Excision Submandibular Gland Excision Submandibular Gland Excision Submandibular Gland ExcisionmawarmelatiNo ratings yet
- Severe Complications of Chronic Cholelithiasis TreatmentDocument8 pagesSevere Complications of Chronic Cholelithiasis Treatmentabraham suarezNo ratings yet
- Ogilvie Syndrome After Emergency Cesarean Section: A Case ReportDocument4 pagesOgilvie Syndrome After Emergency Cesarean Section: A Case ReportIJAR JOURNALNo ratings yet
- A Rare and Fatal Case of Nasogastric Tube.492Document1 pageA Rare and Fatal Case of Nasogastric Tube.492Stefania Szeibert-KerekesNo ratings yet
- Mucinous Neoplasm of Appendix TreatmentDocument3 pagesMucinous Neoplasm of Appendix TreatmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2022 Parathyroid Carcinoma All-In-One, A Rare Life-Threatening Case With Multiple Systemic Manifestations Case Report and Review of The LiteratureDocument12 pages2022 Parathyroid Carcinoma All-In-One, A Rare Life-Threatening Case With Multiple Systemic Manifestations Case Report and Review of The LiteratureCharley WangNo ratings yet
- Mastoiditis Jurnal 2.Document4 pagesMastoiditis Jurnal 2.fahrizan atjoNo ratings yet
- Review On Enterocutaneous FistulaDocument31 pagesReview On Enterocutaneous FistulaAbu ZidaneNo ratings yet
- 19Document3 pages19Elizabeth ToapantaNo ratings yet
- en Choledocholithiasis During Pregnancy MulDocument6 pagesen Choledocholithiasis During Pregnancy MulJuan SlaxNo ratings yet
- Emergencies in Diabetes: Diagnosis, Management and PreventionFrom EverandEmergencies in Diabetes: Diagnosis, Management and PreventionNo ratings yet
- 18 - Fatema AlSaliti - Thyroid - Graves' DiseaseDocument1 page18 - Fatema AlSaliti - Thyroid - Graves' Diseasemohammed makkiNo ratings yet
- Section 2: Insulin Therapy in Type 1 and Type 2 DiabetesDocument48 pagesSection 2: Insulin Therapy in Type 1 and Type 2 Diabetesmohammed makkiNo ratings yet
- Counting Carbohydrates and Dosing Insulin For School Nurses: Presented byDocument26 pagesCounting Carbohydrates and Dosing Insulin For School Nurses: Presented bymohammed makkiNo ratings yet
- 19 - Abdul Aziz - Thyroid - Metastatic Differentiated Thyroid Carcinoma (Poster)Document1 page19 - Abdul Aziz - Thyroid - Metastatic Differentiated Thyroid Carcinoma (Poster)mohammed makkiNo ratings yet
- Pathogenesis and Treatment of Renal Osteodystrophy: Eduardo Slatopolsky Esther Gonzalez Kevin MartinDocument9 pagesPathogenesis and Treatment of Renal Osteodystrophy: Eduardo Slatopolsky Esther Gonzalez Kevin Martinmohammed makkiNo ratings yet
- AACE TRC Interpretation of TFTs Part 3-FINALDocument31 pagesAACE TRC Interpretation of TFTs Part 3-FINALmohammed makkiNo ratings yet
- 46 - Abdullah Al Sabahi - Thyroid Disease - Subacute Thyroiditis PosterDocument1 page46 - Abdullah Al Sabahi - Thyroid Disease - Subacute Thyroiditis Postermohammed makkiNo ratings yet
- 14 - Nadjib Kaouache - Thyroid - CARDIOMETABOLIC RISK FACTORS IN A COHORT OFDocument1 page14 - Nadjib Kaouache - Thyroid - CARDIOMETABOLIC RISK FACTORS IN A COHORT OFmohammed makkiNo ratings yet
- GD in PregnancyDocument37 pagesGD in Pregnancymohammed makkiNo ratings yet
- 59 - Lynda Belabas - Thyroid Disease - Gaed Poster Family PDFDocument1 page59 - Lynda Belabas - Thyroid Disease - Gaed Poster Family PDFmohammed makkiNo ratings yet
- Hypothyrodism in PregnancyDocument32 pagesHypothyrodism in Pregnancymohammed makki0% (1)
- TabernacleDocument126 pagesTabernacleVal100% (8)
- Best Practice Guide 2021Document14 pagesBest Practice Guide 2021Azme Pak LangNo ratings yet
- APM-2024 FlyerDocument2 pagesAPM-2024 FlyeracryptfauNo ratings yet
- Biodiesel Pilot PlatDocument30 pagesBiodiesel Pilot PlatKhairul AnwarNo ratings yet
- Inflatable Packers and GroutingDocument7 pagesInflatable Packers and GroutingjasonlaiymNo ratings yet
- D-155 D-179 D-206 D-239 D-246 D-268 D-310 D-358 DT-239 DT-358 DT-402 Electrical EquipmentDocument52 pagesD-155 D-179 D-206 D-239 D-246 D-268 D-310 D-358 DT-239 DT-358 DT-402 Electrical EquipmentTanase MariusNo ratings yet
- Seamo Paper - F - 2021Document8 pagesSeamo Paper - F - 2021Bá PhongNo ratings yet
- Micom P438: Rail Catenary Protection Device P438/En M/Cf8Document652 pagesMicom P438: Rail Catenary Protection Device P438/En M/Cf8Peng GuoNo ratings yet
- Congestive Heart Failure PathophysiologyDocument7 pagesCongestive Heart Failure PathophysiologyAileen Grace RodrigoNo ratings yet
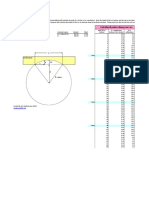
- Arc Layout Calculator: Calculated Points Along Your Arc Enter These ValuesDocument1 pageArc Layout Calculator: Calculated Points Along Your Arc Enter These ValuesPaco PacoNo ratings yet
- Development of 1 Phase of Master Plan at Mormugao Port: Final Feasibility ReportDocument173 pagesDevelopment of 1 Phase of Master Plan at Mormugao Port: Final Feasibility ReportMinh TríNo ratings yet
- Alternators Starters PDFDocument1,346 pagesAlternators Starters PDFДима СелютинNo ratings yet
- Contador Frecuencia 1-50Document4 pagesContador Frecuencia 1-50jose100% (2)
- English 7: Part I: Age of InnocenceDocument4 pagesEnglish 7: Part I: Age of InnocenceAngelNicolinE.SuymanNo ratings yet
- Goulds Pumps: Engineered For LifeDocument6 pagesGoulds Pumps: Engineered For LifeJeffersonGutiérrezNo ratings yet
- A Systemic Review of Functional Near-Infrared Spectroscopy For Stroke: Current Application and Future DirectionsDocument14 pagesA Systemic Review of Functional Near-Infrared Spectroscopy For Stroke: Current Application and Future DirectionsEricNo ratings yet
- Catia Important Interview QuestionsDocument40 pagesCatia Important Interview QuestionsHarshwardhan Singh0% (1)
- Chaitanya Bharati Institute of Technology (A) CED Question Bank-HWRE (18CEC25) Unit-1Document12 pagesChaitanya Bharati Institute of Technology (A) CED Question Bank-HWRE (18CEC25) Unit-1AKHILA UMMANAVENANo ratings yet
- Chapter 4 Final Impression FinalDocument19 pagesChapter 4 Final Impression FinalMohammed AsfourNo ratings yet
- Stochastic ProcessDocument610 pagesStochastic ProcesshopanzNo ratings yet
- Scapular Dyskinesis Its Relation To Shoulder PainDocument21 pagesScapular Dyskinesis Its Relation To Shoulder PainTamas KalmarNo ratings yet
- Berger Paint ProjectDocument144 pagesBerger Paint ProjectMukesh Kumar100% (2)
- Safety Data Sheet: Section 1: Identification of The Substance/Mixture and of The Company/UndertakingDocument10 pagesSafety Data Sheet: Section 1: Identification of The Substance/Mixture and of The Company/UndertakingIsmael Enrique ArciniegasNo ratings yet
- S5 10-11 Math Yearly Exam Paper 2Document12 pagesS5 10-11 Math Yearly Exam Paper 2Shao Jiaren (Jwss)No ratings yet
- Lexmark C500 Menus and MessagesDocument15 pagesLexmark C500 Menus and MessagesjcontractorNo ratings yet
- (FHWA, 2016) - Highway Performance Monitoring System, Field ManualDocument295 pages(FHWA, 2016) - Highway Performance Monitoring System, Field Manualali faresNo ratings yet
- The Effect of Heat Treatment On The Hardness and Impact Properties of Medium Carbon SteelDocument10 pagesThe Effect of Heat Treatment On The Hardness and Impact Properties of Medium Carbon SteelSoumyadipNo ratings yet