Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Reproductive - Systems - in - Vertebrates ss2Document12 pagesReproductive - Systems - in - Vertebrates ss2Ezeh Princess100% (1)
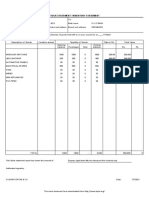
- Stock Statement Format For Bank LoanDocument1 pageStock Statement Format For Bank Loanpsycho Neha40% (5)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- IP391 - 2007 - Determination of Aromatic Hydrocarbon Types in Middle Distillates - High Performance Liquid Chromatography Method With Refractive Index Detection (RID)Document12 pagesIP391 - 2007 - Determination of Aromatic Hydrocarbon Types in Middle Distillates - High Performance Liquid Chromatography Method With Refractive Index Detection (RID)Constantinos ChristodoulouNo ratings yet
- Dsme Piping - Practice PDFDocument117 pagesDsme Piping - Practice PDFJesus PlacedesNo ratings yet
- QEG Opensourced Build Manual 25-Mar-15Document76 pagesQEG Opensourced Build Manual 25-Mar-15Naicheval RobitaiNo ratings yet
- Drone Study PDFDocument54 pagesDrone Study PDFMihaela Azamfirei100% (1)
- POM Class 1 For MD7-2Document2 pagesPOM Class 1 For MD7-2brown_chocolate87643No ratings yet
- PBL2Document12 pagesPBL2brown_chocolate87643No ratings yet
- Normocytic Anemia'sDocument14 pagesNormocytic Anemia'sbrown_chocolate87643No ratings yet
- Nimesulide Patients Still Exposed To A Risk of Severe HepatitisDocument2 pagesNimesulide Patients Still Exposed To A Risk of Severe Hepatitisbrown_chocolate87643No ratings yet
- Cape MCQ 08-13Document51 pagesCape MCQ 08-13brown_chocolate87643No ratings yet
- Phil Must Be Asked For Permission To Sample Blood For A HCV and HIV Test. If He Refuses Then It Must Be Assumed He Is A Carrier of The VirusDocument3 pagesPhil Must Be Asked For Permission To Sample Blood For A HCV and HIV Test. If He Refuses Then It Must Be Assumed He Is A Carrier of The Virusbrown_chocolate87643No ratings yet
- Ghouls Bhowling Alley Kiss of Death Wiked Cricket Grab Bag and More!!!Document2 pagesGhouls Bhowling Alley Kiss of Death Wiked Cricket Grab Bag and More!!!brown_chocolate87643No ratings yet
- Real Comm Studies IA-2Document7 pagesReal Comm Studies IA-2brown_chocolate87643No ratings yet
- Communication Skills 11 ExaminationDocument8 pagesCommunication Skills 11 Examinationbrown_chocolate87643No ratings yet
- Question 3 Micro B-2Document3 pagesQuestion 3 Micro B-2brown_chocolate87643No ratings yet
- AAIMS INVITATION - 4th Anniversary LectureDocument1 pageAAIMS INVITATION - 4th Anniversary Lecturebrown_chocolate87643No ratings yet
- Summer Course 2014 FlyerDocument1 pageSummer Course 2014 Flyerbrown_chocolate87643No ratings yet
- Anemias: Table Showing Types of Anemias and Causes Reticulocyte Count Microcytic Normocytic Macrocytic LOWDocument4 pagesAnemias: Table Showing Types of Anemias and Causes Reticulocyte Count Microcytic Normocytic Macrocytic LOWbrown_chocolate87643No ratings yet
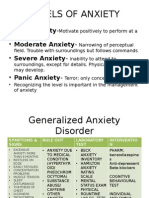
- Levels of Anxiety: - Mild Anxiety - Moderate Anxiety - Severe Anxiety - Panic AnxietyDocument4 pagesLevels of Anxiety: - Mild Anxiety - Moderate Anxiety - Severe Anxiety - Panic Anxietybrown_chocolate87643No ratings yet
- Case 34Document10 pagesCase 34brown_chocolate87643No ratings yet
- Mass in Epigastrium-2Document37 pagesMass in Epigastrium-2brown_chocolate87643100% (1)
- Sports DayDocument4 pagesSports Daybrown_chocolate87643No ratings yet
- Global Ethical Issues Unit 3Document15 pagesGlobal Ethical Issues Unit 3aditi anandNo ratings yet
- AdaptiveAndLearningSystems TheoryAndApplications KumpatiSNarendraDocument410 pagesAdaptiveAndLearningSystems TheoryAndApplications KumpatiSNarendraSooperAktifNo ratings yet
- Greenboro Polychem PVT LTDDocument57 pagesGreenboro Polychem PVT LTDMehdi MadaniNo ratings yet
- BO0008 - Kixx LUBO 150BS - EngDocument9 pagesBO0008 - Kixx LUBO 150BS - EngkokoNo ratings yet
- 4TM1 and 2 Jan 24 PresentersDocument8 pages4TM1 and 2 Jan 24 PresentersMark QuizonNo ratings yet
- Daily ReportDocument3 pagesDaily ReportJoseph AbousafiNo ratings yet
- U5 SCMDocument48 pagesU5 SCMbhathrinaathan16No ratings yet
- Grade 5 DLL SCIENCE 5 Q3 Week 10Document4 pagesGrade 5 DLL SCIENCE 5 Q3 Week 10Leonardo Bruno Jr100% (4)
- E Exe Ef Fluorescent: Standard S Specification FeaturesDocument4 pagesE Exe Ef Fluorescent: Standard S Specification FeaturesrelaxjackNo ratings yet
- Chapter2 PDFDocument18 pagesChapter2 PDFshaik jaheerNo ratings yet
- Diagrama Isb 6 7 cm2150 SN PDFDocument17 pagesDiagrama Isb 6 7 cm2150 SN PDFJunior de CantilloNo ratings yet
- Plumbing Pipe and Fitting SymbolsDocument8 pagesPlumbing Pipe and Fitting Symbolsburhansucipto0% (1)
- The Grand MultiparaDocument5 pagesThe Grand MultiparaIndhumathiNo ratings yet
- Control Electrical Appliances Using PCDocument46 pagesControl Electrical Appliances Using PCsumit gandhi100% (1)
- What Is Pure Substance?: Pure Substances Are Substances That Are Made Up of Only One Kind ofDocument3 pagesWhat Is Pure Substance?: Pure Substances Are Substances That Are Made Up of Only One Kind ofNi Made FebrianiNo ratings yet
- Dyna 86l 8086 P Training Development System With LCD PDFDocument1 pageDyna 86l 8086 P Training Development System With LCD PDFSoluchanNo ratings yet
- Clanbook Tremere (Revised Edition) (2000) WW2357 (With Bookmarks) (OEF)Document107 pagesClanbook Tremere (Revised Edition) (2000) WW2357 (With Bookmarks) (OEF)cwod100% (1)
- Alcium LAT Late: 256-1800ah 0.613 - 5.248kWDocument4 pagesAlcium LAT Late: 256-1800ah 0.613 - 5.248kWJunior Ramirez ReyesNo ratings yet
- Electrical Troubleshooting ManualDocument52 pagesElectrical Troubleshooting ManualMohammed Shdiefat100% (1)
- P2P Paths With Djikstra's AlgorithmDocument8 pagesP2P Paths With Djikstra's AlgorithmNouman AfzalNo ratings yet
- The Scientific WorkDocument24 pagesThe Scientific WorkhumanNo ratings yet
- The One Ring™ Character LifepathsDocument10 pagesThe One Ring™ Character LifepathsDave SatterthwaiteNo ratings yet
- Atomic Structure: Name: Mr. Burnett Date: 03/05/2021 Class: 6A PhysicsDocument50 pagesAtomic Structure: Name: Mr. Burnett Date: 03/05/2021 Class: 6A PhysicsACSVNo ratings yet
- MSDS Diamond Paste (Metprep)Document3 pagesMSDS Diamond Paste (Metprep)Claudia MmsNo ratings yet