
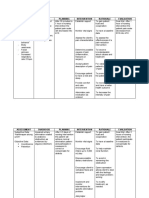
CS5 (AGE) Acute Gastroenteritis NCP
CS5 (AGE) Acute Gastroenteritis NCP
You might also like
- Airline Cabin Crew Training IATA Training Course PDFDocument3 pagesAirline Cabin Crew Training IATA Training Course PDFwin computer0% (1)
- Se 5000英文Amanual PDFDocument73 pagesSe 5000英文Amanual PDFbandi ismail100% (1)
- Surgical Gowning and GlovingDocument36 pagesSurgical Gowning and GlovingAudrie Allyson GabalesNo ratings yet
- Colorectal Cancer Patient DataDocument3 pagesColorectal Cancer Patient DataAudrie Allyson GabalesNo ratings yet
- Health TeachingsDocument7 pagesHealth Teachingstheamacias100% (2)
- OutSystems 10 Professional Developer CertificationDocument4 pagesOutSystems 10 Professional Developer CertificationhanspaulNo ratings yet
- BWT Septron Line 31-61 Rev01!08!05-18 Opm enDocument56 pagesBWT Septron Line 31-61 Rev01!08!05-18 Opm enDavide Grioni100% (1)
- Observation StatementDocument3 pagesObservation Statementapi-241848470No ratings yet
- History of U.S. Table Tennis - Vol. VI: 1970-1973Document506 pagesHistory of U.S. Table Tennis - Vol. VI: 1970-1973Tim Boggan100% (2)
- Evidence Part IDocument10 pagesEvidence Part IVitz IgotNo ratings yet
- DRUG STUDY (Appendicitis)Document14 pagesDRUG STUDY (Appendicitis)Jobelle AcenaNo ratings yet
- Case Study - AGE With Some DHNDocument19 pagesCase Study - AGE With Some DHNJessica Mae Abaquita-javierNo ratings yet
- Drug Name Action Dose & Route Side Effects Nursing Care Brand Name: Twynsta Generic: Telmisartan + AmlodipineDocument4 pagesDrug Name Action Dose & Route Side Effects Nursing Care Brand Name: Twynsta Generic: Telmisartan + AmlodipineEileenAquinoMacapagalNo ratings yet
- Acute GastroenteritisDocument2 pagesAcute GastroenteritisErika CadawanNo ratings yet
- Drug Study of CiprofloxacinDocument3 pagesDrug Study of CiprofloxacinZyra MendozaNo ratings yet
- Hyperthermia Pneumonia Nursing Care PlanDocument1 pageHyperthermia Pneumonia Nursing Care PlanLegendX100% (1)
- Name and Classification of Drug Mechanism of Action Adverse Effects Nursing Responsibility Keto-Analogues + EAA Trade NameDocument2 pagesName and Classification of Drug Mechanism of Action Adverse Effects Nursing Responsibility Keto-Analogues + EAA Trade NameKrizha Angela NicolasNo ratings yet
- NCP ErDocument4 pagesNCP ErljarseniornNo ratings yet
- NCP M7Document3 pagesNCP M7rjalavazo1989No ratings yet
- Drug Study - OB WardDocument8 pagesDrug Study - OB WardCheska YsabelleNo ratings yet
- Pathophysiology of PneumoniaDocument4 pagesPathophysiology of PneumoniaDimpal ChoudharyNo ratings yet
- DibencozideDocument1 pageDibencozideParsley Non100% (2)
- Nursing Care Plan: Histolytica, ADocument4 pagesNursing Care Plan: Histolytica, AkristennemarieNo ratings yet
- SNU49Document2 pagesSNU49Nora BacolNo ratings yet
- NCP GastroenteritisDocument1 pageNCP GastroenteritisFranchesca PaunganNo ratings yet
- Nursing Care Plan For InflammationDocument2 pagesNursing Care Plan For InflammationJobelle AcenaNo ratings yet
- Nursing Care Plan Urinary Tract Infection UTIDocument2 pagesNursing Care Plan Urinary Tract Infection UTITrida Hermano CabansagNo ratings yet
- Age NCPDocument4 pagesAge NCPnj_pink081794No ratings yet
- Tramadol UltramDocument2 pagesTramadol UltramatchiekNo ratings yet
- Nahco3 Vancomycin AmlodipineDocument3 pagesNahco3 Vancomycin AmlodipineShan Dave TupasNo ratings yet
- Nursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NDocument2 pagesNursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NnananaNo ratings yet
- NCP Acute Pain-HyperthermiaDocument6 pagesNCP Acute Pain-HyperthermiarhegellNo ratings yet
- Drug Study NaclDocument3 pagesDrug Study NaclNicole Denise PortugalezaNo ratings yet
- Acc Phu Case NCP HyperthermiaDocument1 pageAcc Phu Case NCP Hyperthermiamacy_bautistaNo ratings yet
- Health Teaching Plan Acute Gastroenteritis - Deficient Fluid VolumeDocument4 pagesHealth Teaching Plan Acute Gastroenteritis - Deficient Fluid VolumeAngelica Mateo100% (2)
- NCP (Crohn's Disease)Document13 pagesNCP (Crohn's Disease)Jay Jay JayyiNo ratings yet
- Pathophysiology AGEDocument2 pagesPathophysiology AGEMareeze Hatta100% (1)
- Nursing Care Plan For Tissue InjuryDocument2 pagesNursing Care Plan For Tissue InjuryJobelle AcenaNo ratings yet
- Sine CodDocument2 pagesSine CodshayneNo ratings yet
- MannitolDocument1 pageMannitolAina HaravataNo ratings yet
- Assessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationDocument6 pagesAssessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationimnasNo ratings yet
- NCP NephrolithiasisDocument3 pagesNCP NephrolithiasisMANUEL EMERSONNo ratings yet
- NCP LatestDocument6 pagesNCP LatestThirdy AquinoNo ratings yet
- Bacillus Clausii ErcefloraDocument1 pageBacillus Clausii ErcefloraCezhille BattadNo ratings yet
- Pathophysiology of Acute GastroenteritisDocument1 pagePathophysiology of Acute GastroenteritisAlliah Grejie AnneNo ratings yet
- NCP HyperthermiaDocument1 pageNCP HyperthermiaPastor James PacadaljenNo ratings yet
- Chronic Renal Failure Nursing Care PlanDocument6 pagesChronic Renal Failure Nursing Care PlanRuva Oscass JimmyNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Hepatitis A PDFDocument2 pagesNursingcrib Com NURSING CARE PLAN Hepatitis A PDFswapnilazarusNo ratings yet
- Patty NCP HyperthermiaDocument4 pagesPatty NCP HyperthermiaPatricia Jean FaeldoneaNo ratings yet
- Pa Tho Physiology of Acute GastroenteritisDocument2 pagesPa Tho Physiology of Acute Gastroenteritisromeo rivera100% (16)
- Case Study BkaDocument92 pagesCase Study BkaMaria CabangonNo ratings yet
- BNP (C)Document2 pagesBNP (C)Mae Ann Bueno CastillonNo ratings yet
- NCP of MGH PatientDocument2 pagesNCP of MGH PatientMaverick LimNo ratings yet
- Pa Tho Physiology of AchalasiaDocument1 pagePa Tho Physiology of AchalasiaSewyel GarburiNo ratings yet
- Drug Name Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesDocument4 pagesDrug Name Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibilitiesangel cenaNo ratings yet
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- Volume 1Document2 pagesVolume 1roxybiscanteNo ratings yet
- Ate Gabs Nyo Pagod NaDocument3 pagesAte Gabs Nyo Pagod NaGabrielle EvangelistaNo ratings yet
- Fluid Volume Deficit Related To Nausea and VomitDocument3 pagesFluid Volume Deficit Related To Nausea and VomitJakeNo ratings yet
- Deficient Fluid Volume (AGEDocument2 pagesDeficient Fluid Volume (AGENursesLabs.com83% (6)
- Subjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Document5 pagesSubjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Erle Gray CadangenNo ratings yet
- NCP Deficit Fluid VolumeDocument4 pagesNCP Deficit Fluid VolumeKingJayson Pacman06No ratings yet
- Fluid Volume Deficit Related To Loose Watery Stool Diarrhea)Document2 pagesFluid Volume Deficit Related To Loose Watery Stool Diarrhea)Jesse James Advincula Edjec100% (15)
- Assessment Explanation of The Problem Objective Intervention Rationale Evaluation Subjective: Objective: Sto: DX StoDocument2 pagesAssessment Explanation of The Problem Objective Intervention Rationale Evaluation Subjective: Objective: Sto: DX StoBasema HashhashNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Scientific Background Planning Implementation Rationale EvaluationDocument3 pagesNursing Care Plan: Assessment Nursing Diagnosis Scientific Background Planning Implementation Rationale EvaluationMelrhean GraceNo ratings yet
- Case #2 Nursing Care PlanDocument2 pagesCase #2 Nursing Care PlanPauline AñesNo ratings yet
- Risk NCP - PESCADERO 4CDocument1 pageRisk NCP - PESCADERO 4COrlando VillanuevaNo ratings yet
- NCP-Fluid Volume DeficitDocument2 pagesNCP-Fluid Volume Deficitanon_207994234100% (1)
- Assessment Nursing Diagnosis Planning Intervention Evaluation ObjectivesDocument4 pagesAssessment Nursing Diagnosis Planning Intervention Evaluation Objectivesashamy acolNo ratings yet
- 3rd Year Nursing RESEARCH MIDTERM QUIZESDocument3 pages3rd Year Nursing RESEARCH MIDTERM QUIZESAudrie Allyson GabalesNo ratings yet
- CS6 Alzheimer DiseaseDocument21 pagesCS6 Alzheimer DiseaseAudrie Allyson GabalesNo ratings yet
- 3rd Year Nursing MS LEC MIDTERM QUIZESDocument18 pages3rd Year Nursing MS LEC MIDTERM QUIZESAudrie Allyson GabalesNo ratings yet
- CS6 Alzheimer's Disease Drug StudyDocument3 pagesCS6 Alzheimer's Disease Drug StudyAudrie Allyson GabalesNo ratings yet
- Breast Self ExaminationDocument81 pagesBreast Self ExaminationAudrie Allyson Gabales100% (1)
- DISCHARGE PLAN & RRL For Colorectal CancerDocument2 pagesDISCHARGE PLAN & RRL For Colorectal CancerAudrie Allyson GabalesNo ratings yet
- Aag Drug StudyDocument7 pagesAag Drug StudyAudrie Allyson GabalesNo ratings yet
- Diagnostic Prodecures X Ray Utz CT Scan MriecgeegDocument42 pagesDiagnostic Prodecures X Ray Utz CT Scan MriecgeegAudrie Allyson GabalesNo ratings yet
- Drug Study HIVDocument10 pagesDrug Study HIVAudrie Allyson GabalesNo ratings yet
- Week 7 PARENTERAL NUTRITIONDocument51 pagesWeek 7 PARENTERAL NUTRITIONAudrie Allyson GabalesNo ratings yet
- Colorectal Cancer DRUG STUDYDocument12 pagesColorectal Cancer DRUG STUDYAudrie Allyson GabalesNo ratings yet
- CS4 Asthma Drug StudyDocument10 pagesCS4 Asthma Drug StudyAudrie Allyson GabalesNo ratings yet
- Colorectal Cancer NCPDocument6 pagesColorectal Cancer NCPAudrie Allyson GabalesNo ratings yet
- CS5 (AGE) Acute Gastroenteritis DRUG STUDYDocument8 pagesCS5 (AGE) Acute Gastroenteritis DRUG STUDYAudrie Allyson GabalesNo ratings yet
- Nursing Care Plan For PneumoniaDocument2 pagesNursing Care Plan For PneumoniaAudrie Allyson GabalesNo ratings yet
- Defining Characteristics Nursing Diagnosis Outcome Identification Nursing Interventions Rationale EvaluationDocument2 pagesDefining Characteristics Nursing Diagnosis Outcome Identification Nursing Interventions Rationale EvaluationAudrie Allyson GabalesNo ratings yet
- L. N .E.R.-'': and The Silver Jubilee'' TrainDocument3 pagesL. N .E.R.-'': and The Silver Jubilee'' TrainIan FlackNo ratings yet
- 07. ĐỀ THI VÀO LỚP 10-CẦN THƠ (2020-2021)Document8 pages07. ĐỀ THI VÀO LỚP 10-CẦN THƠ (2020-2021)Vương ThànhNo ratings yet
- Chemistry Project On Presence of Insecticides & Pesticides in FDocument8 pagesChemistry Project On Presence of Insecticides & Pesticides in FShaila BhandaryNo ratings yet
- Assam 04092012Document53 pagesAssam 04092012Sahu PraveenNo ratings yet
- Grade Thresholds - June 2023: Cambridge International AS & A Level Thinking Skills (9694)Document2 pagesGrade Thresholds - June 2023: Cambridge International AS & A Level Thinking Skills (9694)rqb7704No ratings yet
- Presentation Geotextile (November 2010)Document22 pagesPresentation Geotextile (November 2010)Gizachew ZelekeNo ratings yet
- Solution-Focused Nursing Rethinking Prac PDFDocument1 pageSolution-Focused Nursing Rethinking Prac PDFSHUMETNo ratings yet
- RESEARCH PROPOSAL Detriorating Standard of Education in PakistanDocument12 pagesRESEARCH PROPOSAL Detriorating Standard of Education in Pakistanjaydee_atc581454% (13)
- Chaff CutterDocument23 pagesChaff CutterFekadie TesfaNo ratings yet
- Introductions To Valuation Methods and Requirements 1672683839Document51 pagesIntroductions To Valuation Methods and Requirements 1672683839v7qksq5bzg100% (1)
- Business ProposalDocument35 pagesBusiness ProposalMJ MacapagalNo ratings yet
- Case Study - SkyworksDocument46 pagesCase Study - SkyworksMohd Fadzli JiFadNo ratings yet
- Advatage and DisadadvatagesDocument5 pagesAdvatage and DisadadvatagesPawan PathakNo ratings yet
- Guidelines and Fundamental Considerations For Axle BalancingDocument40 pagesGuidelines and Fundamental Considerations For Axle BalancingAnonymous PVXBGg9TNo ratings yet
- Mark Scheme: Q Scheme Marks Aos Pearson Progression Step and Progress Descriptor 1 M1Document9 pagesMark Scheme: Q Scheme Marks Aos Pearson Progression Step and Progress Descriptor 1 M1sara jaimeNo ratings yet
- Physics 2018 Prelims NYJC Paper 2Document19 pagesPhysics 2018 Prelims NYJC Paper 2NG KAI EE EMMANUELLE NG KAI EE EMMANUELLENo ratings yet
- Certiport Exam Administration Policies: Examination SecurityDocument2 pagesCertiport Exam Administration Policies: Examination SecurityrajputamitdNo ratings yet
- Light Rail TransitDocument4 pagesLight Rail TransitnalakasaNo ratings yet
- Software Quality Assurance: Lecture # 6Document37 pagesSoftware Quality Assurance: Lecture # 6rabiaNo ratings yet
- Thesis On Mughal ArchitectureDocument5 pagesThesis On Mughal Architecturecarlajardinebellevue100% (2)
- Loop Switching PDFDocument176 pagesLoop Switching PDFshawnr7376No ratings yet
- B NilfiskDocument16 pagesB Nilfiskarjun0188No ratings yet
- 5.00 FD An1 s1 CE Chemistry 23-24Document4 pages5.00 FD An1 s1 CE Chemistry 23-24imsNo ratings yet










































































































Download as doc, pdf, or txt
You might also like
- Airline Cabin Crew Training IATA Training Course PDFDocument3 pagesAirline Cabin Crew Training IATA Training Course PDFwin computer0% (1)
- Se 5000英文Amanual PDFDocument73 pagesSe 5000英文Amanual PDFbandi ismail100% (1)
- Surgical Gowning and GlovingDocument36 pagesSurgical Gowning and GlovingAudrie Allyson GabalesNo ratings yet
- Colorectal Cancer Patient DataDocument3 pagesColorectal Cancer Patient DataAudrie Allyson GabalesNo ratings yet
- Health TeachingsDocument7 pagesHealth Teachingstheamacias100% (2)
- OutSystems 10 Professional Developer CertificationDocument4 pagesOutSystems 10 Professional Developer CertificationhanspaulNo ratings yet
- BWT Septron Line 31-61 Rev01!08!05-18 Opm enDocument56 pagesBWT Septron Line 31-61 Rev01!08!05-18 Opm enDavide Grioni100% (1)
- Observation StatementDocument3 pagesObservation Statementapi-241848470No ratings yet
- History of U.S. Table Tennis - Vol. VI: 1970-1973Document506 pagesHistory of U.S. Table Tennis - Vol. VI: 1970-1973Tim Boggan100% (2)
- Evidence Part IDocument10 pagesEvidence Part IVitz IgotNo ratings yet
- DRUG STUDY (Appendicitis)Document14 pagesDRUG STUDY (Appendicitis)Jobelle AcenaNo ratings yet
- Case Study - AGE With Some DHNDocument19 pagesCase Study - AGE With Some DHNJessica Mae Abaquita-javierNo ratings yet
- Drug Name Action Dose & Route Side Effects Nursing Care Brand Name: Twynsta Generic: Telmisartan + AmlodipineDocument4 pagesDrug Name Action Dose & Route Side Effects Nursing Care Brand Name: Twynsta Generic: Telmisartan + AmlodipineEileenAquinoMacapagalNo ratings yet
- Acute GastroenteritisDocument2 pagesAcute GastroenteritisErika CadawanNo ratings yet
- Drug Study of CiprofloxacinDocument3 pagesDrug Study of CiprofloxacinZyra MendozaNo ratings yet
- Hyperthermia Pneumonia Nursing Care PlanDocument1 pageHyperthermia Pneumonia Nursing Care PlanLegendX100% (1)
- Name and Classification of Drug Mechanism of Action Adverse Effects Nursing Responsibility Keto-Analogues + EAA Trade NameDocument2 pagesName and Classification of Drug Mechanism of Action Adverse Effects Nursing Responsibility Keto-Analogues + EAA Trade NameKrizha Angela NicolasNo ratings yet
- NCP ErDocument4 pagesNCP ErljarseniornNo ratings yet
- NCP M7Document3 pagesNCP M7rjalavazo1989No ratings yet
- Drug Study - OB WardDocument8 pagesDrug Study - OB WardCheska YsabelleNo ratings yet
- Pathophysiology of PneumoniaDocument4 pagesPathophysiology of PneumoniaDimpal ChoudharyNo ratings yet
- DibencozideDocument1 pageDibencozideParsley Non100% (2)
- Nursing Care Plan: Histolytica, ADocument4 pagesNursing Care Plan: Histolytica, AkristennemarieNo ratings yet
- SNU49Document2 pagesSNU49Nora BacolNo ratings yet
- NCP GastroenteritisDocument1 pageNCP GastroenteritisFranchesca PaunganNo ratings yet
- Nursing Care Plan For InflammationDocument2 pagesNursing Care Plan For InflammationJobelle AcenaNo ratings yet
- Nursing Care Plan Urinary Tract Infection UTIDocument2 pagesNursing Care Plan Urinary Tract Infection UTITrida Hermano CabansagNo ratings yet
- Age NCPDocument4 pagesAge NCPnj_pink081794No ratings yet
- Tramadol UltramDocument2 pagesTramadol UltramatchiekNo ratings yet
- Nahco3 Vancomycin AmlodipineDocument3 pagesNahco3 Vancomycin AmlodipineShan Dave TupasNo ratings yet
- Nursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NDocument2 pagesNursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NnananaNo ratings yet
- NCP Acute Pain-HyperthermiaDocument6 pagesNCP Acute Pain-HyperthermiarhegellNo ratings yet
- Drug Study NaclDocument3 pagesDrug Study NaclNicole Denise PortugalezaNo ratings yet
- Acc Phu Case NCP HyperthermiaDocument1 pageAcc Phu Case NCP Hyperthermiamacy_bautistaNo ratings yet
- Health Teaching Plan Acute Gastroenteritis - Deficient Fluid VolumeDocument4 pagesHealth Teaching Plan Acute Gastroenteritis - Deficient Fluid VolumeAngelica Mateo100% (2)
- NCP (Crohn's Disease)Document13 pagesNCP (Crohn's Disease)Jay Jay JayyiNo ratings yet
- Pathophysiology AGEDocument2 pagesPathophysiology AGEMareeze Hatta100% (1)
- Nursing Care Plan For Tissue InjuryDocument2 pagesNursing Care Plan For Tissue InjuryJobelle AcenaNo ratings yet
- Sine CodDocument2 pagesSine CodshayneNo ratings yet
- MannitolDocument1 pageMannitolAina HaravataNo ratings yet
- Assessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationDocument6 pagesAssessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationimnasNo ratings yet
- NCP NephrolithiasisDocument3 pagesNCP NephrolithiasisMANUEL EMERSONNo ratings yet
- NCP LatestDocument6 pagesNCP LatestThirdy AquinoNo ratings yet
- Bacillus Clausii ErcefloraDocument1 pageBacillus Clausii ErcefloraCezhille BattadNo ratings yet
- Pathophysiology of Acute GastroenteritisDocument1 pagePathophysiology of Acute GastroenteritisAlliah Grejie AnneNo ratings yet
- NCP HyperthermiaDocument1 pageNCP HyperthermiaPastor James PacadaljenNo ratings yet
- Chronic Renal Failure Nursing Care PlanDocument6 pagesChronic Renal Failure Nursing Care PlanRuva Oscass JimmyNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Hepatitis A PDFDocument2 pagesNursingcrib Com NURSING CARE PLAN Hepatitis A PDFswapnilazarusNo ratings yet
- Patty NCP HyperthermiaDocument4 pagesPatty NCP HyperthermiaPatricia Jean FaeldoneaNo ratings yet
- Pa Tho Physiology of Acute GastroenteritisDocument2 pagesPa Tho Physiology of Acute Gastroenteritisromeo rivera100% (16)
- Case Study BkaDocument92 pagesCase Study BkaMaria CabangonNo ratings yet
- BNP (C)Document2 pagesBNP (C)Mae Ann Bueno CastillonNo ratings yet
- NCP of MGH PatientDocument2 pagesNCP of MGH PatientMaverick LimNo ratings yet
- Pa Tho Physiology of AchalasiaDocument1 pagePa Tho Physiology of AchalasiaSewyel GarburiNo ratings yet
- Drug Name Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesDocument4 pagesDrug Name Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibilitiesangel cenaNo ratings yet
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- Volume 1Document2 pagesVolume 1roxybiscanteNo ratings yet
- Ate Gabs Nyo Pagod NaDocument3 pagesAte Gabs Nyo Pagod NaGabrielle EvangelistaNo ratings yet
- Fluid Volume Deficit Related To Nausea and VomitDocument3 pagesFluid Volume Deficit Related To Nausea and VomitJakeNo ratings yet
- Deficient Fluid Volume (AGEDocument2 pagesDeficient Fluid Volume (AGENursesLabs.com83% (6)
- Subjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Document5 pagesSubjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Erle Gray CadangenNo ratings yet
- NCP Deficit Fluid VolumeDocument4 pagesNCP Deficit Fluid VolumeKingJayson Pacman06No ratings yet
- Fluid Volume Deficit Related To Loose Watery Stool Diarrhea)Document2 pagesFluid Volume Deficit Related To Loose Watery Stool Diarrhea)Jesse James Advincula Edjec100% (15)
- Assessment Explanation of The Problem Objective Intervention Rationale Evaluation Subjective: Objective: Sto: DX StoDocument2 pagesAssessment Explanation of The Problem Objective Intervention Rationale Evaluation Subjective: Objective: Sto: DX StoBasema HashhashNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Scientific Background Planning Implementation Rationale EvaluationDocument3 pagesNursing Care Plan: Assessment Nursing Diagnosis Scientific Background Planning Implementation Rationale EvaluationMelrhean GraceNo ratings yet
- Case #2 Nursing Care PlanDocument2 pagesCase #2 Nursing Care PlanPauline AñesNo ratings yet
- Risk NCP - PESCADERO 4CDocument1 pageRisk NCP - PESCADERO 4COrlando VillanuevaNo ratings yet
- NCP-Fluid Volume DeficitDocument2 pagesNCP-Fluid Volume Deficitanon_207994234100% (1)
- Assessment Nursing Diagnosis Planning Intervention Evaluation ObjectivesDocument4 pagesAssessment Nursing Diagnosis Planning Intervention Evaluation Objectivesashamy acolNo ratings yet
- 3rd Year Nursing RESEARCH MIDTERM QUIZESDocument3 pages3rd Year Nursing RESEARCH MIDTERM QUIZESAudrie Allyson GabalesNo ratings yet
- CS6 Alzheimer DiseaseDocument21 pagesCS6 Alzheimer DiseaseAudrie Allyson GabalesNo ratings yet
- 3rd Year Nursing MS LEC MIDTERM QUIZESDocument18 pages3rd Year Nursing MS LEC MIDTERM QUIZESAudrie Allyson GabalesNo ratings yet
- CS6 Alzheimer's Disease Drug StudyDocument3 pagesCS6 Alzheimer's Disease Drug StudyAudrie Allyson GabalesNo ratings yet
- Breast Self ExaminationDocument81 pagesBreast Self ExaminationAudrie Allyson Gabales100% (1)
- DISCHARGE PLAN & RRL For Colorectal CancerDocument2 pagesDISCHARGE PLAN & RRL For Colorectal CancerAudrie Allyson GabalesNo ratings yet
- Aag Drug StudyDocument7 pagesAag Drug StudyAudrie Allyson GabalesNo ratings yet
- Diagnostic Prodecures X Ray Utz CT Scan MriecgeegDocument42 pagesDiagnostic Prodecures X Ray Utz CT Scan MriecgeegAudrie Allyson GabalesNo ratings yet
- Drug Study HIVDocument10 pagesDrug Study HIVAudrie Allyson GabalesNo ratings yet
- Week 7 PARENTERAL NUTRITIONDocument51 pagesWeek 7 PARENTERAL NUTRITIONAudrie Allyson GabalesNo ratings yet
- Colorectal Cancer DRUG STUDYDocument12 pagesColorectal Cancer DRUG STUDYAudrie Allyson GabalesNo ratings yet
- CS4 Asthma Drug StudyDocument10 pagesCS4 Asthma Drug StudyAudrie Allyson GabalesNo ratings yet
- Colorectal Cancer NCPDocument6 pagesColorectal Cancer NCPAudrie Allyson GabalesNo ratings yet
- CS5 (AGE) Acute Gastroenteritis DRUG STUDYDocument8 pagesCS5 (AGE) Acute Gastroenteritis DRUG STUDYAudrie Allyson GabalesNo ratings yet
- Nursing Care Plan For PneumoniaDocument2 pagesNursing Care Plan For PneumoniaAudrie Allyson GabalesNo ratings yet
- Defining Characteristics Nursing Diagnosis Outcome Identification Nursing Interventions Rationale EvaluationDocument2 pagesDefining Characteristics Nursing Diagnosis Outcome Identification Nursing Interventions Rationale EvaluationAudrie Allyson GabalesNo ratings yet
- L. N .E.R.-'': and The Silver Jubilee'' TrainDocument3 pagesL. N .E.R.-'': and The Silver Jubilee'' TrainIan FlackNo ratings yet
- 07. ĐỀ THI VÀO LỚP 10-CẦN THƠ (2020-2021)Document8 pages07. ĐỀ THI VÀO LỚP 10-CẦN THƠ (2020-2021)Vương ThànhNo ratings yet
- Chemistry Project On Presence of Insecticides & Pesticides in FDocument8 pagesChemistry Project On Presence of Insecticides & Pesticides in FShaila BhandaryNo ratings yet
- Assam 04092012Document53 pagesAssam 04092012Sahu PraveenNo ratings yet
- Grade Thresholds - June 2023: Cambridge International AS & A Level Thinking Skills (9694)Document2 pagesGrade Thresholds - June 2023: Cambridge International AS & A Level Thinking Skills (9694)rqb7704No ratings yet
- Presentation Geotextile (November 2010)Document22 pagesPresentation Geotextile (November 2010)Gizachew ZelekeNo ratings yet
- Solution-Focused Nursing Rethinking Prac PDFDocument1 pageSolution-Focused Nursing Rethinking Prac PDFSHUMETNo ratings yet
- RESEARCH PROPOSAL Detriorating Standard of Education in PakistanDocument12 pagesRESEARCH PROPOSAL Detriorating Standard of Education in Pakistanjaydee_atc581454% (13)
- Chaff CutterDocument23 pagesChaff CutterFekadie TesfaNo ratings yet
- Introductions To Valuation Methods and Requirements 1672683839Document51 pagesIntroductions To Valuation Methods and Requirements 1672683839v7qksq5bzg100% (1)
- Business ProposalDocument35 pagesBusiness ProposalMJ MacapagalNo ratings yet
- Case Study - SkyworksDocument46 pagesCase Study - SkyworksMohd Fadzli JiFadNo ratings yet
- Advatage and DisadadvatagesDocument5 pagesAdvatage and DisadadvatagesPawan PathakNo ratings yet
- Guidelines and Fundamental Considerations For Axle BalancingDocument40 pagesGuidelines and Fundamental Considerations For Axle BalancingAnonymous PVXBGg9TNo ratings yet
- Mark Scheme: Q Scheme Marks Aos Pearson Progression Step and Progress Descriptor 1 M1Document9 pagesMark Scheme: Q Scheme Marks Aos Pearson Progression Step and Progress Descriptor 1 M1sara jaimeNo ratings yet
- Physics 2018 Prelims NYJC Paper 2Document19 pagesPhysics 2018 Prelims NYJC Paper 2NG KAI EE EMMANUELLE NG KAI EE EMMANUELLENo ratings yet
- Certiport Exam Administration Policies: Examination SecurityDocument2 pagesCertiport Exam Administration Policies: Examination SecurityrajputamitdNo ratings yet
- Light Rail TransitDocument4 pagesLight Rail TransitnalakasaNo ratings yet
- Software Quality Assurance: Lecture # 6Document37 pagesSoftware Quality Assurance: Lecture # 6rabiaNo ratings yet
- Thesis On Mughal ArchitectureDocument5 pagesThesis On Mughal Architecturecarlajardinebellevue100% (2)
- Loop Switching PDFDocument176 pagesLoop Switching PDFshawnr7376No ratings yet
- B NilfiskDocument16 pagesB Nilfiskarjun0188No ratings yet
- 5.00 FD An1 s1 CE Chemistry 23-24Document4 pages5.00 FD An1 s1 CE Chemistry 23-24imsNo ratings yet