
Bacterial Meningitis: Etiology and Pathophysiology
Bacterial Meningitis: Etiology and Pathophysiology
You might also like
- Ebook PDF Vanders Human Physiology The Mechanisms of Body Function 13th Edition PDFDocument40 pagesEbook PDF Vanders Human Physiology The Mechanisms of Body Function 13th Edition PDFmarie.simons15697% (35)
- Nurse Practitioner Board ReviewFrom EverandNurse Practitioner Board ReviewRating: 5 out of 5 stars5/5 (1)
- Handstand Push Up ProgressionDocument7 pagesHandstand Push Up ProgressionsandeepbhutaniNo ratings yet
- TB MeningitisDocument18 pagesTB Meningitisjesa34No ratings yet
- Fabrication of Pneumatic Punching and Riveting MachineDocument45 pagesFabrication of Pneumatic Punching and Riveting MachineElakkiya Karthic100% (7)
- Meningitis and Dementia: Dr. Lubna DwerijDocument52 pagesMeningitis and Dementia: Dr. Lubna DwerijNoor MajaliNo ratings yet
- MeningitisDocument46 pagesMeningitisKural ArasanNo ratings yet
- Definition-: Neisseria Meningitidis Invading The Subarachnoid Space of The BrainDocument12 pagesDefinition-: Neisseria Meningitidis Invading The Subarachnoid Space of The BrainAmit MartinNo ratings yet
- Meningitis &encephalitisDocument9 pagesMeningitis &encephalitisSnIP StandredNo ratings yet
- Bacterial Meningitis in ChildrenDocument10 pagesBacterial Meningitis in ChildrenAnny AryanyNo ratings yet
- Bacterial Meningitis Patho PaperDocument5 pagesBacterial Meningitis Patho PaperJessica BrayNo ratings yet
- Acute Bacterial MeningitisDocument15 pagesAcute Bacterial MeningitisOana StefanNo ratings yet
- Community Acuired Bactarial MeningitisDocument16 pagesCommunity Acuired Bactarial Meningitisidno1008No ratings yet
- Blank 10Document7 pagesBlank 10Leomer Calderon jr.No ratings yet
- EncephalitisDocument37 pagesEncephalitisPRADEEPNo ratings yet
- Central Nervous System InfectionDocument12 pagesCentral Nervous System InfectionJoseph DuffyNo ratings yet
- Neurological Infections: Gerard Gabriel P. Reotutar, RM, RN, MANDocument33 pagesNeurological Infections: Gerard Gabriel P. Reotutar, RM, RN, MANJeremiash Noblesala Dela CruzNo ratings yet
- Ssell Pediatrics 05.CNS InfectionDocument13 pagesSsell Pediatrics 05.CNS InfectionMujtaba JawadNo ratings yet
- Meningitis MedscapeDocument73 pagesMeningitis MedscapeBujangNo ratings yet
- Viral Inf of CNSDocument42 pagesViral Inf of CNSTarik100% (1)
- CNSinfectionsDocument79 pagesCNSinfectionsMatusala BafaNo ratings yet
- Meningitis PresentationDocument41 pagesMeningitis PresentationO'Mark AndrewsNo ratings yet
- Cns InfectionsDocument56 pagesCns InfectionsDinaNo ratings yet
- Intracranial Infection - Prof SunartiniDocument12 pagesIntracranial Infection - Prof SunartiniFranciscus BuwanaNo ratings yet
- Menigitis EncephalitisDocument63 pagesMenigitis EncephalitisHussain Azhar100% (1)
- Meningitis - Practice Essentials, Background, PathophysiologyDocument26 pagesMeningitis - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- Tuberculosis of The Central NsDocument74 pagesTuberculosis of The Central Nsderarataye6No ratings yet
- Pubid-848078832 1010 PDFDocument10 pagesPubid-848078832 1010 PDFCocosul Cocosului CocosaruluiNo ratings yet
- Infectious and Inflammatory Diseases of Brain and Spinal CordDocument50 pagesInfectious and Inflammatory Diseases of Brain and Spinal CordKeerthana BNo ratings yet
- Meningitis Clinical PresentationDocument10 pagesMeningitis Clinical PresentationAniwat NillakarnNo ratings yet
- Neurological InfectionsDocument21 pagesNeurological Infectionsfortuneholiness11No ratings yet
- Neurological Infections: By, Mr. Anish Ghosh M.Sc. Nursing 2 YearDocument57 pagesNeurological Infections: By, Mr. Anish Ghosh M.Sc. Nursing 2 YearAnish GhoshNo ratings yet
- CPPP PP P PP PPPPPPP PPDocument3 pagesCPPP PP P PP PPPPPPP PPangelieballesterosNo ratings yet
- Signs and Symptoms: Clinical PresentationDocument11 pagesSigns and Symptoms: Clinical PresentationGaluh NurfadillahNo ratings yet
- Pathology of The Central Nervous SystemDocument78 pagesPathology of The Central Nervous Systemعلي عليNo ratings yet
- College of Nursing Berhampur: Subject-Medical Surgical Nursing Topic-MeningitisDocument9 pagesCollege of Nursing Berhampur: Subject-Medical Surgical Nursing Topic-MeningitisAmlan jyoti thanapati100% (1)
- D17B PresentationDocument28 pagesD17B PresentationBruno KandatamNo ratings yet
- Meningitis: By-Dr Nimco A. MDDocument31 pagesMeningitis: By-Dr Nimco A. MDgibreilNo ratings yet
- Recurrent MeningitisDocument14 pagesRecurrent Meningitisidno1008No ratings yet
- CNS Infection DR DPDocument93 pagesCNS Infection DR DPFini AndrianiNo ratings yet
- Approach To The Patient With Suspected Infection of SNCDocument12 pagesApproach To The Patient With Suspected Infection of SNCJosé Miguel FerreiraNo ratings yet
- Meningitis (Lab Exam)Document1 pageMeningitis (Lab Exam)MohammadAwitNo ratings yet
- SNC TuberculosisDocument19 pagesSNC TuberculosisFabricio NuñezNo ratings yet
- AcuteDocument11 pagesAcutenunu ahmedNo ratings yet
- Chapter 22Document7 pagesChapter 22Lyra Ortega OliquinoNo ratings yet
- Cerebral Toxoplasmosis With Immunocompromised Tugas PKBDocument12 pagesCerebral Toxoplasmosis With Immunocompromised Tugas PKBApriliaNo ratings yet
- CNS Infections - MeningitisDocument156 pagesCNS Infections - MeningitisauNo ratings yet
- Signs and SymptomsDocument33 pagesSigns and SymptomsGaluh NurfadillahNo ratings yet
- Module 7 - Meningitis and EncephalitisDocument35 pagesModule 7 - Meningitis and EncephalitisRick RanitNo ratings yet
- Neurologic Disorders Part 4Document99 pagesNeurologic Disorders Part 4Aly RiveraNo ratings yet
- Viral MeningitisDocument19 pagesViral MeningitisUneebNo ratings yet
- 33 MeningitisDocument71 pages33 MeningitisKaif KhanNo ratings yet
- Epidemic Cerebrospinal MeningitisDocument49 pagesEpidemic Cerebrospinal MeningitisDrAbhilash RMNo ratings yet
- Meningitis: Classification and External ResourcesDocument8 pagesMeningitis: Classification and External ResourcesChoco MuchoNo ratings yet
- 2 Brain AbscessDocument25 pages2 Brain AbscessKaif KhanNo ratings yet
- Meningitis and Encephalitis: Samantha Noll June 11, 2015Document45 pagesMeningitis and Encephalitis: Samantha Noll June 11, 2015galihNo ratings yet
- Research Paper On Bacterial MeningitisDocument8 pagesResearch Paper On Bacterial Meningitisvvgnzdbkf100% (1)
- Nyarang'o Dennis Level IIIDocument29 pagesNyarang'o Dennis Level IIIBryan AmataNo ratings yet
- Subacute and Chronic MeningitisDocument8 pagesSubacute and Chronic MeningitisLucky PuspitasariNo ratings yet
- Investigatory Project On MeningitisDocument15 pagesInvestigatory Project On MeningitisMaanya PrithianiNo ratings yet
- Cysticercosis - Clinical Manifestations and Diagnosis - UpToDateDocument26 pagesCysticercosis - Clinical Manifestations and Diagnosis - UpToDateAndréia GomesNo ratings yet
- ENLS Meningitis and Encephalitis ProtocolDocument20 pagesENLS Meningitis and Encephalitis ProtocolFransiskus MikaelNo ratings yet
- Technology and Operations ManagementDocument26 pagesTechnology and Operations ManagementAnna Dolot100% (1)
- ARA 111 (PREPARATORY ARABIC) - First Sem 2021Document15 pagesARA 111 (PREPARATORY ARABIC) - First Sem 2021Mohaimen GuroNo ratings yet
- IT0007-Laboratory-Exercise-7 - Incident HandlingDocument5 pagesIT0007-Laboratory-Exercise-7 - Incident HandlingDenise JaoNo ratings yet
- Kuno PaperDocument5 pagesKuno Paperkshipra soniNo ratings yet
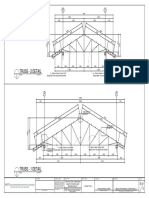
- Truss - 2 Detail: Scale 1: 50 MTRSDocument1 pageTruss - 2 Detail: Scale 1: 50 MTRSGerald MasangayNo ratings yet
- Sony XR Ca370Document32 pagesSony XR Ca370eugen26mNo ratings yet
- 5-Whys Guide& Template: Step-By-Step InstructionsDocument5 pages5-Whys Guide& Template: Step-By-Step InstructionsSudhakar Lakshmana RajNo ratings yet
- (Download PDF) Pastoral Theology and Care Critical Trajectories in Theory and Practice First Edition Ramsay Online Ebook All Chapter PDFDocument42 pages(Download PDF) Pastoral Theology and Care Critical Trajectories in Theory and Practice First Edition Ramsay Online Ebook All Chapter PDFsarah.bronk892100% (11)
- Elena Rodriguez Reflective EssayDocument1 pageElena Rodriguez Reflective EssayElena Rodriguez ZuletaNo ratings yet
- Solution Manual For Computer and Communication Networks 2 e Nader F MirDocument35 pagesSolution Manual For Computer and Communication Networks 2 e Nader F Mirconcreteprimula2ppwr100% (16)
- Melon Growing Tips PDFDocument1 pageMelon Growing Tips PDFTaahirah Ben ZinatNo ratings yet
- Pulse in The Stomach - Could It Be An Abdominal Aortic AneurysmDocument3 pagesPulse in The Stomach - Could It Be An Abdominal Aortic AneurysmLazar VučetićNo ratings yet
- ELEKTROLISISDocument3 pagesELEKTROLISISrazhafiraahNo ratings yet
- Collection Receipt Cum Adjustment Voucher: The New India Assurance Co. Ltd. (Government of India Undertaking)Document2 pagesCollection Receipt Cum Adjustment Voucher: The New India Assurance Co. Ltd. (Government of India Undertaking)fio communicationNo ratings yet
- 2021 Specimen Paper 4 PDFDocument6 pages2021 Specimen Paper 4 PDFZain CruiseNo ratings yet
- Smiths of Winterforge Rulebook 0.9Document9 pagesSmiths of Winterforge Rulebook 0.9NatsukiPLNo ratings yet
- Ch06 Solations Brigham 10th EDocument32 pagesCh06 Solations Brigham 10th ERafay HussainNo ratings yet
- April 5, 2018 Engr Alex Relampagos Subject: Supply, Delivery, Installation of Fire Detection and Alarm SystemDocument2 pagesApril 5, 2018 Engr Alex Relampagos Subject: Supply, Delivery, Installation of Fire Detection and Alarm SystemAlexander Luega Relampagos0% (1)
- Interim E-Notarial Rules (As of July 5 2020)Document20 pagesInterim E-Notarial Rules (As of July 5 2020)Ken LimNo ratings yet
- Gutindex 2009Document170 pagesGutindex 2009Lankesh ZadeNo ratings yet
- Statement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDocument6 pagesStatement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceMahi ThakurNo ratings yet
- Safe ManualDocument2 pagesSafe Manualsrujan patelNo ratings yet
- Jerusalem Studies in Religion andDocument477 pagesJerusalem Studies in Religion andJason PangNo ratings yet
- FIN515 Hw4JDVDocument7 pagesFIN515 Hw4JDVvalderramadavid100% (1)
- Usr Local SRC Education - Com Files Static Lesson-Plans Mapping-My-World Mapping-My-WorldDocument6 pagesUsr Local SRC Education - Com Files Static Lesson-Plans Mapping-My-World Mapping-My-Worldyerikalasupriya90No ratings yet
- SCM Final ReportDocument12 pagesSCM Final ReportSYED DANIYAL HASSAN SHAHNo ratings yet
- Flashcards - Topic 6.1 6.4 - Microbiology - Edexcel IAL Biology A LevelDocument49 pagesFlashcards - Topic 6.1 6.4 - Microbiology - Edexcel IAL Biology A LevelULFANo ratings yet






















































































Download as pdf or txt
You might also like
- Ebook PDF Vanders Human Physiology The Mechanisms of Body Function 13th Edition PDFDocument40 pagesEbook PDF Vanders Human Physiology The Mechanisms of Body Function 13th Edition PDFmarie.simons15697% (35)
- Nurse Practitioner Board ReviewFrom EverandNurse Practitioner Board ReviewRating: 5 out of 5 stars5/5 (1)
- Handstand Push Up ProgressionDocument7 pagesHandstand Push Up ProgressionsandeepbhutaniNo ratings yet
- TB MeningitisDocument18 pagesTB Meningitisjesa34No ratings yet
- Fabrication of Pneumatic Punching and Riveting MachineDocument45 pagesFabrication of Pneumatic Punching and Riveting MachineElakkiya Karthic100% (7)
- Meningitis and Dementia: Dr. Lubna DwerijDocument52 pagesMeningitis and Dementia: Dr. Lubna DwerijNoor MajaliNo ratings yet
- MeningitisDocument46 pagesMeningitisKural ArasanNo ratings yet
- Definition-: Neisseria Meningitidis Invading The Subarachnoid Space of The BrainDocument12 pagesDefinition-: Neisseria Meningitidis Invading The Subarachnoid Space of The BrainAmit MartinNo ratings yet
- Meningitis &encephalitisDocument9 pagesMeningitis &encephalitisSnIP StandredNo ratings yet
- Bacterial Meningitis in ChildrenDocument10 pagesBacterial Meningitis in ChildrenAnny AryanyNo ratings yet
- Bacterial Meningitis Patho PaperDocument5 pagesBacterial Meningitis Patho PaperJessica BrayNo ratings yet
- Acute Bacterial MeningitisDocument15 pagesAcute Bacterial MeningitisOana StefanNo ratings yet
- Community Acuired Bactarial MeningitisDocument16 pagesCommunity Acuired Bactarial Meningitisidno1008No ratings yet
- Blank 10Document7 pagesBlank 10Leomer Calderon jr.No ratings yet
- EncephalitisDocument37 pagesEncephalitisPRADEEPNo ratings yet
- Central Nervous System InfectionDocument12 pagesCentral Nervous System InfectionJoseph DuffyNo ratings yet
- Neurological Infections: Gerard Gabriel P. Reotutar, RM, RN, MANDocument33 pagesNeurological Infections: Gerard Gabriel P. Reotutar, RM, RN, MANJeremiash Noblesala Dela CruzNo ratings yet
- Ssell Pediatrics 05.CNS InfectionDocument13 pagesSsell Pediatrics 05.CNS InfectionMujtaba JawadNo ratings yet
- Meningitis MedscapeDocument73 pagesMeningitis MedscapeBujangNo ratings yet
- Viral Inf of CNSDocument42 pagesViral Inf of CNSTarik100% (1)
- CNSinfectionsDocument79 pagesCNSinfectionsMatusala BafaNo ratings yet
- Meningitis PresentationDocument41 pagesMeningitis PresentationO'Mark AndrewsNo ratings yet
- Cns InfectionsDocument56 pagesCns InfectionsDinaNo ratings yet
- Intracranial Infection - Prof SunartiniDocument12 pagesIntracranial Infection - Prof SunartiniFranciscus BuwanaNo ratings yet
- Menigitis EncephalitisDocument63 pagesMenigitis EncephalitisHussain Azhar100% (1)
- Meningitis - Practice Essentials, Background, PathophysiologyDocument26 pagesMeningitis - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- Tuberculosis of The Central NsDocument74 pagesTuberculosis of The Central Nsderarataye6No ratings yet
- Pubid-848078832 1010 PDFDocument10 pagesPubid-848078832 1010 PDFCocosul Cocosului CocosaruluiNo ratings yet
- Infectious and Inflammatory Diseases of Brain and Spinal CordDocument50 pagesInfectious and Inflammatory Diseases of Brain and Spinal CordKeerthana BNo ratings yet
- Meningitis Clinical PresentationDocument10 pagesMeningitis Clinical PresentationAniwat NillakarnNo ratings yet
- Neurological InfectionsDocument21 pagesNeurological Infectionsfortuneholiness11No ratings yet
- Neurological Infections: By, Mr. Anish Ghosh M.Sc. Nursing 2 YearDocument57 pagesNeurological Infections: By, Mr. Anish Ghosh M.Sc. Nursing 2 YearAnish GhoshNo ratings yet
- CPPP PP P PP PPPPPPP PPDocument3 pagesCPPP PP P PP PPPPPPP PPangelieballesterosNo ratings yet
- Signs and Symptoms: Clinical PresentationDocument11 pagesSigns and Symptoms: Clinical PresentationGaluh NurfadillahNo ratings yet
- Pathology of The Central Nervous SystemDocument78 pagesPathology of The Central Nervous Systemعلي عليNo ratings yet
- College of Nursing Berhampur: Subject-Medical Surgical Nursing Topic-MeningitisDocument9 pagesCollege of Nursing Berhampur: Subject-Medical Surgical Nursing Topic-MeningitisAmlan jyoti thanapati100% (1)
- D17B PresentationDocument28 pagesD17B PresentationBruno KandatamNo ratings yet
- Meningitis: By-Dr Nimco A. MDDocument31 pagesMeningitis: By-Dr Nimco A. MDgibreilNo ratings yet
- Recurrent MeningitisDocument14 pagesRecurrent Meningitisidno1008No ratings yet
- CNS Infection DR DPDocument93 pagesCNS Infection DR DPFini AndrianiNo ratings yet
- Approach To The Patient With Suspected Infection of SNCDocument12 pagesApproach To The Patient With Suspected Infection of SNCJosé Miguel FerreiraNo ratings yet
- Meningitis (Lab Exam)Document1 pageMeningitis (Lab Exam)MohammadAwitNo ratings yet
- SNC TuberculosisDocument19 pagesSNC TuberculosisFabricio NuñezNo ratings yet
- AcuteDocument11 pagesAcutenunu ahmedNo ratings yet
- Chapter 22Document7 pagesChapter 22Lyra Ortega OliquinoNo ratings yet
- Cerebral Toxoplasmosis With Immunocompromised Tugas PKBDocument12 pagesCerebral Toxoplasmosis With Immunocompromised Tugas PKBApriliaNo ratings yet
- CNS Infections - MeningitisDocument156 pagesCNS Infections - MeningitisauNo ratings yet
- Signs and SymptomsDocument33 pagesSigns and SymptomsGaluh NurfadillahNo ratings yet
- Module 7 - Meningitis and EncephalitisDocument35 pagesModule 7 - Meningitis and EncephalitisRick RanitNo ratings yet
- Neurologic Disorders Part 4Document99 pagesNeurologic Disorders Part 4Aly RiveraNo ratings yet
- Viral MeningitisDocument19 pagesViral MeningitisUneebNo ratings yet
- 33 MeningitisDocument71 pages33 MeningitisKaif KhanNo ratings yet
- Epidemic Cerebrospinal MeningitisDocument49 pagesEpidemic Cerebrospinal MeningitisDrAbhilash RMNo ratings yet
- Meningitis: Classification and External ResourcesDocument8 pagesMeningitis: Classification and External ResourcesChoco MuchoNo ratings yet
- 2 Brain AbscessDocument25 pages2 Brain AbscessKaif KhanNo ratings yet
- Meningitis and Encephalitis: Samantha Noll June 11, 2015Document45 pagesMeningitis and Encephalitis: Samantha Noll June 11, 2015galihNo ratings yet
- Research Paper On Bacterial MeningitisDocument8 pagesResearch Paper On Bacterial Meningitisvvgnzdbkf100% (1)
- Nyarang'o Dennis Level IIIDocument29 pagesNyarang'o Dennis Level IIIBryan AmataNo ratings yet
- Subacute and Chronic MeningitisDocument8 pagesSubacute and Chronic MeningitisLucky PuspitasariNo ratings yet
- Investigatory Project On MeningitisDocument15 pagesInvestigatory Project On MeningitisMaanya PrithianiNo ratings yet
- Cysticercosis - Clinical Manifestations and Diagnosis - UpToDateDocument26 pagesCysticercosis - Clinical Manifestations and Diagnosis - UpToDateAndréia GomesNo ratings yet
- ENLS Meningitis and Encephalitis ProtocolDocument20 pagesENLS Meningitis and Encephalitis ProtocolFransiskus MikaelNo ratings yet
- Technology and Operations ManagementDocument26 pagesTechnology and Operations ManagementAnna Dolot100% (1)
- ARA 111 (PREPARATORY ARABIC) - First Sem 2021Document15 pagesARA 111 (PREPARATORY ARABIC) - First Sem 2021Mohaimen GuroNo ratings yet
- IT0007-Laboratory-Exercise-7 - Incident HandlingDocument5 pagesIT0007-Laboratory-Exercise-7 - Incident HandlingDenise JaoNo ratings yet
- Kuno PaperDocument5 pagesKuno Paperkshipra soniNo ratings yet
- Truss - 2 Detail: Scale 1: 50 MTRSDocument1 pageTruss - 2 Detail: Scale 1: 50 MTRSGerald MasangayNo ratings yet
- Sony XR Ca370Document32 pagesSony XR Ca370eugen26mNo ratings yet
- 5-Whys Guide& Template: Step-By-Step InstructionsDocument5 pages5-Whys Guide& Template: Step-By-Step InstructionsSudhakar Lakshmana RajNo ratings yet
- (Download PDF) Pastoral Theology and Care Critical Trajectories in Theory and Practice First Edition Ramsay Online Ebook All Chapter PDFDocument42 pages(Download PDF) Pastoral Theology and Care Critical Trajectories in Theory and Practice First Edition Ramsay Online Ebook All Chapter PDFsarah.bronk892100% (11)
- Elena Rodriguez Reflective EssayDocument1 pageElena Rodriguez Reflective EssayElena Rodriguez ZuletaNo ratings yet
- Solution Manual For Computer and Communication Networks 2 e Nader F MirDocument35 pagesSolution Manual For Computer and Communication Networks 2 e Nader F Mirconcreteprimula2ppwr100% (16)
- Melon Growing Tips PDFDocument1 pageMelon Growing Tips PDFTaahirah Ben ZinatNo ratings yet
- Pulse in The Stomach - Could It Be An Abdominal Aortic AneurysmDocument3 pagesPulse in The Stomach - Could It Be An Abdominal Aortic AneurysmLazar VučetićNo ratings yet
- ELEKTROLISISDocument3 pagesELEKTROLISISrazhafiraahNo ratings yet
- Collection Receipt Cum Adjustment Voucher: The New India Assurance Co. Ltd. (Government of India Undertaking)Document2 pagesCollection Receipt Cum Adjustment Voucher: The New India Assurance Co. Ltd. (Government of India Undertaking)fio communicationNo ratings yet
- 2021 Specimen Paper 4 PDFDocument6 pages2021 Specimen Paper 4 PDFZain CruiseNo ratings yet
- Smiths of Winterforge Rulebook 0.9Document9 pagesSmiths of Winterforge Rulebook 0.9NatsukiPLNo ratings yet
- Ch06 Solations Brigham 10th EDocument32 pagesCh06 Solations Brigham 10th ERafay HussainNo ratings yet
- April 5, 2018 Engr Alex Relampagos Subject: Supply, Delivery, Installation of Fire Detection and Alarm SystemDocument2 pagesApril 5, 2018 Engr Alex Relampagos Subject: Supply, Delivery, Installation of Fire Detection and Alarm SystemAlexander Luega Relampagos0% (1)
- Interim E-Notarial Rules (As of July 5 2020)Document20 pagesInterim E-Notarial Rules (As of July 5 2020)Ken LimNo ratings yet
- Gutindex 2009Document170 pagesGutindex 2009Lankesh ZadeNo ratings yet
- Statement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDocument6 pagesStatement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceMahi ThakurNo ratings yet
- Safe ManualDocument2 pagesSafe Manualsrujan patelNo ratings yet
- Jerusalem Studies in Religion andDocument477 pagesJerusalem Studies in Religion andJason PangNo ratings yet
- FIN515 Hw4JDVDocument7 pagesFIN515 Hw4JDVvalderramadavid100% (1)
- Usr Local SRC Education - Com Files Static Lesson-Plans Mapping-My-World Mapping-My-WorldDocument6 pagesUsr Local SRC Education - Com Files Static Lesson-Plans Mapping-My-World Mapping-My-Worldyerikalasupriya90No ratings yet
- SCM Final ReportDocument12 pagesSCM Final ReportSYED DANIYAL HASSAN SHAHNo ratings yet
- Flashcards - Topic 6.1 6.4 - Microbiology - Edexcel IAL Biology A LevelDocument49 pagesFlashcards - Topic 6.1 6.4 - Microbiology - Edexcel IAL Biology A LevelULFANo ratings yet