Download as pdf or txt
You might also like
- Evolution A Developmental Approach Wallace Arthur PDFDocument2 pagesEvolution A Developmental Approach Wallace Arthur PDFLisaNo ratings yet
- Hybrid Mortality Prediction Using Multiple Source SystemsDocument8 pagesHybrid Mortality Prediction Using Multiple Source SystemsijcisjournalNo ratings yet
- Icuarm-A Valuable Approach in Clinical Decision Support SystemDocument5 pagesIcuarm-A Valuable Approach in Clinical Decision Support SystemInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Association Rules To Analyze Hospital Resources With Mortality RatesDocument7 pagesAssociation Rules To Analyze Hospital Resources With Mortality RatesIJRASETPublicationsNo ratings yet
- Prediction of ICU Admission For Covid-19 Patients A Machine Learning Approach Based On Complete Blood Count DataDocument6 pagesPrediction of ICU Admission For Covid-19 Patients A Machine Learning Approach Based On Complete Blood Count DataIJRASETPublicationsNo ratings yet
- Combining Structured and Unstructured Data Forpredictive Models A Deep Learning ApproachDocument10 pagesCombining Structured and Unstructured Data Forpredictive Models A Deep Learning ApproachSarmad N. MOHAMMEDNo ratings yet
- Prediction in Mimic 3 DataDocument8 pagesPrediction in Mimic 3 DataUday GulghaneNo ratings yet
- Survival Study On Medical Disease Diagnosis With Coronavirus DatabaseDocument9 pagesSurvival Study On Medical Disease Diagnosis With Coronavirus DatabaseIJRASETPublicationsNo ratings yet
- AI in MedicineDocument4 pagesAI in MedicinemjNo ratings yet
- Prognosis of Determined Cardiovascular Illnesses Using Machine Learning TechniquesDocument9 pagesPrognosis of Determined Cardiovascular Illnesses Using Machine Learning TechniquesIJRASETPublicationsNo ratings yet
- 2019 DsadaşsklDocument8 pages2019 DsadaşsklAhmet KaragozNo ratings yet
- Use of Machine Learning To Analyse Routinely Collected Intensive Care Unit Data: A Systematic ReviewDocument11 pagesUse of Machine Learning To Analyse Routinely Collected Intensive Care Unit Data: A Systematic ReviewDaniel MalpartidaNo ratings yet
- Combining Structured and Unstructured Data For Predictive Models: A Deep Learning ApproachDocument11 pagesCombining Structured and Unstructured Data For Predictive Models: A Deep Learning ApproachAbdelkader MEJDOUBNo ratings yet
- Base Paper 1Document5 pagesBase Paper 1SACHIN SAHUNo ratings yet
- Disease Prediction by Machine Learning Over Big Data From Healthcare CommunitiesDocument3 pagesDisease Prediction by Machine Learning Over Big Data From Healthcare CommunitiesAruna RajNo ratings yet
- Leveraging Clinical Time-Series Data For Prediction: A Cautionary TaleDocument10 pagesLeveraging Clinical Time-Series Data For Prediction: A Cautionary TaleEmotyNo ratings yet
- Article BI Knowledge Grid Support For Treatment of Traumatic Brain Injury VictimsDocument10 pagesArticle BI Knowledge Grid Support For Treatment of Traumatic Brain Injury VictimsjlkazadiNo ratings yet
- Heart Attack Predictions Using Machine LearningDocument8 pagesHeart Attack Predictions Using Machine LearningIJRASETPublicationsNo ratings yet
- Early Hospital Mortality Prediction Using Vital SignalsDocument11 pagesEarly Hospital Mortality Prediction Using Vital SignalsUday GulghaneNo ratings yet
- Predicting Unplanned Hospital Readmissions Using Patient Level DataDocument9 pagesPredicting Unplanned Hospital Readmissions Using Patient Level DataMeetGandhiNo ratings yet
- Covid19 Prediction Model With Hybrid Approach A ReviewDocument6 pagesCovid19 Prediction Model With Hybrid Approach A ReviewIJRASETPublicationsNo ratings yet
- Predicting Cardiovascular Disease Using Logistic Regression Research PaperDocument4 pagesPredicting Cardiovascular Disease Using Logistic Regression Research PaperSbobhuNo ratings yet
- Health CNN-SMO: To Secure and Enhance The Medical Healthcare System by Using Convolution Neural NetworkDocument4 pagesHealth CNN-SMO: To Secure and Enhance The Medical Healthcare System by Using Convolution Neural NetworkInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Prediction of ICU Admission Analysis For Covid-19 PatientsDocument6 pagesPrediction of ICU Admission Analysis For Covid-19 PatientsIJRASETPublicationsNo ratings yet
- Critical Care ApplicationsDocument3 pagesCritical Care ApplicationsJustine Bianca NayreNo ratings yet
- Heart Disease Prediction Using Logistic Regression AlgorithmDocument8 pagesHeart Disease Prediction Using Logistic Regression AlgorithmIJRASETPublicationsNo ratings yet
- Nursing Informatics - EditedDocument4 pagesNursing Informatics - Editeddaviace72No ratings yet
- Prediction of Cardiovascular Disease Using Machine Learning TechniquesDocument6 pagesPrediction of Cardiovascular Disease Using Machine Learning TechniquesNowreen HaqueNo ratings yet
- Biology: Synsiggan: Generative Adversarial Networks For Synthetic Biomedical Signal GenerationDocument20 pagesBiology: Synsiggan: Generative Adversarial Networks For Synthetic Biomedical Signal GenerationSahil FarhanNo ratings yet
- Information Systems: Secure Sharing of Healthcare Data Collaborative and in Multi-CloudsDocument8 pagesInformation Systems: Secure Sharing of Healthcare Data Collaborative and in Multi-CloudsxribeneNo ratings yet
- A Hadoop-Based Platform For Patient ClassificationDocument20 pagesA Hadoop-Based Platform For Patient Classificationprabhu rachutiNo ratings yet
- Check ThisDocument10 pagesCheck ThisC RAHUL RAO.571No ratings yet
- Poh 2014Document6 pagesPoh 2014karanNo ratings yet
- Artificial Intelligence and Big Data Science in NeDocument8 pagesArtificial Intelligence and Big Data Science in NeAxel Harim GuzmanNo ratings yet
- Analysis of Hybrid Machine Learning Algorithm For Heart Disease PredictionDocument7 pagesAnalysis of Hybrid Machine Learning Algorithm For Heart Disease PredictionIJRASETPublicationsNo ratings yet
- Prediction of Heart Diseases Using Machine LearningDocument49 pagesPrediction of Heart Diseases Using Machine Learningandyy4663No ratings yet
- (2023) ALF - Ambient Assisted Living For Healthcare Framework Based On IoMT and Big DataDocument9 pages(2023) ALF - Ambient Assisted Living For Healthcare Framework Based On IoMT and Big DataSUJITHA MEDURINo ratings yet
- A Long Short-Term Memory Ensemble Approach For Improving The Output Prediction in ICUDocument11 pagesA Long Short-Term Memory Ensemble Approach For Improving The Output Prediction in ICUIdris RabiuNo ratings yet
- My Data Figure Report TempDocument13 pagesMy Data Figure Report Tempapi-667814020No ratings yet
- Multitask Learning and Benchmarking With Clinical Time Series DataDocument18 pagesMultitask Learning and Benchmarking With Clinical Time Series DataJiancheng ZhangNo ratings yet
- Integrated Multimodal Arti Ficial Intelligence Framework For Healthcare ApplicationsDocument10 pagesIntegrated Multimodal Arti Ficial Intelligence Framework For Healthcare ApplicationsRaghavendranNo ratings yet
- A Multi-View Learning Based Clustering Method For Health Care SystemDocument9 pagesA Multi-View Learning Based Clustering Method For Health Care SystemIJRASETPublicationsNo ratings yet
- Prediction of Stroke Using Deep Learning Model: October 2017Document10 pagesPrediction of Stroke Using Deep Learning Model: October 2017darNo ratings yet
- Customization and External Validation of The Simplified Mortality Score For The Intensive Care Unit (SMS-ICU) in Brazilian Critically Ill PatientsDocument7 pagesCustomization and External Validation of The Simplified Mortality Score For The Intensive Care Unit (SMS-ICU) in Brazilian Critically Ill PatientsIsais NNo ratings yet
- Articulo Revista Artificial Intelligence in MedicineDocument8 pagesArticulo Revista Artificial Intelligence in MedicineAngelly TolozaNo ratings yet
- Multiple Disease Prediction SystemDocument9 pagesMultiple Disease Prediction SystemIJRASETPublications100% (1)
- Heart Disease Prediction Using Machine LearningDocument7 pagesHeart Disease Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Heart Disease Prediction-02-1Document27 pagesHeart Disease Prediction-02-1Aakash .RNo ratings yet
- Physionet Challenge 2019 CCM Manuscript PDFDocument26 pagesPhysionet Challenge 2019 CCM Manuscript PDFAmish SharmaNo ratings yet
- Prediction of Chronic Diseases From X-Rays Using Distributed Machine LearningDocument10 pagesPrediction of Chronic Diseases From X-Rays Using Distributed Machine LearningIJRASETPublicationsNo ratings yet
- Hyperparameter Optimization For Disease Detection and AnalysisDocument5 pagesHyperparameter Optimization For Disease Detection and AnalysisIJRASETPublicationsNo ratings yet
- Information: Ensemble Deep Learning Models For Heart Disease Classification: A Case Study From MexicoDocument28 pagesInformation: Ensemble Deep Learning Models For Heart Disease Classification: A Case Study From MexicosdfasfdNo ratings yet
- RM AatDocument5 pagesRM AatSukruthi KcNo ratings yet
- Heart Disease Prediction Using CNN, Deep Learning ModelDocument9 pagesHeart Disease Prediction Using CNN, Deep Learning ModelIJRASETPublicationsNo ratings yet
- Literature Review On Patient Monitoring SystemDocument6 pagesLiterature Review On Patient Monitoring Systemc5rc7ppr100% (1)
- Arti Ficial Intelligence in MedicineDocument8 pagesArti Ficial Intelligence in MedicineSAMUEL ESCARESNo ratings yet
- Using Artificial Intelligence To Detect Heart Disease Analysis of Grid Search To Increase Accuracy and Deploying Custom Models OnlineDocument4 pagesUsing Artificial Intelligence To Detect Heart Disease Analysis of Grid Search To Increase Accuracy and Deploying Custom Models OnlineInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Conference Paper FinalDocument14 pagesConference Paper FinalAdit SantokheeNo ratings yet
- 2021 Article 120Document14 pages2021 Article 120Fitri ainun MalahayatiNo ratings yet
- Prediction of Diabetes Using Machine Learning Algorithms in HealthcareDocument6 pagesPrediction of Diabetes Using Machine Learning Algorithms in HealthcareTamimjdNo ratings yet
- Neurocritical Care Informatics: Translating Raw Data into Bedside ActionFrom EverandNeurocritical Care Informatics: Translating Raw Data into Bedside ActionMichael De GeorgiaNo ratings yet
- Unit 3 OLAP and OLTPDocument64 pagesUnit 3 OLAP and OLTPvikasbhowateNo ratings yet
- Draft - Institute's Directions For Department Objectives - 2023-24-1Document4 pagesDraft - Institute's Directions For Department Objectives - 2023-24-1vikasbhowateNo ratings yet
- INFOTSAV 2k22Document28 pagesINFOTSAV 2k22vikasbhowateNo ratings yet
- Unit 1 - DWMDocument112 pagesUnit 1 - DWMvikasbhowateNo ratings yet
- Unit 2 - Data PreprocessingDocument42 pagesUnit 2 - Data PreprocessingvikasbhowateNo ratings yet
- MALPRACTICESDocument4 pagesMALPRACTICESvikasbhowateNo ratings yet
- Sensors: A Novel Secure Iot-Based Smart Home Automation System Using A Wireless Sensor NetworkDocument19 pagesSensors: A Novel Secure Iot-Based Smart Home Automation System Using A Wireless Sensor NetworkvikasbhowateNo ratings yet
- Image Similarity Aptitude Test 24TH Nov'22Document13 pagesImage Similarity Aptitude Test 24TH Nov'22vikasbhowateNo ratings yet
- InheritanceDocument2 pagesInheritancevikasbhowateNo ratings yet
- Neurocomputing: José-Ramón Cano, Pedro Antonio Gutiérrez, Bartosz Krawczyk, Michał Wo Zniak, Salvador GarcíaDocument15 pagesNeurocomputing: José-Ramón Cano, Pedro Antonio Gutiérrez, Bartosz Krawczyk, Michał Wo Zniak, Salvador GarcíavikasbhowateNo ratings yet
- Ensemble Models For Effective Classification of Big Data With Data ImbalanceDocument17 pagesEnsemble Models For Effective Classification of Big Data With Data ImbalancevikasbhowateNo ratings yet
- Bagging Using Instance-Level Difficulty For Multi-Class Imbalanced Big Data Classification On SparkDocument10 pagesBagging Using Instance-Level Difficulty For Multi-Class Imbalanced Big Data Classification On SparkvikasbhowateNo ratings yet
- Performance of Machine Learning Algorithms For Class-Imbalanced Process Fault Detection ProblemsDocument9 pagesPerformance of Machine Learning Algorithms For Class-Imbalanced Process Fault Detection ProblemsvikasbhowateNo ratings yet
- HAIL: A High-Availability and Integrity Layer For Cloud StorageDocument12 pagesHAIL: A High-Availability and Integrity Layer For Cloud StoragevikasbhowateNo ratings yet
- NewbookDocument80 pagesNewbookvikasbhowateNo ratings yet
- Knowledge-Based Systems: Michał Koziarski Michał Woźniak Bartosz KrawczykDocument16 pagesKnowledge-Based Systems: Michał Koziarski Michał Woźniak Bartosz KrawczykvikasbhowateNo ratings yet
- A Survey of Predictive Modeling On Imbalanced Domains: Computing MethodologiesDocument50 pagesA Survey of Predictive Modeling On Imbalanced Domains: Computing MethodologiesvikasbhowateNo ratings yet
- A Novel Riboswitch Classification Based On Imbalanced Sequences Achieved by Machine LearningDocument23 pagesA Novel Riboswitch Classification Based On Imbalanced Sequences Achieved by Machine LearningvikasbhowateNo ratings yet
- Enhanced Over - Sampling Techniques For Imbalanced Big Data Set Classi FicationDocument33 pagesEnhanced Over - Sampling Techniques For Imbalanced Big Data Set Classi FicationvikasbhowateNo ratings yet
- Lesson OutlineDocument30 pagesLesson OutlinevikasbhowateNo ratings yet
- Eng2 12298 PDFDocument24 pagesEng2 12298 PDFvikasbhowateNo ratings yet
- Over-Sampling Algorithm For Imbalanced Data Classification: XU Xiaolong, Chen Wen, and SUN YanfeiDocument10 pagesOver-Sampling Algorithm For Imbalanced Data Classification: XU Xiaolong, Chen Wen, and SUN YanfeivikasbhowateNo ratings yet
- SMOTEFUNA: Synthetic Minority Over-Sampling Technique Based On Furthest Neighbour AlgorithmDocument14 pagesSMOTEFUNA: Synthetic Minority Over-Sampling Technique Based On Furthest Neighbour AlgorithmvikasbhowateNo ratings yet
- Design and Implementation of Secure File Storage Using Distributed Cloud MechanismDocument5 pagesDesign and Implementation of Secure File Storage Using Distributed Cloud MechanismvikasbhowateNo ratings yet
- Multi-Cloud Secure Data Storage Using Cryptographic TechniquesDocument4 pagesMulti-Cloud Secure Data Storage Using Cryptographic TechniquesvikasbhowateNo ratings yet
- Secure Cloud Data Storage: From Single To Multi-Cloud EnvironmentDocument4 pagesSecure Cloud Data Storage: From Single To Multi-Cloud EnvironmentvikasbhowateNo ratings yet
- A Framework For Establishing Trust in Cloud Provenance: Imad M. AbbadiDocument18 pagesA Framework For Establishing Trust in Cloud Provenance: Imad M. AbbadivikasbhowateNo ratings yet
- A Cost Efficient Multi-Cloud Data Hosting Scheme Using CharmDocument6 pagesA Cost Efficient Multi-Cloud Data Hosting Scheme Using CharmvikasbhowateNo ratings yet
- Class 5 Syllabus Plan 2024-2025 Structured Test 1Document2 pagesClass 5 Syllabus Plan 2024-2025 Structured Test 1shetty.vgNo ratings yet
- LGBTQ-themed Young Adult LiteratureDocument9 pagesLGBTQ-themed Young Adult LiteratureLaura PalotásNo ratings yet
- Pervasive Developmental Disorders - Indian SceneDocument11 pagesPervasive Developmental Disorders - Indian SceneVijay DasNo ratings yet
- Notes of CH 10 Gravitation - Class 9th ScienceDocument19 pagesNotes of CH 10 Gravitation - Class 9th ScienceAnujNo ratings yet
- Key To Kanji Sample - 4Document14 pagesKey To Kanji Sample - 4nastusha sunshaNo ratings yet
- KaizenDocument5 pagesKaizenMaison_Orion_9800No ratings yet
- Full Test Bank For Statistics For Business Economics 14Th by Anderson PDF Docx Full Chapter ChapterDocument6 pagesFull Test Bank For Statistics For Business Economics 14Th by Anderson PDF Docx Full Chapter Chapterjoshuaperkinsobjpadfmyx100% (13)
- Transition PlanDocument5 pagesTransition Planapi-634378436No ratings yet
- 21mat11 2Document4 pages21mat11 2Fathima Syed MaqsoodNo ratings yet
- Differentiated-Instruction NotesDocument15 pagesDifferentiated-Instruction NotesMontenegro Roi VincentNo ratings yet
- Report Major Project by ShubhamDocument45 pagesReport Major Project by ShubhamYash KakranNo ratings yet
- FSF2D Course Handout 2015 2016Document7 pagesFSF2D Course Handout 2015 2016Elizabeth ProvostNo ratings yet
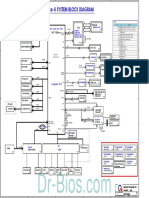
- Zaaa Serials Skylake-U System Block Diagram: Sky Lake Ult 15WDocument48 pagesZaaa Serials Skylake-U System Block Diagram: Sky Lake Ult 15Wzawnaing soe08No ratings yet
- Math Interns - LESSON-PLANDocument6 pagesMath Interns - LESSON-PLANLESTER PARADILLONo ratings yet
- ICGSE Y8 Maths Progression Test Mid-Year (Chapter1-11)Document10 pagesICGSE Y8 Maths Progression Test Mid-Year (Chapter1-11)YAP LEE KHIMNo ratings yet
- Anecdotal Record Assestment FormDocument3 pagesAnecdotal Record Assestment FormMerilyn AngNo ratings yet
- Expert Classes I Offer OnDocument2 pagesExpert Classes I Offer OnLearnItLiveNo ratings yet
- Registered Nurse - RNDocument11 pagesRegistered Nurse - RNMaurinus DickyNo ratings yet
- Assessment in Corn Farming in DA-MAFAR in Upi, MaguindanaoDocument7 pagesAssessment in Corn Farming in DA-MAFAR in Upi, MaguindanaoAff ReyylNo ratings yet
- Introduction To Management and OrganizationsDocument16 pagesIntroduction To Management and OrganizationslunapanozoNo ratings yet
- FINAL - Corporate Brochure - MACEE Fulbright Malaysia - (For Print) PDFDocument40 pagesFINAL - Corporate Brochure - MACEE Fulbright Malaysia - (For Print) PDFMaisara MalekNo ratings yet
- Week 2 Day 1 GRADE 8Document2 pagesWeek 2 Day 1 GRADE 8Anonymous yElhvOhPnNo ratings yet
- Short Course in Social Work at UnisaDocument8 pagesShort Course in Social Work at Unisaafjwftijfbwmen100% (2)
- KISTERS License Server Admin Guide 3Document12 pagesKISTERS License Server Admin Guide 3Çağatay AbayNo ratings yet
- Grades 1 To 12 Daily Lesson Log School: Grade Level Teacher Learning Area Teaching Dates & Time QuarterDocument5 pagesGrades 1 To 12 Daily Lesson Log School: Grade Level Teacher Learning Area Teaching Dates & Time QuarterJohnCzyril Deladia DomensNo ratings yet
- Lauren Carew ResumeDocument1 pageLauren Carew ResumeLauren CarewNo ratings yet
- DLL 6Document2 pagesDLL 6arlene aliporoNo ratings yet
- What Are TRP RatingsDocument2 pagesWhat Are TRP Ratingsshoebkhan1No ratings yet
- The Influence of Learning Strategy On Ability Reading Understanding of Students Grade 4 in Basic SchoolDocument5 pagesThe Influence of Learning Strategy On Ability Reading Understanding of Students Grade 4 in Basic SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet