Download as pdf or txt
You might also like
- Full Download Solution Manual For Discrete Mathematics With Applications 5th Edition Susanna S Epp PDF Full ChapterDocument36 pagesFull Download Solution Manual For Discrete Mathematics With Applications 5th Edition Susanna S Epp PDF Full Chapterrabate.toiler.vv5s092% (24)
- Statistics and Data Analysis in Geology (3rd - Ed.)Document257 pagesStatistics and Data Analysis in Geology (3rd - Ed.)Jorge Orejarena Garcia71% (35)
- Nursing Care Plan - ConstipationDocument2 pagesNursing Care Plan - Constipationderic86% (72)
- Assignment# 9-10uploadDocument6 pagesAssignment# 9-10uploadneha100% (2)
- CITICOLINE, Drugs in MedicalDocument10 pagesCITICOLINE, Drugs in MedicalInosanto May AnnNo ratings yet
- Statement of PurposeDocument2 pagesStatement of PurposeNazmul Hasan71% (7)
- Drug Study (Ranitidine, Metoclopramide, Ketorolac, and Omeprazole)Document8 pagesDrug Study (Ranitidine, Metoclopramide, Ketorolac, and Omeprazole)Akisan0% (1)
- Nursing Care Plan ConstipationDocument2 pagesNursing Care Plan ConstipationkazelleNo ratings yet
- NCP ConstipationDocument2 pagesNCP ConstipationFaith Bingan Remiscal67% (6)
- RanitidineDocument2 pagesRanitidineHarvey BanagNo ratings yet
- Drug Study - BisacodylDocument4 pagesDrug Study - BisacodylKyla CastroNo ratings yet
- Constipation NCPDocument3 pagesConstipation NCPSeth Amiel MotaNo ratings yet
- General Indications: BeforeDocument24 pagesGeneral Indications: Beforelouie john abilaNo ratings yet
- Constipation NCPDocument2 pagesConstipation NCPAbby GonzalesNo ratings yet
- Drug StudyDocument8 pagesDrug Studyzhapper2002No ratings yet
- MEDSURG 1 NotesDocument43 pagesMEDSURG 1 NotesNEIL NETTE S. REYNALDONo ratings yet
- SUMAOANG - Maalox Drug StudyDocument4 pagesSUMAOANG - Maalox Drug StudyMina SumaoangNo ratings yet
- Hirschsprung Disease (Congenital Aganglionic Megacolon) : By: Romeo Benjamin D. Laurente Group 4 BSN-2ADocument11 pagesHirschsprung Disease (Congenital Aganglionic Megacolon) : By: Romeo Benjamin D. Laurente Group 4 BSN-2ARob Romeo Benjamin LaurenteNo ratings yet
- Drug Study Camillus MabiniDocument5 pagesDrug Study Camillus MabiniJonh Carlo LopezNo ratings yet
- CPH 1902 Group PresentationDocument15 pagesCPH 1902 Group PresentationNicole MicallefNo ratings yet
- DRUG STUDY F 1Document18 pagesDRUG STUDY F 1Kolimlim, Marienne SD.No ratings yet
- OmeprazoleDocument1 pageOmeprazolejennelyn losantaNo ratings yet
- OmeprazoleDocument2 pagesOmeprazoleIvan Matthew SuperioNo ratings yet
- Drug Study (Med Ward Duty)Document6 pagesDrug Study (Med Ward Duty)Kimberly Abellar LatoNo ratings yet
- Drug StudyDocument4 pagesDrug StudyMelody Forca FranciscoNo ratings yet
- Drug StudyDocument2 pagesDrug StudyKimberly Abellar LatoNo ratings yet
- Drug StudyDocument2 pagesDrug Studyjennelyn losantaNo ratings yet
- NCP Ruth DeveraDocument8 pagesNCP Ruth DeveraBESA JERIC FLORESNo ratings yet
- ConstipationDocument4 pagesConstipationprincess_bee100% (1)
- Lactulose Drug StudyDocument1 pageLactulose Drug StudyJhanine ArellanoNo ratings yet
- Lida AjocDocument10 pagesLida AjocEzra Knight Llesis AcebedoNo ratings yet
- Drug StudyDocument5 pagesDrug StudyGAYOL BREEN IRAH A.No ratings yet
- Waiters Morphine PDFDocument2 pagesWaiters Morphine PDFmp1757No ratings yet
- ConstipationDocument3 pagesConstipationmyer pasandalanNo ratings yet
- DS - Senokot ForteDocument1 pageDS - Senokot ForteMarjorie Dela RosaNo ratings yet
- DIARRHEADocument2 pagesDIARRHEADanielNo ratings yet
- Drug Mechanism of Action Indication Contraindication Adverse Effects Nursing Responsibility BetahistineDocument16 pagesDrug Mechanism of Action Indication Contraindication Adverse Effects Nursing Responsibility Betahistineclydell joyce masiarNo ratings yet
- Drug StudyDocument14 pagesDrug StudyWendy EscalanteNo ratings yet
- GI Motility DrugsDocument1 pageGI Motility DrugspulmonologistNo ratings yet
- University of Eastern Philippines: University Town, Northern SamarDocument5 pagesUniversity of Eastern Philippines: University Town, Northern SamarJane MinNo ratings yet
- Drug Senno Sides SennaDocument1 pageDrug Senno Sides SennaSrkocherNo ratings yet
- Individual Case Study (1st Sem 1st Rotation) - Drug StudyDocument3 pagesIndividual Case Study (1st Sem 1st Rotation) - Drug StudyMichael Gino SarenasNo ratings yet
- Nursing Care Plan ConstipationDocument2 pagesNursing Care Plan ConstipationGio Baduria100% (1)
- Drug Study (V.luna)Document4 pagesDrug Study (V.luna)carizzajoyNo ratings yet
- Diarrhea Nursing Care PlanDocument2 pagesDiarrhea Nursing Care PlanKrizha Angela NicolasNo ratings yet
- Drug Study OR RLEDocument13 pagesDrug Study OR RLEVannesa TarifaNo ratings yet
- Benztrop, Congentin: Drug StudyDocument4 pagesBenztrop, Congentin: Drug StudyHamimah Bint AliNo ratings yet
- ConstipationDocument6 pagesConstipationاحمد محمدNo ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationMara Jon Ocden CasibenNo ratings yet
- DilantinDocument2 pagesDilantinMarinel AgultoNo ratings yet
- Nursing DiagnosisDocument9 pagesNursing DiagnosisSkyerexNo ratings yet
- The Complete Guide to Chronic Constipation: Symptoms, Risks, Treatments & CuresFrom EverandThe Complete Guide to Chronic Constipation: Symptoms, Risks, Treatments & CuresNo ratings yet
- Intestinal Failure: Diagnosis, Management and TransplantationFrom EverandIntestinal Failure: Diagnosis, Management and TransplantationAlan LangnasNo ratings yet
- Gastric Band Hypnosis For Women: How To Burn Fat, Stop Disordered And Emotional Eating Through Positive Affirmations, Guided Meditation, And Self-Hypnosis Without The Risk Of Gastric Band SurgeryFrom EverandGastric Band Hypnosis For Women: How To Burn Fat, Stop Disordered And Emotional Eating Through Positive Affirmations, Guided Meditation, And Self-Hypnosis Without The Risk Of Gastric Band SurgeryRating: 5 out of 5 stars5/5 (3)
- A Simple Guide to Esophagus Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Esophagus Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- The Dyspepsia Mastery Bible: Your Blueprint For Complete Dyspepsia ManagementFrom EverandThe Dyspepsia Mastery Bible: Your Blueprint For Complete Dyspepsia ManagementNo ratings yet
- Incontinence a Time to Heal with Yoga and Acupressure: A Six Week Exercise Program for People with Simple Stress Urinary IncontinenceFrom EverandIncontinence a Time to Heal with Yoga and Acupressure: A Six Week Exercise Program for People with Simple Stress Urinary IncontinenceNo ratings yet
- Food Is Figureoutable: AN ESSENTIAL GUIDE TO BODY SYSTEMSFrom EverandFood Is Figureoutable: AN ESSENTIAL GUIDE TO BODY SYSTEMSNo ratings yet
- Gut-Level Conversations: Pediatric Gastroenterology for the Primary Care ProviderFrom EverandGut-Level Conversations: Pediatric Gastroenterology for the Primary Care ProviderNo ratings yet
- A Guide To Managing InfertilityDocument38 pagesA Guide To Managing InfertilitynehaNo ratings yet
- Liberty Construction College: Student Assessment - Written ActivityDocument12 pagesLiberty Construction College: Student Assessment - Written ActivitynehaNo ratings yet
- 2437 The Complex Path To Simple Elegance The Story of 432 Park AvenueDocument7 pages2437 The Complex Path To Simple Elegance The Story of 432 Park AvenuenehaNo ratings yet
- 53 Hamada Et Al Genetics and Male InfertilityDocument45 pages53 Hamada Et Al Genetics and Male InfertilitynehaNo ratings yet
- Comprehensive Overview of Constipation: William E. Whitehead, PHD Center Co-DirectorDocument3 pagesComprehensive Overview of Constipation: William E. Whitehead, PHD Center Co-DirectornehaNo ratings yet
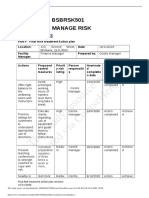
- This Study Resource Was: Unit Code: Bsbrsk501 Unit Name: Manage RiskDocument2 pagesThis Study Resource Was: Unit Code: Bsbrsk501 Unit Name: Manage RisknehaNo ratings yet
- Assessment Task 1 Unit Code: BSBMKG523 Unit Name: Design and Develop An Integrated Marketing Communication PlanDocument12 pagesAssessment Task 1 Unit Code: BSBMKG523 Unit Name: Design and Develop An Integrated Marketing Communication PlannehaNo ratings yet
- Improvement and Support Plan (ISP)Document3 pagesImprovement and Support Plan (ISP)nehaNo ratings yet
- This Study Resource Was: ASSESSMENT 2 - Written ReportDocument9 pagesThis Study Resource Was: ASSESSMENT 2 - Written ReportnehaNo ratings yet
- Pes Anserine BursitisDocument4 pagesPes Anserine BursitisnehaNo ratings yet
- BSBMGT617 Format of AssessmentDocument8 pagesBSBMGT617 Format of AssessmentnehaNo ratings yet
- Worksheet Pharaohs, Pyramids and The World of The GodsDocument9 pagesWorksheet Pharaohs, Pyramids and The World of The GodsnehaNo ratings yet
- Photocopiable Resources: Macmillan Children's Readers Worksheets and Teacher's NotesDocument8 pagesPhotocopiable Resources: Macmillan Children's Readers Worksheets and Teacher's NotesnehaNo ratings yet
- Voslp /F 38: Overcenter ValvesDocument2 pagesVoslp /F 38: Overcenter ValvesSachin RamadasanNo ratings yet
- Assessment of Temporal Hydrological Variations Due To Land Use Changes Using Remote Sensing/GISDocument38 pagesAssessment of Temporal Hydrological Variations Due To Land Use Changes Using Remote Sensing/GISWubieNo ratings yet
- Cyctocyle - Care PlanDocument22 pagesCyctocyle - Care Planarchana vermaNo ratings yet
- Standard DC Output: Simplified Internal Diagram of The Charger's Output ConnectionsDocument1 pageStandard DC Output: Simplified Internal Diagram of The Charger's Output ConnectionstoufikNo ratings yet
- Chapter#3 - Assignmnet ProblemDocument36 pagesChapter#3 - Assignmnet ProblemHarishNo ratings yet
- Intermediate Accounting Reporting and Analysis 3Rd Edition James Wahlen Full ChapterDocument67 pagesIntermediate Accounting Reporting and Analysis 3Rd Edition James Wahlen Full Chapterwilliam.rodriquez579100% (6)
- REPORT Multiple DisabilitiesDocument8 pagesREPORT Multiple DisabilitiesIrene FriasNo ratings yet
- Marketing Plan: GoldilocksDocument18 pagesMarketing Plan: GoldilocksAkhia Visitacion100% (1)
- 2021 DBaaS Security Architect and SolutionsDocument26 pages2021 DBaaS Security Architect and Solutionsluke luNo ratings yet
- IAL Business Studies (COPYRIGHT REMOVED) WBS03 01 Jan 2014Document20 pagesIAL Business Studies (COPYRIGHT REMOVED) WBS03 01 Jan 2014shamimahNo ratings yet
- Is 228 9 1989Document8 pagesIs 228 9 1989Andrewz PachuauNo ratings yet
- Briggs-Myers Personality Test and Careers: MindDocument2 pagesBriggs-Myers Personality Test and Careers: Mindapi-378982090No ratings yet
- 03 Product SpecificationDocument10 pages03 Product Specificationxor_45No ratings yet
- FOSFA Technical Manual Oils and FatsDocument15 pagesFOSFA Technical Manual Oils and FatsNurhayati SurbaktiNo ratings yet
- Talent Scout Test Body Mass ARM Span Basketball Throw Agility RUN 40 Metre SprintDocument6 pagesTalent Scout Test Body Mass ARM Span Basketball Throw Agility RUN 40 Metre SprintSoekemalNo ratings yet
- Chapter 10 - Eco LiteracyDocument15 pagesChapter 10 - Eco LiteracyMichelle Bandoquillo100% (1)
- Absolute C 6th Edition Savitch Test BankDocument36 pagesAbsolute C 6th Edition Savitch Test Bankproteosemolehill.g1n1h100% (25)
- NOVATHERABBITPATTERNDocument10 pagesNOVATHERABBITPATTERNTejidos Castillo Amigurumis con Amor100% (3)
- PRojectDocument61 pagesPRojectAditya SalunkheNo ratings yet
- Expt. 8 Salivary DigestionDocument25 pagesExpt. 8 Salivary DigestionLESLIE JANE BALUYOS JALANo ratings yet
- CadburyDocument24 pagesCadburyDeepti Mangal50% (2)
- Westinghouse Style-Tone Mercury Vapor Lamps Bulletin 1975Document2 pagesWestinghouse Style-Tone Mercury Vapor Lamps Bulletin 1975Alan MastersNo ratings yet
- ASM Interview QuestionDocument14 pagesASM Interview QuestiondayascNo ratings yet
- Aaroure: Salah EddineDocument2 pagesAaroure: Salah EddineAy OùbNo ratings yet
- Principles of Electricity PDFDocument371 pagesPrinciples of Electricity PDFJohn C. Stephens100% (5)
- Irctcs E-Ticketing Service Electronic Reservation Slip (Personal User)Document1 pageIrctcs E-Ticketing Service Electronic Reservation Slip (Personal User)Jay ParkheNo ratings yet
- Care Sheet - Neon Tree Dragon (Japalura Splendida)Document2 pagesCare Sheet - Neon Tree Dragon (Japalura Splendida)John Gamesby100% (1)