Download as pdf or txt
You might also like
- Use This Assumption of LiabilityDocument7 pagesUse This Assumption of LiabilityBleak NarrativesNo ratings yet
- Living Will TemplateDocument2 pagesLiving Will Templatesaucolcous60% (5)
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- JAnaesthClinPharmacol294459-335648 091924 PDFDocument6 pagesJAnaesthClinPharmacol294459-335648 091924 PDFaltaikhsannurNo ratings yet
- Critical AppraisalDocument13 pagesCritical AppraisalRatna Widiyanti KNo ratings yet
- Comparison of Hyperbaric Levobupivacaine/ Bupivacaine For Ceserean SectionDocument6 pagesComparison of Hyperbaric Levobupivacaine/ Bupivacaine For Ceserean SectionIJAR JOURNALNo ratings yet
- 2264-Article Text-5024-4-10-20151024Document6 pages2264-Article Text-5024-4-10-20151024shivamNo ratings yet
- Dexme IntratechalDocument5 pagesDexme IntratechalDianWindiAmaliaNo ratings yet
- Priyanka New PPT Final 2-1Document49 pagesPriyanka New PPT Final 2-1sourabh jakharNo ratings yet
- Comparison of Analgesic Effects of Intravenous Nalbuphine and Pentazocine in Patients Posted For Short-Duration Surgeries A Prospective Randomized Double-Blinded StudyDocument4 pagesComparison of Analgesic Effects of Intravenous Nalbuphine and Pentazocine in Patients Posted For Short-Duration Surgeries A Prospective Randomized Double-Blinded StudyMuhammad AtifNo ratings yet
- Plan of Dissertation-MadhaviDocument18 pagesPlan of Dissertation-MadhaviVijay ChhillarNo ratings yet
- HindawiDocument6 pagesHindawiTaufiqo Nugraha SjachrilNo ratings yet
- Arp2018 1486261Document5 pagesArp2018 1486261Sheren ElinNo ratings yet
- SynopsisDocument14 pagesSynopsisAqeel AhmadNo ratings yet
- Effectiveness of Fascia Iliaca Compartment Block For Post Operative Analgesia After Surgery For Femur Bone FractureDocument12 pagesEffectiveness of Fascia Iliaca Compartment Block For Post Operative Analgesia After Surgery For Femur Bone FractureIJAR JOURNALNo ratings yet
- Prediction of Hypotension Using PerfusioDocument6 pagesPrediction of Hypotension Using PerfusioachyutsharmaNo ratings yet
- Jurnal 3 ACBTDocument4 pagesJurnal 3 ACBTMuhamad Elfitra SalamNo ratings yet
- Surgery 23 3 1Document6 pagesSurgery 23 3 1razaqhussain00No ratings yet
- Levobupivacaine and Bupivacaine in Spinal Anesthesia For Transurethral Endoscopic SurgeryDocument7 pagesLevobupivacaine and Bupivacaine in Spinal Anesthesia For Transurethral Endoscopic SurgeryCassandraBussinkNo ratings yet
- Does Intravenous Low Dose Dexmedetomidine Supplementation Has Beneficial Effects On Spinal Anaesthesia?Document4 pagesDoes Intravenous Low Dose Dexmedetomidine Supplementation Has Beneficial Effects On Spinal Anaesthesia?MOHAMMED IQBALNo ratings yet
- Low Dose Levobupivacaıne 0.5% With Fentanyl in Spinal Anaesthesia For Transurethral Resection of Prostate SurgeryDocument6 pagesLow Dose Levobupivacaıne 0.5% With Fentanyl in Spinal Anaesthesia For Transurethral Resection of Prostate Surgeryblabarry1109No ratings yet
- Comparison of Surgical Outcome and Complications Between Spinal and General Anaesthesia For Patients Undergoing Percutaneous NephrolithotomyDocument5 pagesComparison of Surgical Outcome and Complications Between Spinal and General Anaesthesia For Patients Undergoing Percutaneous Nephrolithotomynaufal12345No ratings yet
- Revista Brasileira DE AnestesiologiaDocument9 pagesRevista Brasileira DE AnestesiologiayulianiNo ratings yet
- Iaim 2015 0209 02 PDFDocument9 pagesIaim 2015 0209 02 PDFPalwasha MalikNo ratings yet
- The Effectiveness of Magnesium Sulphate Intravenous Bolus or Added As An Adjunct To Ropivacaine For Brachial Plexus Block in Upper Limb Orthopaedic SurgeriesDocument7 pagesThe Effectiveness of Magnesium Sulphate Intravenous Bolus or Added As An Adjunct To Ropivacaine For Brachial Plexus Block in Upper Limb Orthopaedic SurgeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- IJISRT23JUN363Document7 pagesIJISRT23JUN363International Journal of Innovative Science and Research TechnologyNo ratings yet
- Erdem 2018Document9 pagesErdem 2018SFS GAMEX546No ratings yet
- Dr. - Nataraj - EJCM 132 1888 1893 2023Document7 pagesDr. - Nataraj - EJCM 132 1888 1893 2023vithz kNo ratings yet
- Jimbo 2017Document15 pagesJimbo 2017Sahily MoralesNo ratings yet
- 9829 CE (Ra) F (SH) PF1 (SNAK) PFA (P)Document4 pages9829 CE (Ra) F (SH) PF1 (SNAK) PFA (P)razaqhussain00No ratings yet
- Assessing Pain Relief Following Medical and Surgical Interventions For Lumbar Disc HerniationDocument4 pagesAssessing Pain Relief Following Medical and Surgical Interventions For Lumbar Disc HerniationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Comparative Study To Determine The Efficacy of Routine Physical Therapy Treatment With and Without Kaltenborn Mobilization On Pain and Shoulder Mobility in Frozen Shoulder PatientsDocument4 pagesA Comparative Study To Determine The Efficacy of Routine Physical Therapy Treatment With and Without Kaltenborn Mobilization On Pain and Shoulder Mobility in Frozen Shoulder Patientsfi.afifah NurNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument50 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Comparative Study of Intrathecal Sufentanil Bupivacaine Versus Intrathecal Bupivacaine in Patients Undergoing Elective Cesarean SectionDocument5 pagesComparative Study of Intrathecal Sufentanil Bupivacaine Versus Intrathecal Bupivacaine in Patients Undergoing Elective Cesarean SectiontamiNo ratings yet
- JAnaesthClinPharmacol37163-254754 000414Document4 pagesJAnaesthClinPharmacol37163-254754 000414Ferdy RahadiyanNo ratings yet
- Effectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryDocument6 pagesEffectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Anes 10 3 9Document7 pagesAnes 10 3 9ema moralesNo ratings yet
- JPNR 2022 S01 216+ (1815 1822)Document8 pagesJPNR 2022 S01 216+ (1815 1822)prabaNo ratings yet
- Hyperbaric Spinal For Elective Cesarean Section: - Ropivacaine Vs BupivacaineDocument13 pagesHyperbaric Spinal For Elective Cesarean Section: - Ropivacaine Vs BupivacaineYayaNo ratings yet
- Research Article: Laleh Farokhmehr, Hesameddin Modir, Bijan Yazdi, Alireza Kamali, Amir Almasi-HashianiDocument7 pagesResearch Article: Laleh Farokhmehr, Hesameddin Modir, Bijan Yazdi, Alireza Kamali, Amir Almasi-HashianiAndhika DNo ratings yet
- Reduction in The Incidence of Awareness Using BIS MonitoringDocument7 pagesReduction in The Incidence of Awareness Using BIS MonitoringAlan Robinet VargasNo ratings yet
- Medi 96 E6490Document4 pagesMedi 96 E6490TheEdgeNo ratings yet
- A Comparative Study of Intravenous Paracetamol and Ketorolac For Postoperative Analgesia Following Laproscopic CholecystectomyDocument6 pagesA Comparative Study of Intravenous Paracetamol and Ketorolac For Postoperative Analgesia Following Laproscopic CholecystectomyAmrit singhNo ratings yet
- My Published Paper 7.Document4 pagesMy Published Paper 7.mir sahirNo ratings yet
- Bloqueo Pec 2 MamaDocument9 pagesBloqueo Pec 2 Mamapalomisgarcia1995No ratings yet
- Clinical StudyDocument7 pagesClinical StudymeldaerNo ratings yet
- 10 1097@eja 0000000000000642Document7 pages10 1097@eja 0000000000000642drsubramanianNo ratings yet
- PRM2017 1721460 PDFDocument6 pagesPRM2017 1721460 PDFmikoNo ratings yet
- Keywords:-Anaesthetics, Bupivacaine, Impaction, InferiorDocument8 pagesKeywords:-Anaesthetics, Bupivacaine, Impaction, InferiorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1041 4798 1 PBDocument5 pages1041 4798 1 PBBeti KristinawatiNo ratings yet
- A Prospective Study in Analgesic Effect of Distal Sodium Channel Blockers (DSCB) in Patients With SciaticaDocument5 pagesA Prospective Study in Analgesic Effect of Distal Sodium Channel Blockers (DSCB) in Patients With SciaticaInternational Journal of Innovative Science and Research Technology100% (1)
- Efficacy Lidocaine Endoscopic Submucosal DissectionDocument7 pagesEfficacy Lidocaine Endoscopic Submucosal DissectionAnonymous lSWQIQNo ratings yet
- Cervical Epidural Anaesthesia For Shoulder Arthroscopy and Effective Postoperative Physiotherapy For A Frozen Shoulder: A Case StudyDocument4 pagesCervical Epidural Anaesthesia For Shoulder Arthroscopy and Effective Postoperative Physiotherapy For A Frozen Shoulder: A Case StudySutiyono TyoNo ratings yet
- Impact of Remote Ischaemic Preconditioning On Cerebral Oxygenation During Total Knee ArthroplastyDocument8 pagesImpact of Remote Ischaemic Preconditioning On Cerebral Oxygenation During Total Knee ArthroplastySanti ParambangNo ratings yet
- Sieo Irizarry2021Document28 pagesSieo Irizarry2021Luluil MunirohNo ratings yet
- Inter Fan ZhangDocument9 pagesInter Fan ZhangrizkaNo ratings yet
- DR T. Suryasree, DR K. Indira Priya Darshini, DR PratikshaDocument9 pagesDR T. Suryasree, DR K. Indira Priya Darshini, DR PratikshaIOSRjournalNo ratings yet
- Journal PresentationDocument12 pagesJournal PresentationMANISH RAMGARHNo ratings yet
- Xia 2018Document7 pagesXia 2018Jefferson891127No ratings yet
- Enhanced Recovery After Surgery (Eras) Protocols vs. Standard Care in Patients With Peptic Ulcer PerforationDocument8 pagesEnhanced Recovery After Surgery (Eras) Protocols vs. Standard Care in Patients With Peptic Ulcer PerforationIJAR JOURNALNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Atlas of Early Neoplasias of the Gastrointestinal Tract: Endoscopic Diagnosis and Therapeutic DecisionsFrom EverandAtlas of Early Neoplasias of the Gastrointestinal Tract: Endoscopic Diagnosis and Therapeutic DecisionsFrieder BerrNo ratings yet
- Pedro Carreño: SkillsDocument1 pagePedro Carreño: Skillsapi-253966222No ratings yet
- Incident vs. Prevalent Cases and Measures of OccurrenceDocument3 pagesIncident vs. Prevalent Cases and Measures of OccurrenceRenzo FernandezNo ratings yet
- MediCard List of Accredited Providers Aug 2022Document156 pagesMediCard List of Accredited Providers Aug 2022Ellie HarmonieNo ratings yet
- The Effectiveness of An Oral Sensorimotor Stimulation Protocol For The Early Achievement of Exclusive Oral Feeding in Premature Infants A RandomizedDocument14 pagesThe Effectiveness of An Oral Sensorimotor Stimulation Protocol For The Early Achievement of Exclusive Oral Feeding in Premature Infants A RandomizedJUAN CARLOSNo ratings yet
- Ethio HDSDocument93 pagesEthio HDSberhanu nathanielNo ratings yet
- VIS Shingles-RecombinantDocument2 pagesVIS Shingles-RecombinantAlmira MenggeNo ratings yet
- IDM/HND/System Analysis Page 1 of 5Document5 pagesIDM/HND/System Analysis Page 1 of 5ChiranSJNo ratings yet
- Prepared By:: A.rajashekarDocument27 pagesPrepared By:: A.rajashekarAkhil SharmaNo ratings yet
- LFE Report Group 11Document40 pagesLFE Report Group 11Avishake SahaNo ratings yet
- SUBSTANCE ABUSE & MISUSE: NarcoticsDocument2 pagesSUBSTANCE ABUSE & MISUSE: Narcoticsjgstorandt44No ratings yet
- Block I (Paper I) Blueprint (Theory & OSPE - OSCE)Document2 pagesBlock I (Paper I) Blueprint (Theory & OSPE - OSCE)Danyal AzamNo ratings yet
- Medical Services Plan: Online: by PhoneDocument2 pagesMedical Services Plan: Online: by Phoneian pierceNo ratings yet
- Health Information Systems Utilization: A Comparison of Extent and Magnitude in Public and Private Health Facilities in Dar Es Salaam, TanzaniaDocument10 pagesHealth Information Systems Utilization: A Comparison of Extent and Magnitude in Public and Private Health Facilities in Dar Es Salaam, TanzaniaAJHSSR JournalNo ratings yet
- Paediatric Digestive Health Across Europe: Early Nutrition, Liver Disease and Inflammatory Bowel DiseaseDocument20 pagesPaediatric Digestive Health Across Europe: Early Nutrition, Liver Disease and Inflammatory Bowel DiseaseVasoRafaelaVakouftsiNo ratings yet
- Sick Enough PDFDocument277 pagesSick Enough PDFSelena TomaNo ratings yet
- Dengue EditedDocument112 pagesDengue EditedMarvin Yebes ArceNo ratings yet
- LEXICON International Media Guide For Mental Health - FINAL - LexiconDocument16 pagesLEXICON International Media Guide For Mental Health - FINAL - LexiconVaishnavi JayakumarNo ratings yet
- Roadmap ICT Topsectoren 4 0Document60 pagesRoadmap ICT Topsectoren 4 0abey134175No ratings yet
- Adolescent HealthDocument47 pagesAdolescent Healthsushma100% (1)
- Case Report Interdisciplinary Approach For Closure and Prevention of Relapse in A Case of Maxillary Midline Diastema-A Case ReportDocument4 pagesCase Report Interdisciplinary Approach For Closure and Prevention of Relapse in A Case of Maxillary Midline Diastema-A Case ReportPinky TolaniNo ratings yet
- 2014 Internal COC PharmaDocument16 pages2014 Internal COC PharmategenezewudeNo ratings yet
- Epidemiology of Cutaneous Melanoma in Germany and Worldwide: Claus Garbe Andreas BlumDocument11 pagesEpidemiology of Cutaneous Melanoma in Germany and Worldwide: Claus Garbe Andreas BlumGabriela AgrigNo ratings yet
- Kenya Relief Grant ProposalDocument31 pagesKenya Relief Grant ProposalgyrichardNo ratings yet
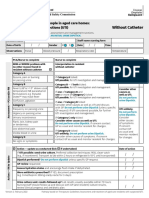
- Form Ams Clinical Pathway Fillable Form Without CatheterDocument1 pageForm Ams Clinical Pathway Fillable Form Without CatheterTeenu JobyNo ratings yet
- Toaz - Info Answer and Rationale Psychiatric Nursing PR 4Document1 pageToaz - Info Answer and Rationale Psychiatric Nursing PR 4MimiNo ratings yet
- EldermistreatmentandabusepaperDocument8 pagesEldermistreatmentandabusepaperapi-353301076No ratings yet
- Skilled Occupation List (SOL) : Schedule 1: Australian Government Department of Immigration and CitizenshipDocument6 pagesSkilled Occupation List (SOL) : Schedule 1: Australian Government Department of Immigration and Citizenshipmd abNo ratings yet
- Physical Education and HealthDocument2 pagesPhysical Education and HealthSHERWIN BERMEJONo ratings yet