Download as pdf or txt
You might also like
- Hesi Review For Health AssessmentDocument18 pagesHesi Review For Health AssessmentJennifer Portillo100% (19)
- OB Nursing NotesDocument101 pagesOB Nursing NotesNur Sanaani100% (2)
- Course Title Course Code Course Description Prerequisites Course Credit Placement Program OutcomeDocument10 pagesCourse Title Course Code Course Description Prerequisites Course Credit Placement Program OutcomeNur Sanaani100% (1)
- Anxious in LoveDocument17 pagesAnxious in LoveNew Harbinger Publications80% (5)
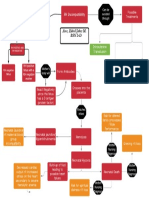
- Basic Concept Map - RH IncompatibilityDocument1 pageBasic Concept Map - RH IncompatibilityTechnoShindoNo ratings yet
- NCM 112 Lec Midterm Unit TestDocument5 pagesNCM 112 Lec Midterm Unit TestJULIANA PANGILINANNo ratings yet
- OCHONDRA CA - FinalExam - 2020Document15 pagesOCHONDRA CA - FinalExam - 2020joyrena ochondraNo ratings yet
- Why Join PNADocument2 pagesWhy Join PNADarren CariñoNo ratings yet
- Diagnostic Exam - NP1Document18 pagesDiagnostic Exam - NP1ogiskuadz100% (1)
- Preboard Angelus Victus Test 4Document16 pagesPreboard Angelus Victus Test 4Alpro ZamboNo ratings yet
- Risk Reduction and Preparedness Equipment ProtectDocument2 pagesRisk Reduction and Preparedness Equipment ProtectR ArcegaNo ratings yet
- Iv Fluid Sheet: Bautista A 58 2021-0000025 Milagros F Medical Ward-207Document1 pageIv Fluid Sheet: Bautista A 58 2021-0000025 Milagros F Medical Ward-207Renea Joy ArruejoNo ratings yet
- Geria Post Test AnswersDocument3 pagesGeria Post Test AnswersMarco AglibotNo ratings yet
- Rinciples and Practice of The HospiceDocument1 pageRinciples and Practice of The HospiceCake ManNo ratings yet
- Sanaani Nur Hathi M. Nso Jugular Venous Oximetry Staff Nurse 1Document7 pagesSanaani Nur Hathi M. Nso Jugular Venous Oximetry Staff Nurse 1Nur SanaaniNo ratings yet
- FNCP TB As A Health DeficitDocument5 pagesFNCP TB As A Health Deficitkuu faalNo ratings yet
- NCP Micu Hascvd Cad - RioDocument5 pagesNCP Micu Hascvd Cad - RioRio BonifacioNo ratings yet
- Cefipime HCL (AXERA)Document2 pagesCefipime HCL (AXERA)Kristine YoungNo ratings yet
- Assessment and Management of Patients With Hearing and Balance Disorders WebDocument36 pagesAssessment and Management of Patients With Hearing and Balance Disorders Webmalinda0% (1)
- NCM 114: Care of The Older Adult Instructor: Gino Paulo A. Buizon, R.NDocument9 pagesNCM 114: Care of The Older Adult Instructor: Gino Paulo A. Buizon, R.NJay VillasotoNo ratings yet
- NCM 117 Final Exam MamelDocument16 pagesNCM 117 Final Exam MamelJade CentinoNo ratings yet
- Nursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NDocument2 pagesNursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NnananaNo ratings yet
- MNAP Military Nursing in The Philippines May Be Said To Have Existed As Early As 1896 When The Legendary Tandang Sora Took Care of The Sick and WoundedDocument4 pagesMNAP Military Nursing in The Philippines May Be Said To Have Existed As Early As 1896 When The Legendary Tandang Sora Took Care of The Sick and WoundedarjeighNo ratings yet
- Case 3 Care of Client With GI, PUD, Cancer, Liver FailureDocument33 pagesCase 3 Care of Client With GI, PUD, Cancer, Liver FailureNyeam NyeamNo ratings yet
- Inp Eval ExamDocument3 pagesInp Eval Examd1choosenNo ratings yet
- Operating Room WriteDocument2 pagesOperating Room WritemodiNo ratings yet
- Doctors Order LoveDocument4 pagesDoctors Order LoveAubrey Unique EvangelistaNo ratings yet
- Objectives - Surgical WardDocument3 pagesObjectives - Surgical WardAzhly AntenorNo ratings yet
- Aminogen Drug StudyDocument2 pagesAminogen Drug Studymilesmin100% (1)
- Family Nursing Care Plan - Cough and ColdsDocument1 pageFamily Nursing Care Plan - Cough and ColdsArnx QuilonNo ratings yet
- Diagnostic Exam - NP5Document19 pagesDiagnostic Exam - NP5ogiskuadzNo ratings yet
- NCP Ch31 p991-992Document2 pagesNCP Ch31 p991-992Ala'a Abd Mansor100% (2)
- Ivf StudyDocument1 pageIvf StudyjeliinNo ratings yet
- FNCPDocument5 pagesFNCPCarina QuibinitNo ratings yet
- Peach and Green Organic Shapes Meditation Workshop Webinar Keynote PresentationDocument7 pagesPeach and Green Organic Shapes Meditation Workshop Webinar Keynote PresentationNicole Ivy GorimoNo ratings yet
- Female Perineal CareDocument8 pagesFemale Perineal CareMushy_ayaNo ratings yet
- Kardex: Date/ Time Medications Date Treatment/ ManagementDocument2 pagesKardex: Date/ Time Medications Date Treatment/ ManagementJuviely PremacioNo ratings yet
- FDAR ChartingDocument2 pagesFDAR Chartinglouie roderosNo ratings yet
- Drugs Mechanism of Action Nursing Responsibilities OMXDocument5 pagesDrugs Mechanism of Action Nursing Responsibilities OMXEmmanuelRodriguezNo ratings yet
- NCP Knowledge DeficitDocument2 pagesNCP Knowledge DeficitPrincess Faniega SugatonNo ratings yet
- Components of FHSISDocument3 pagesComponents of FHSISraquel maniegoNo ratings yet
- Cholecystectomy Nursing Care Plan: Intraoperative Problem: Risk For AspirationDocument1 pageCholecystectomy Nursing Care Plan: Intraoperative Problem: Risk For AspirationJess GoNo ratings yet
- F - Case Scenario Peritoneal Dialysis - PDF - 173767042Document5 pagesF - Case Scenario Peritoneal Dialysis - PDF - 173767042yumulNo ratings yet
- NCPDocument1 pageNCPEve DelosoNo ratings yet
- Chn-Herbal MedicineDocument5 pagesChn-Herbal MedicineBSN 1-N CASTRO, RicciNo ratings yet
- Drug Study SARAHDocument2 pagesDrug Study SARAHirene Joy DigaoNo ratings yet
- Hyperthermia Pneumonia Nursing Care PlanDocument1 pageHyperthermia Pneumonia Nursing Care PlanLegendX100% (1)
- Psychiatric Nursing (Post-Lecture Examination)Document19 pagesPsychiatric Nursing (Post-Lecture Examination)Kristel Alyssa MarananNo ratings yet
- Discontinuing IvDocument2 pagesDiscontinuing IvJamaica Leslie NovenoNo ratings yet
- Soapie Charting: Date, Time, and Shift Progress NotesDocument3 pagesSoapie Charting: Date, Time, and Shift Progress NotesBianx Flores DosdosNo ratings yet
- Post Test - Psych-Prof. Alviz - SCDocument4 pagesPost Test - Psych-Prof. Alviz - SCKristen FajilanNo ratings yet
- IDPS Chapter 15Document10 pagesIDPS Chapter 15002No ratings yet
- 12 Health Indicator LegendsDocument4 pages12 Health Indicator LegendsEmman TeewaiNo ratings yet
- Demography: Sources of Demographic DataDocument8 pagesDemography: Sources of Demographic DataSHERMINA HASANNo ratings yet
- Discharge PlanDocument9 pagesDischarge PlanRheynel NietesNo ratings yet
- Nursing Care Plan: Sweating Temperature Rigors Nausea Vomiting Diarrhoea Lethargy MalaiseDocument1 pageNursing Care Plan: Sweating Temperature Rigors Nausea Vomiting Diarrhoea Lethargy Malaise06eltianNo ratings yet
- Drug Study RopivacaineDocument2 pagesDrug Study Ropivacainerica sebabillonesNo ratings yet
- NCP Infection NewDocument3 pagesNCP Infection NewXerxes DejitoNo ratings yet
- SITUATION: Wide Knowledge About The Human Ear, Its Parts and Its Functions Will Help A NurseDocument2 pagesSITUATION: Wide Knowledge About The Human Ear, Its Parts and Its Functions Will Help A NurseWiljohn de la CruzNo ratings yet
- Drug Study For Hepatic ABCESSDocument3 pagesDrug Study For Hepatic ABCESSEric EvangelistaNo ratings yet
- Endotracheal Intubation and Treacheastomy.Document9 pagesEndotracheal Intubation and Treacheastomy.Savita HanamsagarNo ratings yet
- Na So Faring EalDocument5 pagesNa So Faring EalDian Putri ListyantiNo ratings yet
- Ateneo de Zamboanga University: Nursing Skills Output (Nso)Document9 pagesAteneo de Zamboanga University: Nursing Skills Output (Nso)Mitzi BelamideNo ratings yet
- 4.assignment On Endo TubeDocument5 pages4.assignment On Endo Tubesantosh kumarNo ratings yet
- Nursing Research - InitialDocument25 pagesNursing Research - InitialNur SanaaniNo ratings yet
- Answer Key.Document4 pagesAnswer Key.Nur SanaaniNo ratings yet
- PediaDocument9 pagesPediaNur SanaaniNo ratings yet
- Code of Ethics For Filipino NursesDocument22 pagesCode of Ethics For Filipino NursesNur SanaaniNo ratings yet
- Nursing Care Plan For SCIDocument10 pagesNursing Care Plan For SCINur SanaaniNo ratings yet
- Management Quiz 1Document10 pagesManagement Quiz 1Reema100% (1)
- Communicable Disease NursingDocument22 pagesCommunicable Disease NursingNur SanaaniNo ratings yet
- Neurologic System Disorders: Ateneo de Zamboanga UniversityDocument2 pagesNeurologic System Disorders: Ateneo de Zamboanga UniversityNur SanaaniNo ratings yet
- A-Module 2 - EVP, CommunicationRecords Mgt.Document7 pagesA-Module 2 - EVP, CommunicationRecords Mgt.Nur SanaaniNo ratings yet
- 3 Reflection Paper in One WordDocument3 pages3 Reflection Paper in One WordNur SanaaniNo ratings yet
- Date/Week Learning Objectives Asynchronous Learning Topic Synchronous Learning TopicDocument6 pagesDate/Week Learning Objectives Asynchronous Learning Topic Synchronous Learning TopicNur SanaaniNo ratings yet
- Nephrons (Functional Unit)Document44 pagesNephrons (Functional Unit)Nur SanaaniNo ratings yet
- Module Content CHN113Document6 pagesModule Content CHN113Nur SanaaniNo ratings yet
- RRL Mental Health Adjustment and Perceived Academic Performance of Senior Highschool StudentsDocument19 pagesRRL Mental Health Adjustment and Perceived Academic Performance of Senior Highschool StudentsNur SanaaniNo ratings yet
- Rationale: Answer: C. If A Patient HasDocument12 pagesRationale: Answer: C. If A Patient HasNur SanaaniNo ratings yet
- RRL Mental Health Adjustment and Perceived Academic Performance of Senior Highschool StudentsDocument22 pagesRRL Mental Health Adjustment and Perceived Academic Performance of Senior Highschool StudentsNur Sanaani100% (1)
- Untitled DocumentDocument121 pagesUntitled DocumentNur SanaaniNo ratings yet
- RRL Mental Health Adjustment and Perceived Academic Performance of Senior Highschool StudentsDocument22 pagesRRL Mental Health Adjustment and Perceived Academic Performance of Senior Highschool StudentsNur SanaaniNo ratings yet
- Module I - Group Work (Edited)Document21 pagesModule I - Group Work (Edited)Nur SanaaniNo ratings yet
- Case Management and InnovativeDocument2 pagesCase Management and InnovativeNur SanaaniNo ratings yet
- Sanaani Nur Hathi M. Nso Jugular Venous Oximetry Staff Nurse 1Document7 pagesSanaani Nur Hathi M. Nso Jugular Venous Oximetry Staff Nurse 1Nur SanaaniNo ratings yet
- Module I - Group WorkDocument6 pagesModule I - Group WorkNur SanaaniNo ratings yet
- Module I Group WorkDocument6 pagesModule I Group WorkNur Sanaani100% (1)
- Manila Doctors Hospital v. Chua and TyDocument19 pagesManila Doctors Hospital v. Chua and Tydivine venturaNo ratings yet
- Buhner MethodDocument13 pagesBuhner Method7candlesburning100% (2)
- PART-2017-551038V1 - MDR CodesDocument11 pagesPART-2017-551038V1 - MDR CodesFranciscoNo ratings yet
- Health Education ProcessDocument25 pagesHealth Education Processdailygrind00011No ratings yet
- ANSI b301 99pdfDocument20 pagesANSI b301 99pdfstrip1No ratings yet
- PB Mental Health Snapshot 4Document5 pagesPB Mental Health Snapshot 4amanda wuNo ratings yet
- The Relationship Between Mental Disorders and Different Types of CrimeDocument15 pagesThe Relationship Between Mental Disorders and Different Types of CrimeКсенияNo ratings yet
- Research 3 Quarter 1 DLP 2Document5 pagesResearch 3 Quarter 1 DLP 2Dacel Ann EndomaNo ratings yet
- Stacy Adams Equity TheoryDocument13 pagesStacy Adams Equity TheoryFajar nNo ratings yet
- Guidelines For Maternity Care 2016Document148 pagesGuidelines For Maternity Care 2016MjunjuNo ratings yet
- Respectful Maternity CareDocument33 pagesRespectful Maternity CareJenelle Melinda TullochNo ratings yet
- HBSE-Mock ExamDocument3 pagesHBSE-Mock ExamAnneNo ratings yet
- ZEBRA Pen SDS R 301Document6 pagesZEBRA Pen SDS R 301chusqueteNo ratings yet
- 9.family Life EducationDocument7 pages9.family Life EducationVeena DalmeidaNo ratings yet
- HPV Amostras AlternativasDocument6 pagesHPV Amostras Alternativasnathaliasantosx3No ratings yet
- National Insurance Company LimitedDocument6 pagesNational Insurance Company LimitedJeet MaruNo ratings yet
- CV Nicolas Duarte Cifuentes InglesDocument2 pagesCV Nicolas Duarte Cifuentes InglesNicolas Duarte CifuentesNo ratings yet
- A. B. C. D. A. B. C. D.: Thời gian làm bài: 60 phút, không kể thời gian phát đềDocument4 pagesA. B. C. D. A. B. C. D.: Thời gian làm bài: 60 phút, không kể thời gian phát đềTruong Thi Ha Trang 1KT-19No ratings yet
- Eurasia Research Pharma Corporation: e Effective SupersedesDocument10 pagesEurasia Research Pharma Corporation: e Effective SupersedesErine FelipeNo ratings yet
- Freedom Forever!: PMO Hacknotes For Those Still Slipping UpDocument13 pagesFreedom Forever!: PMO Hacknotes For Those Still Slipping Upmeh3reNo ratings yet
- English 7 q1 m7 EditedDocument11 pagesEnglish 7 q1 m7 EditedShei La Ma RieNo ratings yet
- Shell Advance 4T AX5 10W-30 (SL/MA) : Performance, Features & Benefits Specifications, Approvals & RecommendationsDocument2 pagesShell Advance 4T AX5 10W-30 (SL/MA) : Performance, Features & Benefits Specifications, Approvals & RecommendationsandriNo ratings yet
- Uncertainity Illness Theory (Merle H.mishel)Document50 pagesUncertainity Illness Theory (Merle H.mishel)Taate Mohammed100% (1)
- 2021 ESC Preporuke Za Srčani Pejsing I Srčanu Resinhronizacionu TerapijuDocument68 pages2021 ESC Preporuke Za Srčani Pejsing I Srčanu Resinhronizacionu TerapijuDaria Lily MićanovićNo ratings yet
- Luma - Health Insurance Quotation - May Kabyar Oo (3 Options)Document3 pagesLuma - Health Insurance Quotation - May Kabyar Oo (3 Options)Kabyar MayNo ratings yet
- Risk Assessment - Placing of Transformer - TTSDocument6 pagesRisk Assessment - Placing of Transformer - TTSnsadnan100% (2)
- Report On The Transition From Institutional Care To Community-Based Services in 27 Eu Member StatesDocument124 pagesReport On The Transition From Institutional Care To Community-Based Services in 27 Eu Member StatesP.Ch.O.No ratings yet
- Public Health Career GuideDocument219 pagesPublic Health Career Guidejemil l. candiladaNo ratings yet