
Classification and Management of Bile Duct Injuries: Editorial
Classification and Management of Bile Duct Injuries: Editorial
You might also like
- Atlas of Surgical Techniques in TraumaDocument364 pagesAtlas of Surgical Techniques in TraumaAgustina Zabini100% (1)
- Iatrogenic Biliary InjuriesDocument15 pagesIatrogenic Biliary InjuriessolysanNo ratings yet
- Trauma ColonDocument7 pagesTrauma Colonricardo arreguiNo ratings yet
- Tto de Ileo BiliarDocument5 pagesTto de Ileo BiliarnerisNo ratings yet
- WJG 20 13904Document8 pagesWJG 20 13904iovanela campoNo ratings yet
- 1 s2.0 S1091255X23056731 MainDocument8 pages1 s2.0 S1091255X23056731 MainPaul SantiagoNo ratings yet
- Multilevel Duodenal Injury After Blunt TraumaDocument5 pagesMultilevel Duodenal Injury After Blunt TraumaHanny RusliNo ratings yet
- Iatrogenic Hepatopancreaticobiliary Injuries: A ReviewDocument13 pagesIatrogenic Hepatopancreaticobiliary Injuries: A ReviewJohn ShipNo ratings yet
- 6 Readmission With Major AbdominalDocument10 pages6 Readmission With Major AbdominalElizabeth Mautino CaceresNo ratings yet
- Post-Cholecystectomy Acute Injury: What Can Go Wrong?Document7 pagesPost-Cholecystectomy Acute Injury: What Can Go Wrong?Ramyasree BadeNo ratings yet
- Iatrogenic Biliary Injuries: Classification, Identification, and ManagementDocument15 pagesIatrogenic Biliary Injuries: Classification, Identification, and ManagementLUISNo ratings yet
- Minimally Invasive EsophagectomyDocument5 pagesMinimally Invasive Esophagectomyfernando herbellaNo ratings yet
- Corrosive InjuryDocument6 pagesCorrosive InjuryCristian O. Saavedra RodriguezNo ratings yet
- SurgeryDocument7 pagesSurgeryFrancisco GilNo ratings yet
- International Consensus Conference On Open Abdomen in TraumaDocument11 pagesInternational Consensus Conference On Open Abdomen in TraumaCarlos HernándezNo ratings yet
- 1 s2.0 S174391910700129X MainDocument6 pages1 s2.0 S174391910700129X MainGiorgio André Gabino GonzalezNo ratings yet
- Management of Duodenal Trauma: ReviewDocument4 pagesManagement of Duodenal Trauma: ReviewAladesuruOlumideAdewaleNo ratings yet
- Pancreatitis Aguda Necrotizante Papel de La Cirugía 2017 FranciaDocument8 pagesPancreatitis Aguda Necrotizante Papel de La Cirugía 2017 FranciasergiocansecoguerraNo ratings yet
- 268 2018 Article 4642Document9 pages268 2018 Article 4642Derian TanwijayaNo ratings yet
- Post-Operative Biliary StricturesDocument7 pagesPost-Operative Biliary StricturesGeraldNo ratings yet
- 01 Editorial 6042 IngDocument2 pages01 Editorial 6042 IngJuan Mendia OssioNo ratings yet
- Baldoni 2011Document10 pagesBaldoni 2011naili nsnNo ratings yet
- Via BiliarDocument7 pagesVia Biliarahs ahnNo ratings yet
- 8 9 FistulasDocument9 pages8 9 FistulascystanarisaNo ratings yet
- Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite: DOI: 10.1590/S0100-69912014000300016Document4 pagesTbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite: DOI: 10.1590/S0100-69912014000300016Hanny RusliNo ratings yet
- Management of Duodenal Trauma: Chinese Journal of Traumatology (English Edition) February 2011Document5 pagesManagement of Duodenal Trauma: Chinese Journal of Traumatology (English Edition) February 2011dr muddssar sattarNo ratings yet
- Abdomen TraumaDocument74 pagesAbdomen TraumajeevanNo ratings yet
- Complications of Enterocystoplastycase SeriesDocument5 pagesComplications of Enterocystoplastycase SeriesIJAR JOURNALNo ratings yet
- B - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Document16 pagesB - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Battousaih1No ratings yet
- Chevallay 2020Document17 pagesChevallay 2020Maria PalNo ratings yet
- Pathophysiology and Prevention of Postoperative Peritoneal AdhesionsDocument9 pagesPathophysiology and Prevention of Postoperative Peritoneal AdhesionsFarah UlyaNo ratings yet
- Safe CholecystectomyDocument60 pagesSafe CholecystectomyCarlos Reyes100% (1)
- Penetratng InjuryDocument5 pagesPenetratng InjuryAbdulloh AbdurrohmanNo ratings yet
- Challenges in The Maagement of Pancreatic and Duodenal InjuriesDocument6 pagesChallenges in The Maagement of Pancreatic and Duodenal InjuriesOpl OplNo ratings yet
- Amilaze PredictivDocument7 pagesAmilaze PredictivDumitru RadulescuNo ratings yet
- Repair of Common Bile Duct InjuriesDocument12 pagesRepair of Common Bile Duct InjuriesDragoș PopaNo ratings yet
- Outcome of Surgical Treatment of Intestinal Perforation in Typhoid FeverDocument5 pagesOutcome of Surgical Treatment of Intestinal Perforation in Typhoid Feverdaru_qthinkNo ratings yet
- Repair of Common Bile Duct Injuries - UpToDateDocument16 pagesRepair of Common Bile Duct Injuries - UpToDateLuis Miguel Díaz VegaNo ratings yet
- Wong 2019Document11 pagesWong 2019karencuervomNo ratings yet
- A1504050119 PDFDocument19 pagesA1504050119 PDFImam Hakim SuryonoNo ratings yet
- Classification of Iatrogenic Bile Duct Injury - 2Document5 pagesClassification of Iatrogenic Bile Duct Injury - 2RameshKumarNo ratings yet
- Evaluation and Management of Splenic Injury in Blunt Abdominal TraumaDocument32 pagesEvaluation and Management of Splenic Injury in Blunt Abdominal TraumaImam Hakim SuryonoNo ratings yet
- 2012 Article 625 PDFDocument5 pages2012 Article 625 PDFPutri AdimuktiNo ratings yet
- 3Document8 pages3polomska.kmNo ratings yet
- 01 HepatogastroDocument3 pages01 Hepatogastroyacine26No ratings yet
- Acute CholangitisDocument11 pagesAcute CholangitisFrancisco EsparzaNo ratings yet
- Complicationsafter Pancreaticoduodenectomy: Robert SimonDocument10 pagesComplicationsafter Pancreaticoduodenectomy: Robert SimonŞükriye AngaNo ratings yet
- Injury Patterns and Causes of Death in 953 Patients With Penetrating Abdominal War Wounds in A Civilian Independent Non-Governmental Organization Hospital in Lashkargah, AfghanistanDocument8 pagesInjury Patterns and Causes of Death in 953 Patients With Penetrating Abdominal War Wounds in A Civilian Independent Non-Governmental Organization Hospital in Lashkargah, AfghanistanLeandro NogueiraNo ratings yet
- An Unusual Cause of Failure of Nom in Liver Trauma FinalDocument20 pagesAn Unusual Cause of Failure of Nom in Liver Trauma FinalMariyam AlblooshiNo ratings yet
- Endoscopic and Surgical Management of Iatrogenic BDocument10 pagesEndoscopic and Surgical Management of Iatrogenic BRahul SinghNo ratings yet
- Laparoscopic Cholecystectomy:An Experience of 200 Cases: Original ArticleDocument4 pagesLaparoscopic Cholecystectomy:An Experience of 200 Cases: Original ArticleAndrei GheorghitaNo ratings yet
- Jurnal Case ReportDocument3 pagesJurnal Case ReportNining Rhyanie TampubolonNo ratings yet
- Management of CBD Injury - Digestive Week Jogja 2016Document42 pagesManagement of CBD Injury - Digestive Week Jogja 2016Wisnu DipoyonoNo ratings yet
- 2015 Laparoscopic Surgery in Abdominal Trauma A Single Center Review of A 7-Year ExperienceDocument7 pages2015 Laparoscopic Surgery in Abdominal Trauma A Single Center Review of A 7-Year ExperiencejohnnhekoNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument5 pagesAnnals of Medicine and Surgery: SciencedirectMishel Rodriguez GuzmanNo ratings yet
- 1 s2.0 S0065341116000038 MainDocument12 pages1 s2.0 S0065341116000038 MainFlorin AchimNo ratings yet
- Subtotal Gastrectomy For Gastric CancerDocument15 pagesSubtotal Gastrectomy For Gastric CancerRUBEN DARIO AGRESOTTNo ratings yet
- Bile Duct InjuriesDocument24 pagesBile Duct InjuriesLUISNo ratings yet
- International Journal of Surgery Case ReportsDocument5 pagesInternational Journal of Surgery Case ReportsMuhammad Fuad MahfudNo ratings yet
- Wound: Abdominal DehiscenceDocument5 pagesWound: Abdominal DehiscencesmileyginaaNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- Surgical Treatment Options For Fecal IncontinenceDocument7 pagesSurgical Treatment Options For Fecal IncontinenceSINAN SHAWKATNo ratings yet
- Biliary InjuryDocument9 pagesBiliary InjurySINAN SHAWKATNo ratings yet
- Punção No Hipocôndrio Esquerdo Com Agulha de Veress para A Criação Do PneumoperitônioDocument8 pagesPunção No Hipocôndrio Esquerdo Com Agulha de Veress para A Criação Do PneumoperitônioSINAN SHAWKATNo ratings yet
- Hemosuccus Pancreaticus: A Mysterious Cause of Gastrointestinal BleedingDocument6 pagesHemosuccus Pancreaticus: A Mysterious Cause of Gastrointestinal BleedingSINAN SHAWKATNo ratings yet
- Complete Urine Examination (CUE), Urine: MR.P V Rama RaoDocument19 pagesComplete Urine Examination (CUE), Urine: MR.P V Rama RaoGautam PendyalaNo ratings yet
- LOGIQ S8 XDC BrochureDocument5 pagesLOGIQ S8 XDC BrochureDANIA BWIDANINo ratings yet
- Lab Test 22Document139 pagesLab Test 22Noor MajaliNo ratings yet
- Biology Investigatory Project: Sleeping Habits and DisordersDocument23 pagesBiology Investigatory Project: Sleeping Habits and Disordersred snapper0% (1)
- ICD 10 CM SPECIALIZED CodingWorkbookwithAns v1.1Document161 pagesICD 10 CM SPECIALIZED CodingWorkbookwithAns v1.1AntonSusanto100% (2)
- NIMAS Medical FormDocument2 pagesNIMAS Medical FormBhargav VekariaNo ratings yet
- A Case Study On Dengue FeverDocument10 pagesA Case Study On Dengue FeverRinrin de BelenNo ratings yet
- Data Obat Perlu CekDocument57 pagesData Obat Perlu CekIvo NilaNo ratings yet
- Test Taking Strategies For The NCLEXDocument6 pagesTest Taking Strategies For The NCLEXRomel CunetaNo ratings yet
- To Be Completed by The AssesseeDocument20 pagesTo Be Completed by The AssesseeJitu TradersNo ratings yet
- Effect of Gabapentin Vs Pregabalin On Pain Intensity in Adults WIth Chronic Sciatica A Randomized Clinical TrialDocument7 pagesEffect of Gabapentin Vs Pregabalin On Pain Intensity in Adults WIth Chronic Sciatica A Randomized Clinical TrialJorge Dornellys LapaNo ratings yet
- Icu Procedures and TechniquesDocument106 pagesIcu Procedures and TechniquesAnusha VergheseNo ratings yet
- RDS HvacDocument1 pageRDS HvacQNBNo ratings yet
- MSM Information BookletDocument36 pagesMSM Information Bookletzimko100% (3)
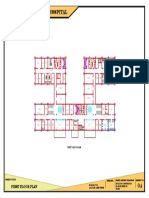
- 100 Bedded General Hospital: First Floor PlanDocument1 page100 Bedded General Hospital: First Floor PlanAshish chauhanNo ratings yet
- Patient Assessment ToolDocument2 pagesPatient Assessment ToolRachael93% (41)
- S59 - LPL - Tilak Nagar 4B/13, Near Metro Pillar No.494, Tilak N AGAR, NEW DELHI - 110018 DelhiDocument4 pagesS59 - LPL - Tilak Nagar 4B/13, Near Metro Pillar No.494, Tilak N AGAR, NEW DELHI - 110018 DelhiAyushNo ratings yet
- List of Panel HospitalsDocument38 pagesList of Panel HospitalsSaurav BansalNo ratings yet
- Year 3 Undergraduate Progressive Test - Attempt reviewPDF - 231031 - 194511Document49 pagesYear 3 Undergraduate Progressive Test - Attempt reviewPDF - 231031 - 194511DR BUYINZA TITUSNo ratings yet
- Jadwal Kuliah Blok Ss FK Umi 2016 Fix 22 SeptDocument16 pagesJadwal Kuliah Blok Ss FK Umi 2016 Fix 22 SeptAdjhy Aji AchmadNo ratings yet
- Adult Hip (2nd Edition)Document1,693 pagesAdult Hip (2nd Edition)Jocelyne SturridgeNo ratings yet
- Apotek Mega Medika: Kode Item Nama Item Jenis Rak Stok Harga Pokok SatuanDocument24 pagesApotek Mega Medika: Kode Item Nama Item Jenis Rak Stok Harga Pokok Satuanyuyun arlitaNo ratings yet
- Some Misconceptions and Pitfalls in UltrasonographyDocument27 pagesSome Misconceptions and Pitfalls in UltrasonographyMădălina CiobotariuNo ratings yet
- Prinsip Kedokteran Keluarga 2018Document57 pagesPrinsip Kedokteran Keluarga 2018BisukNo ratings yet
- Clinical Practice Guideline - Ménière's Disease PDFDocument56 pagesClinical Practice Guideline - Ménière's Disease PDFCarol Natalia Fonseca SalgadoNo ratings yet
- Book IndentDocument6 pagesBook Indentpushpajachar95No ratings yet
- Revise Nursing Care PlanDocument5 pagesRevise Nursing Care PlanNur SetsuNo ratings yet
- Week 13 Documentation Related To Client CareDocument87 pagesWeek 13 Documentation Related To Client Care8rvgjxf92kNo ratings yet
- Mesenchymal Stromal Cells: Potential For Cardiovascular RepairDocument19 pagesMesenchymal Stromal Cells: Potential For Cardiovascular RepairardhanputraNo ratings yet





























































































Download as pdf or txt
You might also like
- Atlas of Surgical Techniques in TraumaDocument364 pagesAtlas of Surgical Techniques in TraumaAgustina Zabini100% (1)
- Iatrogenic Biliary InjuriesDocument15 pagesIatrogenic Biliary InjuriessolysanNo ratings yet
- Trauma ColonDocument7 pagesTrauma Colonricardo arreguiNo ratings yet
- Tto de Ileo BiliarDocument5 pagesTto de Ileo BiliarnerisNo ratings yet
- WJG 20 13904Document8 pagesWJG 20 13904iovanela campoNo ratings yet
- 1 s2.0 S1091255X23056731 MainDocument8 pages1 s2.0 S1091255X23056731 MainPaul SantiagoNo ratings yet
- Multilevel Duodenal Injury After Blunt TraumaDocument5 pagesMultilevel Duodenal Injury After Blunt TraumaHanny RusliNo ratings yet
- Iatrogenic Hepatopancreaticobiliary Injuries: A ReviewDocument13 pagesIatrogenic Hepatopancreaticobiliary Injuries: A ReviewJohn ShipNo ratings yet
- 6 Readmission With Major AbdominalDocument10 pages6 Readmission With Major AbdominalElizabeth Mautino CaceresNo ratings yet
- Post-Cholecystectomy Acute Injury: What Can Go Wrong?Document7 pagesPost-Cholecystectomy Acute Injury: What Can Go Wrong?Ramyasree BadeNo ratings yet
- Iatrogenic Biliary Injuries: Classification, Identification, and ManagementDocument15 pagesIatrogenic Biliary Injuries: Classification, Identification, and ManagementLUISNo ratings yet
- Minimally Invasive EsophagectomyDocument5 pagesMinimally Invasive Esophagectomyfernando herbellaNo ratings yet
- Corrosive InjuryDocument6 pagesCorrosive InjuryCristian O. Saavedra RodriguezNo ratings yet
- SurgeryDocument7 pagesSurgeryFrancisco GilNo ratings yet
- International Consensus Conference On Open Abdomen in TraumaDocument11 pagesInternational Consensus Conference On Open Abdomen in TraumaCarlos HernándezNo ratings yet
- 1 s2.0 S174391910700129X MainDocument6 pages1 s2.0 S174391910700129X MainGiorgio André Gabino GonzalezNo ratings yet
- Management of Duodenal Trauma: ReviewDocument4 pagesManagement of Duodenal Trauma: ReviewAladesuruOlumideAdewaleNo ratings yet
- Pancreatitis Aguda Necrotizante Papel de La Cirugía 2017 FranciaDocument8 pagesPancreatitis Aguda Necrotizante Papel de La Cirugía 2017 FranciasergiocansecoguerraNo ratings yet
- 268 2018 Article 4642Document9 pages268 2018 Article 4642Derian TanwijayaNo ratings yet
- Post-Operative Biliary StricturesDocument7 pagesPost-Operative Biliary StricturesGeraldNo ratings yet
- 01 Editorial 6042 IngDocument2 pages01 Editorial 6042 IngJuan Mendia OssioNo ratings yet
- Baldoni 2011Document10 pagesBaldoni 2011naili nsnNo ratings yet
- Via BiliarDocument7 pagesVia Biliarahs ahnNo ratings yet
- 8 9 FistulasDocument9 pages8 9 FistulascystanarisaNo ratings yet
- Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite: DOI: 10.1590/S0100-69912014000300016Document4 pagesTbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite: DOI: 10.1590/S0100-69912014000300016Hanny RusliNo ratings yet
- Management of Duodenal Trauma: Chinese Journal of Traumatology (English Edition) February 2011Document5 pagesManagement of Duodenal Trauma: Chinese Journal of Traumatology (English Edition) February 2011dr muddssar sattarNo ratings yet
- Abdomen TraumaDocument74 pagesAbdomen TraumajeevanNo ratings yet
- Complications of Enterocystoplastycase SeriesDocument5 pagesComplications of Enterocystoplastycase SeriesIJAR JOURNALNo ratings yet
- B - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Document16 pagesB - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Battousaih1No ratings yet
- Chevallay 2020Document17 pagesChevallay 2020Maria PalNo ratings yet
- Pathophysiology and Prevention of Postoperative Peritoneal AdhesionsDocument9 pagesPathophysiology and Prevention of Postoperative Peritoneal AdhesionsFarah UlyaNo ratings yet
- Safe CholecystectomyDocument60 pagesSafe CholecystectomyCarlos Reyes100% (1)
- Penetratng InjuryDocument5 pagesPenetratng InjuryAbdulloh AbdurrohmanNo ratings yet
- Challenges in The Maagement of Pancreatic and Duodenal InjuriesDocument6 pagesChallenges in The Maagement of Pancreatic and Duodenal InjuriesOpl OplNo ratings yet
- Amilaze PredictivDocument7 pagesAmilaze PredictivDumitru RadulescuNo ratings yet
- Repair of Common Bile Duct InjuriesDocument12 pagesRepair of Common Bile Duct InjuriesDragoș PopaNo ratings yet
- Outcome of Surgical Treatment of Intestinal Perforation in Typhoid FeverDocument5 pagesOutcome of Surgical Treatment of Intestinal Perforation in Typhoid Feverdaru_qthinkNo ratings yet
- Repair of Common Bile Duct Injuries - UpToDateDocument16 pagesRepair of Common Bile Duct Injuries - UpToDateLuis Miguel Díaz VegaNo ratings yet
- Wong 2019Document11 pagesWong 2019karencuervomNo ratings yet
- A1504050119 PDFDocument19 pagesA1504050119 PDFImam Hakim SuryonoNo ratings yet
- Classification of Iatrogenic Bile Duct Injury - 2Document5 pagesClassification of Iatrogenic Bile Duct Injury - 2RameshKumarNo ratings yet
- Evaluation and Management of Splenic Injury in Blunt Abdominal TraumaDocument32 pagesEvaluation and Management of Splenic Injury in Blunt Abdominal TraumaImam Hakim SuryonoNo ratings yet
- 2012 Article 625 PDFDocument5 pages2012 Article 625 PDFPutri AdimuktiNo ratings yet
- 3Document8 pages3polomska.kmNo ratings yet
- 01 HepatogastroDocument3 pages01 Hepatogastroyacine26No ratings yet
- Acute CholangitisDocument11 pagesAcute CholangitisFrancisco EsparzaNo ratings yet
- Complicationsafter Pancreaticoduodenectomy: Robert SimonDocument10 pagesComplicationsafter Pancreaticoduodenectomy: Robert SimonŞükriye AngaNo ratings yet
- Injury Patterns and Causes of Death in 953 Patients With Penetrating Abdominal War Wounds in A Civilian Independent Non-Governmental Organization Hospital in Lashkargah, AfghanistanDocument8 pagesInjury Patterns and Causes of Death in 953 Patients With Penetrating Abdominal War Wounds in A Civilian Independent Non-Governmental Organization Hospital in Lashkargah, AfghanistanLeandro NogueiraNo ratings yet
- An Unusual Cause of Failure of Nom in Liver Trauma FinalDocument20 pagesAn Unusual Cause of Failure of Nom in Liver Trauma FinalMariyam AlblooshiNo ratings yet
- Endoscopic and Surgical Management of Iatrogenic BDocument10 pagesEndoscopic and Surgical Management of Iatrogenic BRahul SinghNo ratings yet
- Laparoscopic Cholecystectomy:An Experience of 200 Cases: Original ArticleDocument4 pagesLaparoscopic Cholecystectomy:An Experience of 200 Cases: Original ArticleAndrei GheorghitaNo ratings yet
- Jurnal Case ReportDocument3 pagesJurnal Case ReportNining Rhyanie TampubolonNo ratings yet
- Management of CBD Injury - Digestive Week Jogja 2016Document42 pagesManagement of CBD Injury - Digestive Week Jogja 2016Wisnu DipoyonoNo ratings yet
- 2015 Laparoscopic Surgery in Abdominal Trauma A Single Center Review of A 7-Year ExperienceDocument7 pages2015 Laparoscopic Surgery in Abdominal Trauma A Single Center Review of A 7-Year ExperiencejohnnhekoNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument5 pagesAnnals of Medicine and Surgery: SciencedirectMishel Rodriguez GuzmanNo ratings yet
- 1 s2.0 S0065341116000038 MainDocument12 pages1 s2.0 S0065341116000038 MainFlorin AchimNo ratings yet
- Subtotal Gastrectomy For Gastric CancerDocument15 pagesSubtotal Gastrectomy For Gastric CancerRUBEN DARIO AGRESOTTNo ratings yet
- Bile Duct InjuriesDocument24 pagesBile Duct InjuriesLUISNo ratings yet
- International Journal of Surgery Case ReportsDocument5 pagesInternational Journal of Surgery Case ReportsMuhammad Fuad MahfudNo ratings yet
- Wound: Abdominal DehiscenceDocument5 pagesWound: Abdominal DehiscencesmileyginaaNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- Surgical Treatment Options For Fecal IncontinenceDocument7 pagesSurgical Treatment Options For Fecal IncontinenceSINAN SHAWKATNo ratings yet
- Biliary InjuryDocument9 pagesBiliary InjurySINAN SHAWKATNo ratings yet
- Punção No Hipocôndrio Esquerdo Com Agulha de Veress para A Criação Do PneumoperitônioDocument8 pagesPunção No Hipocôndrio Esquerdo Com Agulha de Veress para A Criação Do PneumoperitônioSINAN SHAWKATNo ratings yet
- Hemosuccus Pancreaticus: A Mysterious Cause of Gastrointestinal BleedingDocument6 pagesHemosuccus Pancreaticus: A Mysterious Cause of Gastrointestinal BleedingSINAN SHAWKATNo ratings yet
- Complete Urine Examination (CUE), Urine: MR.P V Rama RaoDocument19 pagesComplete Urine Examination (CUE), Urine: MR.P V Rama RaoGautam PendyalaNo ratings yet
- LOGIQ S8 XDC BrochureDocument5 pagesLOGIQ S8 XDC BrochureDANIA BWIDANINo ratings yet
- Lab Test 22Document139 pagesLab Test 22Noor MajaliNo ratings yet
- Biology Investigatory Project: Sleeping Habits and DisordersDocument23 pagesBiology Investigatory Project: Sleeping Habits and Disordersred snapper0% (1)
- ICD 10 CM SPECIALIZED CodingWorkbookwithAns v1.1Document161 pagesICD 10 CM SPECIALIZED CodingWorkbookwithAns v1.1AntonSusanto100% (2)
- NIMAS Medical FormDocument2 pagesNIMAS Medical FormBhargav VekariaNo ratings yet
- A Case Study On Dengue FeverDocument10 pagesA Case Study On Dengue FeverRinrin de BelenNo ratings yet
- Data Obat Perlu CekDocument57 pagesData Obat Perlu CekIvo NilaNo ratings yet
- Test Taking Strategies For The NCLEXDocument6 pagesTest Taking Strategies For The NCLEXRomel CunetaNo ratings yet
- To Be Completed by The AssesseeDocument20 pagesTo Be Completed by The AssesseeJitu TradersNo ratings yet
- Effect of Gabapentin Vs Pregabalin On Pain Intensity in Adults WIth Chronic Sciatica A Randomized Clinical TrialDocument7 pagesEffect of Gabapentin Vs Pregabalin On Pain Intensity in Adults WIth Chronic Sciatica A Randomized Clinical TrialJorge Dornellys LapaNo ratings yet
- Icu Procedures and TechniquesDocument106 pagesIcu Procedures and TechniquesAnusha VergheseNo ratings yet
- RDS HvacDocument1 pageRDS HvacQNBNo ratings yet
- MSM Information BookletDocument36 pagesMSM Information Bookletzimko100% (3)
- 100 Bedded General Hospital: First Floor PlanDocument1 page100 Bedded General Hospital: First Floor PlanAshish chauhanNo ratings yet
- Patient Assessment ToolDocument2 pagesPatient Assessment ToolRachael93% (41)
- S59 - LPL - Tilak Nagar 4B/13, Near Metro Pillar No.494, Tilak N AGAR, NEW DELHI - 110018 DelhiDocument4 pagesS59 - LPL - Tilak Nagar 4B/13, Near Metro Pillar No.494, Tilak N AGAR, NEW DELHI - 110018 DelhiAyushNo ratings yet
- List of Panel HospitalsDocument38 pagesList of Panel HospitalsSaurav BansalNo ratings yet
- Year 3 Undergraduate Progressive Test - Attempt reviewPDF - 231031 - 194511Document49 pagesYear 3 Undergraduate Progressive Test - Attempt reviewPDF - 231031 - 194511DR BUYINZA TITUSNo ratings yet
- Jadwal Kuliah Blok Ss FK Umi 2016 Fix 22 SeptDocument16 pagesJadwal Kuliah Blok Ss FK Umi 2016 Fix 22 SeptAdjhy Aji AchmadNo ratings yet
- Adult Hip (2nd Edition)Document1,693 pagesAdult Hip (2nd Edition)Jocelyne SturridgeNo ratings yet
- Apotek Mega Medika: Kode Item Nama Item Jenis Rak Stok Harga Pokok SatuanDocument24 pagesApotek Mega Medika: Kode Item Nama Item Jenis Rak Stok Harga Pokok Satuanyuyun arlitaNo ratings yet
- Some Misconceptions and Pitfalls in UltrasonographyDocument27 pagesSome Misconceptions and Pitfalls in UltrasonographyMădălina CiobotariuNo ratings yet
- Prinsip Kedokteran Keluarga 2018Document57 pagesPrinsip Kedokteran Keluarga 2018BisukNo ratings yet
- Clinical Practice Guideline - Ménière's Disease PDFDocument56 pagesClinical Practice Guideline - Ménière's Disease PDFCarol Natalia Fonseca SalgadoNo ratings yet
- Book IndentDocument6 pagesBook Indentpushpajachar95No ratings yet
- Revise Nursing Care PlanDocument5 pagesRevise Nursing Care PlanNur SetsuNo ratings yet
- Week 13 Documentation Related To Client CareDocument87 pagesWeek 13 Documentation Related To Client Care8rvgjxf92kNo ratings yet
- Mesenchymal Stromal Cells: Potential For Cardiovascular RepairDocument19 pagesMesenchymal Stromal Cells: Potential For Cardiovascular RepairardhanputraNo ratings yet