Download as pdf or txt
You might also like
- Chapter 19 Mental StatusDocument3 pagesChapter 19 Mental StatusAmber Nicole HubbardNo ratings yet
- 0671Document5 pages0671prashanthNo ratings yet
- Mother ArticleDocument6 pagesMother ArticleRakesh JhaNo ratings yet
- TRUP Syndrome in Elderly Patients A Retrospective Observational StudyDocument6 pagesTRUP Syndrome in Elderly Patients A Retrospective Observational StudyanibalmezagarcesNo ratings yet
- Diagnostic Value of Combined Static-Excretory MR Urography in Children With HydronephrosisDocument9 pagesDiagnostic Value of Combined Static-Excretory MR Urography in Children With HydronephrosisnyimasNo ratings yet
- Diagnostic Value of Combined Static Excretory MR Urogr - 2015 - Journal of AdvanDocument9 pagesDiagnostic Value of Combined Static Excretory MR Urogr - 2015 - Journal of AdvanSuresh SeerviNo ratings yet
- Comparison of Surgical Outcome and Complications Between Spinal and General Anaesthesia For Patients Undergoing Percutaneous NephrolithotomyDocument5 pagesComparison of Surgical Outcome and Complications Between Spinal and General Anaesthesia For Patients Undergoing Percutaneous Nephrolithotomynaufal12345No ratings yet
- Blana 2004Document4 pagesBlana 2004skribekbenjaminNo ratings yet
- D ASOf-nask 1Document7 pagesD ASOf-nask 1Academecian groupNo ratings yet
- ST Riner Sistem Ta Lar Nda ESWL Nin Etkinli I (#390504) - 419548Document6 pagesST Riner Sistem Ta Lar Nda ESWL Nin Etkinli I (#390504) - 419548Abeselom lemmaNo ratings yet
- Articulo N. 1 ProstataDocument5 pagesArticulo N. 1 ProstataNathaly RamírezNo ratings yet
- Burud 2020Document8 pagesBurud 2020Wirda Elya SariNo ratings yet
- Vur KoreanDocument7 pagesVur KoreanIoannis ValioulisNo ratings yet
- Clinical Study: Retrograde Intrarenal Surgery Versus Percutaneous Lithotripsy To Treat Renal Stones 2-3 CM in DiameterDocument5 pagesClinical Study: Retrograde Intrarenal Surgery Versus Percutaneous Lithotripsy To Treat Renal Stones 2-3 CM in DiameterAslesa Wangpathi PagehgiriNo ratings yet
- Role of Triple Phase Computed Tomography Findings For Evaluation of Hepatic LesionsDocument8 pagesRole of Triple Phase Computed Tomography Findings For Evaluation of Hepatic LesionsGordana PuzovicNo ratings yet
- Role of Sexual Intercourse After Shockwave Lithotripsy For Distal Ureteral Stones: A Randomized Controlled TrialDocument5 pagesRole of Sexual Intercourse After Shockwave Lithotripsy For Distal Ureteral Stones: A Randomized Controlled TrialAnindya Laksmi LarasatiNo ratings yet
- Zhou 2013Document7 pagesZhou 2013Leonardo SamuelNo ratings yet
- Comparative Evaluation of Ultrasonography and Computed Tomography in Pancreatic LesionsDocument13 pagesComparative Evaluation of Ultrasonography and Computed Tomography in Pancreatic LesionsMultan SohanhalwaNo ratings yet
- Bipolar Versus Monopolar Resection of Benign Prostate Hyperplasia: A Comparison of Plasma Electrolytes, Hemoglobin and TUR SyndromeDocument7 pagesBipolar Versus Monopolar Resection of Benign Prostate Hyperplasia: A Comparison of Plasma Electrolytes, Hemoglobin and TUR Syndromefabian arassiNo ratings yet
- Obstructive Uropathy With Renal FailureDocument3 pagesObstructive Uropathy With Renal FailureAnggaNo ratings yet
- Indications of Ventriculoperitoneal Shunt: A Prospective StudyDocument8 pagesIndications of Ventriculoperitoneal Shunt: A Prospective Studyvalencia suwardiNo ratings yet
- Posterior Tibial Nerve Stimulation As Treatment For The Overactive BladderDocument5 pagesPosterior Tibial Nerve Stimulation As Treatment For The Overactive BladderSendyA-AzizNo ratings yet
- Hepatic Incidentaloma: The Rule of Tens: Original ArticleDocument5 pagesHepatic Incidentaloma: The Rule of Tens: Original ArticleNora Vianey Alcantara VelascoNo ratings yet
- Chung 2004Document4 pagesChung 2004raghad.bassalNo ratings yet
- Comparative Study of Lithotripsy and Miniperc in 11 To 18 MM Impacted Puj CalculiDocument5 pagesComparative Study of Lithotripsy and Miniperc in 11 To 18 MM Impacted Puj CalculiInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- Journal 5Document4 pagesJournal 517.061 Kharismayanti FatimatuzzahroNo ratings yet
- Izumita 2020Document5 pagesIzumita 2020AsimaJulianaSiregarNo ratings yet
- Efficacy and Safety of Sacral Nerve Stimulation For Urinary Urge Incontinence - A Systematic ReviewDocument7 pagesEfficacy and Safety of Sacral Nerve Stimulation For Urinary Urge Incontinence - A Systematic ReviewMUHAMMMAD FAKHRINo ratings yet
- HN 03-2011 Submadibular Salivary Gland Transfer PDFDocument7 pagesHN 03-2011 Submadibular Salivary Gland Transfer PDFVikas VatsNo ratings yet
- TSWJ2012 731089Document9 pagesTSWJ2012 731089samamansorNo ratings yet
- Intravenous UROGRAMDocument14 pagesIntravenous UROGRAMvijendrakumarsahuNo ratings yet
- 114-Article Text-170-1-10-20180209Document6 pages114-Article Text-170-1-10-20180209Munazzah MehakNo ratings yet
- SC 2015242Document7 pagesSC 2015242resi ciruNo ratings yet
- Investigations in UrologyDocument19 pagesInvestigations in UrologyMohammed AadeelNo ratings yet
- Ahs V19i3 57Document6 pagesAhs V19i3 57Priska ForceveeanaNo ratings yet
- The Comparative Study of Usg and MDCT in The Evaluation of Pelvic Masses in FemalesDocument10 pagesThe Comparative Study of Usg and MDCT in The Evaluation of Pelvic Masses in FemalesIJAR JOURNALNo ratings yet
- Usg Acute AppendicitisDocument10 pagesUsg Acute AppendicitisAtika RahmahNo ratings yet
- Liu Et Al 2015 Comparison of Multislice Computed Tomography and Clinical Scores For Diagnosing Acute AppendicitisDocument9 pagesLiu Et Al 2015 Comparison of Multislice Computed Tomography and Clinical Scores For Diagnosing Acute AppendicitisNovi OktaviantiNo ratings yet
- Comparison of Percutaneous Nephrolithotomy and Retrograde Intrarenal Surgery in Treating 20-40 MM Renal StonesDocument5 pagesComparison of Percutaneous Nephrolithotomy and Retrograde Intrarenal Surgery in Treating 20-40 MM Renal StonesputraNo ratings yet
- Safety and Efficacy of Ultrasound-Guided Fiducial Marker Implantation For Cyberknife Radiation TherapyDocument7 pagesSafety and Efficacy of Ultrasound-Guided Fiducial Marker Implantation For Cyberknife Radiation TherapyAngelito SalinasNo ratings yet
- US Not Useful For Low BMI and Easy Palpable PatientsDocument6 pagesUS Not Useful For Low BMI and Easy Palpable Patientscailin.hicuraNo ratings yet
- MR Sialography and Conventional Sialography in SalDocument6 pagesMR Sialography and Conventional Sialography in Salshehla khanNo ratings yet
- MainDocument7 pagesMainEngga CandranataNo ratings yet
- The Nephrologist As An Ultrasonographer: Adv Chronic Kidney Dis. 2020 27 (3) :243-252Document10 pagesThe Nephrologist As An Ultrasonographer: Adv Chronic Kidney Dis. 2020 27 (3) :243-252Kev Jose Ruiz RojasNo ratings yet
- Role of Percutaneous Ultrasonographic Guided Radiofrequency Ablation in The Management of Hepatocellular CarcinomaDocument8 pagesRole of Percutaneous Ultrasonographic Guided Radiofrequency Ablation in The Management of Hepatocellular CarcinomadickyaririsandyNo ratings yet
- Ultrasonography of Immature Teratomas: 11 Case Reports: Z.Y. Shen, B. Hu, G.L. Xia, K. ShenDocument8 pagesUltrasonography of Immature Teratomas: 11 Case Reports: Z.Y. Shen, B. Hu, G.L. Xia, K. ShenIlincaNo ratings yet
- BPJ Vol 14 No 2 P 921-938Document18 pagesBPJ Vol 14 No 2 P 921-938Satish SinghNo ratings yet
- Pemeriksaan IVPDocument41 pagesPemeriksaan IVPChandra Noor SatriyoNo ratings yet
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDocument5 pagesSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariNo ratings yet
- Un Estudio Retrospectivo de Pacientes post-TURP Que Se Sometieron A Anestesia Espinal Con Consideración de Los Déficits Neurológicos InvolucradosDocument1 pageUn Estudio Retrospectivo de Pacientes post-TURP Que Se Sometieron A Anestesia Espinal Con Consideración de Los Déficits Neurológicos InvolucradosanibalmezagarcesNo ratings yet
- Transrectal Ultrasound and Biopsy in The Early Diagnosis of Prostate CancerDocument10 pagesTransrectal Ultrasound and Biopsy in The Early Diagnosis of Prostate CancerHutri MahardikaNo ratings yet
- Computerized Tomography (CT) Scan: Indication Abnormal ResultsDocument7 pagesComputerized Tomography (CT) Scan: Indication Abnormal ResultsVanessa VillanuevaNo ratings yet
- Interest of Trans-Obturator Tape (Tot) in Stress Urinary Incontinence :series of 173 Women and 1 ManDocument5 pagesInterest of Trans-Obturator Tape (Tot) in Stress Urinary Incontinence :series of 173 Women and 1 ManIJAR JOURNALNo ratings yet
- Liver Fibrosis With Two-Dimensional US Shear-Wave Elastography in Participants With Chronic Hepatitis B A Prospective Multicenter StudyDocument9 pagesLiver Fibrosis With Two-Dimensional US Shear-Wave Elastography in Participants With Chronic Hepatitis B A Prospective Multicenter StudynanNo ratings yet
- Radiation Doses From Small-Bowel Follow-Through and Abdominopelvic MDCT in Crohn's DiseaseDocument16 pagesRadiation Doses From Small-Bowel Follow-Through and Abdominopelvic MDCT in Crohn's DiseaseAbdullahNo ratings yet
- Monopolar Enucleation Vs Transurethral Resection of The ProstateDocument7 pagesMonopolar Enucleation Vs Transurethral Resection of The ProstateAbraham WilliamNo ratings yet
- An Observation Trial Without Surgical Treatment in Patients With Papillary Microcarcinoma of The ThyroidDocument7 pagesAn Observation Trial Without Surgical Treatment in Patients With Papillary Microcarcinoma of The Thyroiddavid villamilNo ratings yet
- Posterior Sagittal Anorectoplasty in Anorectal MalformationsDocument5 pagesPosterior Sagittal Anorectoplasty in Anorectal MalformationsmustikaarumNo ratings yet
- Blunt Abdominal Trauma: The Role of Focused Abdominal Sonography in Assessment of Organ Injury and Reducing The Need For CTDocument7 pagesBlunt Abdominal Trauma: The Role of Focused Abdominal Sonography in Assessment of Organ Injury and Reducing The Need For CTsiska khairNo ratings yet
- 5-Renal Cortical Thickness in Adults WithDocument4 pages5-Renal Cortical Thickness in Adults Withjeb faqNo ratings yet
- Contrast-Enhanced Ultrasound Imaging of Hepatic NeoplasmsFrom EverandContrast-Enhanced Ultrasound Imaging of Hepatic NeoplasmsWen-Ping WangNo ratings yet
- Izumita 2020Document5 pagesIzumita 2020AsimaJulianaSiregarNo ratings yet
- Cardiovascular TSDocument22 pagesCardiovascular TSAsimaJulianaSiregarNo ratings yet
- Bone Fragility in TSDocument8 pagesBone Fragility in TSAsimaJulianaSiregarNo ratings yet
- The Cancer HandbookDocument1,529 pagesThe Cancer HandbookAsimaJulianaSiregarNo ratings yet
- Study Design in The ATBC StudyDocument6 pagesStudy Design in The ATBC StudyAsimaJulianaSiregarNo ratings yet
- Stubble BurningDocument12 pagesStubble BurningSherin MaryNo ratings yet
- Cmca Lec ReviewerDocument32 pagesCmca Lec Reviewercuteathena11No ratings yet
- Chapter 63 Antifungal Susceptibility Testing-Therapy & PreventionDocument13 pagesChapter 63 Antifungal Susceptibility Testing-Therapy & PreventionbartsnewNo ratings yet
- Exjade: (Deferasirox)Document13 pagesExjade: (Deferasirox)athayafebNo ratings yet
- Notes 20211016211852Document2 pagesNotes 20211016211852fghhdd4rtgj75423No ratings yet
- Dealing With PatientDocument14 pagesDealing With PatientAnggih PriyantoNo ratings yet
- Artikel Review Ratna DpsDocument5 pagesArtikel Review Ratna DpsRika AmeliaNo ratings yet
- Fixed ProsthodonticsDocument21 pagesFixed ProsthodonticsnseraldenNo ratings yet
- Cover Letter - Wellington ManagementDocument1 pageCover Letter - Wellington ManagementAnas HadiNo ratings yet
- Laurie Ritchie, Blueprint For Learning: Constructing College Couirse To Facilitate, Assess and Document Learning Sterling VA: Stylus, 2006Document4 pagesLaurie Ritchie, Blueprint For Learning: Constructing College Couirse To Facilitate, Assess and Document Learning Sterling VA: Stylus, 2006Joel Lim Zamora0% (1)
- Myhealth Suraksha - PWWDocument38 pagesMyhealth Suraksha - PWWpriyankaNo ratings yet
- Esmeril de Banco Metabo DS-200Document24 pagesEsmeril de Banco Metabo DS-200rctallerelectricoNo ratings yet
- Vaksin Influenza OverviewDocument27 pagesVaksin Influenza OverviewMaria Astika DewiNo ratings yet
- Ethico Legal of Perioperative NursingDocument19 pagesEthico Legal of Perioperative NursingAziil Liiza100% (1)
- The Answer Task 6 Toefl PreparationDocument7 pagesThe Answer Task 6 Toefl PreparationEmilia AnnisaNo ratings yet
- Tutorials 20156Document6 pagesTutorials 20156Everton KingNo ratings yet
- 1009 1014 1 PDFDocument6 pages1009 1014 1 PDFCuriosityShopNo ratings yet
- CA - (June'16 - May'17)Document276 pagesCA - (June'16 - May'17)S.VigneshwaranNo ratings yet
- Bronchopneumonia Care PlanDocument6 pagesBronchopneumonia Care PlanAbhijit Soundade0% (1)
- Colorado House Bill 13-1114Document20 pagesColorado House Bill 13-1114Medicinal ColoradoNo ratings yet
- MSCT SCAN ABDOMEN PDSRI DR IraDocument78 pagesMSCT SCAN ABDOMEN PDSRI DR IraGuntur SaputraNo ratings yet
- G Hid Montes Sory Pentru Bebelus IDocument42 pagesG Hid Montes Sory Pentru Bebelus Imelimatyas100% (1)
- School Health and Nutrition Program - IloiloDocument7 pagesSchool Health and Nutrition Program - IloiloJohn ArañoNo ratings yet
- Research Paper On Dengue Fever in PakistanDocument6 pagesResearch Paper On Dengue Fever in Pakistangvzz4v44100% (1)
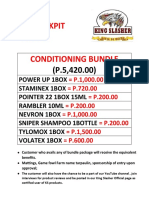
- Texas Cockpit Arena Conditioning BundleDocument4 pagesTexas Cockpit Arena Conditioning BundleHanna Sobreviñas AmanteNo ratings yet
- Pradhan Mantri Ujwala Yojna: Points To NoteDocument2 pagesPradhan Mantri Ujwala Yojna: Points To NotekrithikNo ratings yet
- A Guide To Well-BeingDocument111 pagesA Guide To Well-BeingAtul Pant100% (2)
- Dalena VDocument3 pagesDalena Vapi-346115077No ratings yet
- Hospital Information SystemDocument153 pagesHospital Information SystemKartik DwivediNo ratings yet