Download as pdf or txt
You might also like
- Cambridge Research ProposalDocument3 pagesCambridge Research ProposalRocky Balbowa100% (1)
- Stuxnet and Its Hidden Lessons On The Ethics of CyberweaponsDocument9 pagesStuxnet and Its Hidden Lessons On The Ethics of CyberweaponsprofcameloNo ratings yet
- Fluids and Electrolytes Reaction PaperDocument1 pageFluids and Electrolytes Reaction PaperKY LANo ratings yet
- Degenerative Disc Disease Concept MapDocument1 pageDegenerative Disc Disease Concept Mapnursing concept mapsNo ratings yet
- Anatomy and PhysiologyDocument2 pagesAnatomy and PhysiologyJeffrey Calicdan BucalaNo ratings yet
- Complement SystemDocument6 pagesComplement SystemJimit GandhiNo ratings yet
- Concept Map Meningitis TheoryDocument3 pagesConcept Map Meningitis TheoryMia AuliaNo ratings yet
- Mechanism of Labor: Presented By: GROUP 1Document11 pagesMechanism of Labor: Presented By: GROUP 1Mary Christine Estrada Cabactulan100% (1)
- NCP-Drug Study 2Document4 pagesNCP-Drug Study 2hsiriaNo ratings yet
- GI Bu FirastiDocument92 pagesGI Bu FirastiBriliant GhaustinNo ratings yet
- GENITO URINARY SYSTEM 2nd Year BSC NursingDocument8 pagesGENITO URINARY SYSTEM 2nd Year BSC NursingShreyas WalvekarNo ratings yet
- Biochemistry Week 3 - EnzymesDocument6 pagesBiochemistry Week 3 - EnzymesMicah JadeNo ratings yet
- Trixie - Anatomy and Physiology (Brain Tumor)Document4 pagesTrixie - Anatomy and Physiology (Brain Tumor)Trixie Marie Sabile AbdullaNo ratings yet
- Drug StudyDocument8 pagesDrug StudyJohn Ronald P. RamosNo ratings yet
- Bipolar Affective Disorder, Current Manic Episode With Symptoms of Psychotic and Care in NursingDocument4 pagesBipolar Affective Disorder, Current Manic Episode With Symptoms of Psychotic and Care in NursingKit LaraNo ratings yet
- Stages of Labor Nursing Intervention: First StageDocument3 pagesStages of Labor Nursing Intervention: First StageJhanniel IreneaNo ratings yet
- Cefoxitin and Ketorolac Edited!!Document3 pagesCefoxitin and Ketorolac Edited!!Bryan Cruz VisarraNo ratings yet
- Covid 19 - PathophysiologyDocument3 pagesCovid 19 - PathophysiologyRenea Joy ArruejoNo ratings yet
- Case Study 2Document4 pagesCase Study 2api-2451636590% (1)
- Breasts and AxillaeDocument10 pagesBreasts and Axillaedlneisha61100% (1)
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocument43 pagesPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaNo ratings yet
- Adrenocortical AgentsDocument14 pagesAdrenocortical AgentsFredie O HadjimudinNo ratings yet
- Gastrointestinal Tract 1Document14 pagesGastrointestinal Tract 1Jezzah Mae CañeteNo ratings yet
- Cerebral Palsy AnatomyDocument5 pagesCerebral Palsy AnatomyIoana irimiaNo ratings yet
- Anatomy and Physiology FinalDocument2 pagesAnatomy and Physiology FinalChloé Jane Hilario100% (1)
- GastrointestinalDocument39 pagesGastrointestinalالمسوول الاعلاميNo ratings yet
- NCP UreteroDocument1 pageNCP UreteroCerie Anne OlayNo ratings yet
- ParkinsonDocument2 pagesParkinsongoyaNo ratings yet
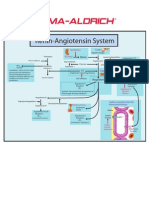
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Anatomy N Physiology of UtiDocument6 pagesAnatomy N Physiology of UtiMarjorie PalaganasNo ratings yet
- Hyperosmolar Hyperglycemic StateDocument10 pagesHyperosmolar Hyperglycemic StateMirko S. León RguezNo ratings yet
- Copy CNSDocument2 pagesCopy CNSJesica MarieNo ratings yet
- Stump CareDocument7 pagesStump CareirtazakazmiNo ratings yet
- Basilar Skull FractureDocument16 pagesBasilar Skull FractureRindahMDNo ratings yet
- Subjective Data: Baseline Data of Client.: Reference: Nurse's Pocket Guide: Diagnoses, Interventions, and RationalesDocument4 pagesSubjective Data: Baseline Data of Client.: Reference: Nurse's Pocket Guide: Diagnoses, Interventions, and RationalesJor GarciaNo ratings yet
- Child - Major Burn PDFDocument3 pagesChild - Major Burn PDFAldith GrahamNo ratings yet
- Pott Disease 1223292121651385 8Document54 pagesPott Disease 1223292121651385 8Ismail SalimNo ratings yet
- Geriatic Fluid and Electrolyte Imbalance NCPDocument4 pagesGeriatic Fluid and Electrolyte Imbalance NCPCA Candido JavierNo ratings yet
- Case Study HydrocephalusDocument19 pagesCase Study HydrocephalusJane Mae JesoroNo ratings yet
- Ineffective Airway ClearanceDocument1 pageIneffective Airway ClearanceChristineAlaNo ratings yet
- Urinary Incontinence and Retention Grup10Document13 pagesUrinary Incontinence and Retention Grup10Deniela Jamaicy HerbertNo ratings yet
- Anatomy and Physiology of OvaryDocument2 pagesAnatomy and Physiology of OvaryFrancez Anne GuanzonNo ratings yet
- Introduction CASE STUDYDocument3 pagesIntroduction CASE STUDYDavid CalaloNo ratings yet
- Coma - Types, Causes, Treatments, PrognosisDocument3 pagesComa - Types, Causes, Treatments, PrognosisgcsNo ratings yet
- Smooth MuscleDocument33 pagesSmooth MuscleDorin PathakNo ratings yet
- Physio Reviewer Renal To Acid BaseDocument11 pagesPhysio Reviewer Renal To Acid BaseNicole ChanNo ratings yet
- Trifluridine and TipiracilDocument3 pagesTrifluridine and TipiracilKristine AcasioNo ratings yet
- Sensory Organ-Sense of Smell - Nose, Taste-Tongue, Touch-Skin by DR - Reshma Ajay.Document46 pagesSensory Organ-Sense of Smell - Nose, Taste-Tongue, Touch-Skin by DR - Reshma Ajay.RESHMA AJAY100% (1)
- Papillary Thyroid Ca: Group. 1 B Grand CaseDocument16 pagesPapillary Thyroid Ca: Group. 1 B Grand CaseAdora Dela CruzNo ratings yet
- Anatomy and Physiology of The LungsDocument3 pagesAnatomy and Physiology of The LungsMayownski TejeroNo ratings yet
- Sleep Pattern DisturbanceDocument1 pageSleep Pattern DisturbanceNik Rose ElNo ratings yet
- Community Teaching Plan and Evaluation Submission, Assignment Week 6Document10 pagesCommunity Teaching Plan and Evaluation Submission, Assignment Week 6taniaNo ratings yet
- Case Study 2 NCPDocument1 pageCase Study 2 NCPJayson SamonteNo ratings yet
- Anatomy and PhysiologyDocument3 pagesAnatomy and PhysiologyLorraine Gambito100% (1)
- Nursing Care PlansDocument2 pagesNursing Care PlansatchiekNo ratings yet
- PancreatitisDocument6 pagesPancreatitisMahaNo ratings yet
- POLYMYOLITISDocument4 pagesPOLYMYOLITISAlexa Lexington Rae ZagadoNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Anatomy and PhysiologyDocument10 pagesAnatomy and Physiologykrizzia raymundoNo ratings yet
- Anaphy PancreasDocument6 pagesAnaphy PancreasAELYN SEVILLANo ratings yet
- Cells and Secretions of The Pancreatic IsletsDocument4 pagesCells and Secretions of The Pancreatic IsletsSophia OcayNo ratings yet
- Checklist On Administering Cleansing Enema: ProcedureDocument3 pagesChecklist On Administering Cleansing Enema: ProcedureKyla CalzadoNo ratings yet
- Philippine Mining Act of 1995Document11 pagesPhilippine Mining Act of 1995Kyla CalzadoNo ratings yet
- Report - NCM 114Document37 pagesReport - NCM 114Kyla CalzadoNo ratings yet
- NCP - Disturbed Sleep PatternDocument3 pagesNCP - Disturbed Sleep PatternKyla CalzadoNo ratings yet
- GEE 1 - Group PresentationDocument20 pagesGEE 1 - Group PresentationKyla CalzadoNo ratings yet
- Procedure Rationale RD 1 2 PEDocument7 pagesProcedure Rationale RD 1 2 PEKyla CalzadoNo ratings yet
- 07 Hawt and VawtDocument10 pages07 Hawt and Vawtthisisanonymous6254No ratings yet
- FIN2339-Ch4 - Practice QuestionsDocument3 pagesFIN2339-Ch4 - Practice QuestionsJasleen Gill100% (1)
- ANSI B30.8 InterpretationDocument10 pagesANSI B30.8 InterpretationAndreyNo ratings yet
- Sparsh Idt FinalDocument12 pagesSparsh Idt FinalSparsh vatsNo ratings yet
- Principal 5svbk8Document56 pagesPrincipal 5svbk8badillojdNo ratings yet
- UPI Linking SpecificationDocument42 pagesUPI Linking Specificationananya26196No ratings yet
- Img 0004Document7 pagesImg 0004velavan100% (1)
- Epe 2013111515302022Document5 pagesEpe 2013111515302022qais652002No ratings yet
- Fire Catalog Alco-LiteDocument14 pagesFire Catalog Alco-LiteForum PompieriiNo ratings yet
- Modeling & Simulation of Spherical Robot Configuration Using Solidworks & MatlabDocument3 pagesModeling & Simulation of Spherical Robot Configuration Using Solidworks & Matlabkarthi0% (1)
- Calculus III and IV - SodinDocument164 pagesCalculus III and IV - Sodintom-manor-1138No ratings yet
- DLL WK 10 LC 171819Document14 pagesDLL WK 10 LC 171819Regiel Guiang ArnibalNo ratings yet
- Jack Goldestone - THE PROBLEM OF THE EARLY MODERN WORLD - TEXT PDFDocument36 pagesJack Goldestone - THE PROBLEM OF THE EARLY MODERN WORLD - TEXT PDFBojanNo ratings yet
- 2july Grade 1 TestDocument12 pages2july Grade 1 TestEron Roi Centina-gacutanNo ratings yet
- Types of VolcanoesDocument10 pagesTypes of VolcanoesRobert MestiolaNo ratings yet
- Khidmat - The ServiceDocument6 pagesKhidmat - The ServiceAjay Prakash VermaNo ratings yet
- GA 132 VSD - 150 Psi - Air Cooled - 2015 Rev 0Document1 pageGA 132 VSD - 150 Psi - Air Cooled - 2015 Rev 0esteban muñozNo ratings yet
- Table of Specifications Grade 5Document3 pagesTable of Specifications Grade 5rene balayoNo ratings yet
- Design Basis For Nht/Unit 02: SnamprogettiDocument2 pagesDesign Basis For Nht/Unit 02: Snamprogettimohsen ranjbarNo ratings yet
- Ascensional and Descensional VentilationDocument5 pagesAscensional and Descensional VentilationP Taviti Naidu100% (1)
- Resource Guide For New ChrosDocument23 pagesResource Guide For New Chroslane.a.mcfNo ratings yet
- Evolution of The Entertainment Ecosystem in India and Challenges AheadDocument78 pagesEvolution of The Entertainment Ecosystem in India and Challenges AheadAbhishek KumarNo ratings yet
- ISBB CompilationDocument6 pagesISBB CompilationElla SalesNo ratings yet
- BGP (Border Gateway Protocol) - Port 179: Gateway Protocols (IGP's)Document32 pagesBGP (Border Gateway Protocol) - Port 179: Gateway Protocols (IGP's)Nitesh MulukNo ratings yet
- The Concept of Developmental PsychologyDocument16 pagesThe Concept of Developmental PsychologyJulie Anne ÜNo ratings yet
- Threshold Heteroskedastic Models: Jean-Michel ZakoianDocument25 pagesThreshold Heteroskedastic Models: Jean-Michel ZakoianLuis Bautista0% (1)
- Activities Guide and Evaluation Rubric - Unit 1 - Task 2 - Attacking and DefendingDocument9 pagesActivities Guide and Evaluation Rubric - Unit 1 - Task 2 - Attacking and Defendingsteven alvarezNo ratings yet