Download as pdf or txt
You might also like
- Wedding Cake ContractDocument3 pagesWedding Cake ContractktetchillNo ratings yet
- Student Personal Information Form PDFDocument1 pageStudent Personal Information Form PDFLouie Giray100% (2)
- Criteria For Curriculum AssessmentDocument2 pagesCriteria For Curriculum AssessmentMyka Robles89% (19)
- Hostel Allotment Form 2017-18: Saira Girls Paying GuestDocument12 pagesHostel Allotment Form 2017-18: Saira Girls Paying GuestPampa KarNo ratings yet
- MONTANARI+R+Brll's Companion To Ancient Greek Scholarship. 1 & 2 (2015)Document1,533 pagesMONTANARI+R+Brll's Companion To Ancient Greek Scholarship. 1 & 2 (2015)Anderson Zalewski Vargas100% (5)
- Uranus in Sagittarius in 12th HouseDocument1 pageUranus in Sagittarius in 12th HouseMoraru Mariana100% (1)
- Initial Application Kindergarten REVISEDDocument2 pagesInitial Application Kindergarten REVISEDSir CalaqueiNo ratings yet
- Camp RegistrationDocument1 pageCamp RegistrationlegacyofbobNo ratings yet
- Service AgreementDocument1 pageService AgreementOlrick DejaunoNo ratings yet
- Application Form InitialDocument2 pagesApplication Form InitialSaori NagaseNo ratings yet
- Housing & Dining Application: Texas Wesleyan UniversityDocument4 pagesHousing & Dining Application: Texas Wesleyan UniversityKevin WhitesideNo ratings yet
- IMLS - Customer Information SheetDocument1 pageIMLS - Customer Information SheetMark Lester OgotNo ratings yet
- HH Payment and Receipt SummaryDocument1 pageHH Payment and Receipt SummaryTemple Beth Sholom100% (2)
- Membership Application 17-18Document2 pagesMembership Application 17-18api-228956733No ratings yet
- 00 CP Rental Application (Updated 2023-02)Document1 page00 CP Rental Application (Updated 2023-02)g7pp8djyvhNo ratings yet
- Ancianos Client ProfileDocument2 pagesAncianos Client ProfileRico LedesmaNo ratings yet
- Tenant Information SheetDocument2 pagesTenant Information SheetAk rajput MarcosNo ratings yet
- HR Action Form Editable PDFDocument3 pagesHR Action Form Editable PDFManishaNo ratings yet
- Patient/Client Information Form - Animal Medical ClinicDocument1 pagePatient/Client Information Form - Animal Medical ClinicArchetype ProductionsNo ratings yet
- Transcript - Letter Request FormDocument2 pagesTranscript - Letter Request FormHung Kwan1 KeungNo ratings yet
- Application For RentalDocument3 pagesApplication For RentalreenywNo ratings yet
- 02 23 09 Travel Camp RegistrationDocument2 pages02 23 09 Travel Camp RegistrationEwing Township, NJNo ratings yet
- Private Event Contract FormDocument1 pagePrivate Event Contract FormEnergo RowerNo ratings yet
- CAR Lease Application - Ball, BrianDocument2 pagesCAR Lease Application - Ball, Brianeap6482No ratings yet
- Job ApplicationDocument4 pagesJob Applicationapi-546988246No ratings yet
- Employment / Job Application: Page 1 of 4Document4 pagesEmployment / Job Application: Page 1 of 4api-545870588No ratings yet
- Bank DetailsDocument2 pagesBank DetailshimanshuNo ratings yet
- Typing FormDocument2 pagesTyping FormSanje MakNo ratings yet
- Patient Form PDFDocument1 pagePatient Form PDFHENRYNo ratings yet
- BAY VIEW From by Abdullah Maqbool Roll No 14 Energy Engg Eve SectionDocument1 pageBAY VIEW From by Abdullah Maqbool Roll No 14 Energy Engg Eve SectionABDULLAH MAQBOOLNo ratings yet
- AOY Registration Form 2020V3Document2 pagesAOY Registration Form 2020V3PaulNo ratings yet
- Warranty Form (1688)Document2 pagesWarranty Form (1688)Debbie ButtonNo ratings yet
- Will'S Kmart/Will'S 199 Samgyupsal: Application Form A. Personal Data Application Date: SEPT 14, 2021Document2 pagesWill'S Kmart/Will'S 199 Samgyupsal: Application Form A. Personal Data Application Date: SEPT 14, 2021KYLA CABALLESNo ratings yet
- Application to Rent -Mario Fillable PDFDocument1 pageApplication to Rent -Mario Fillable PDFjustice.whitehurstNo ratings yet
- Application Form 2023 For Sureway Promotions Inc.Document4 pagesApplication Form 2023 For Sureway Promotions Inc.rchnrngl18No ratings yet
- Residential Rental ApplicationDocument3 pagesResidential Rental Applicationphoebekapoor5037No ratings yet
- WN Volunteer Training ApplicationDocument3 pagesWN Volunteer Training ApplicationKitsilano HouseNo ratings yet
- Verification of EmploymentDocument1 pageVerification of EmploymentBaby ShowerNo ratings yet
- DCC Application For Admission - 230926 - 210621Document2 pagesDCC Application For Admission - 230926 - 210621Krispin FongNo ratings yet
- Receipt (2) MarkupDocument2 pagesReceipt (2) MarkupAllen E. MartinNo ratings yet
- KamoshitaDocument4 pagesKamoshitaapi-532097424No ratings yet
- Sellers Information Worksheet: Ortgage NformationDocument1 pageSellers Information Worksheet: Ortgage Nformationapi-482673140No ratings yet
- Pre AdmissionsformDocument2 pagesPre Admissionsformapi-199090503No ratings yet
- Examination Fee ReceiptDocument1 pageExamination Fee ReceiptKushal Pratap RajawatNo ratings yet
- George Street, Brisbane City, ApplicationDocument4 pagesGeorge Street, Brisbane City, ApplicationtranvochienthangNo ratings yet
- Residental Rental ApplicationDocument6 pagesResidental Rental ApplicationJoy FrieseNo ratings yet
- Client Intake FormDocument2 pagesClient Intake Formapi-255276593100% (1)
- KR 1Document1 pageKR 1angelicapapas1597No ratings yet
- Internal Application FormDocument3 pagesInternal Application Formfd8rq2rvmyNo ratings yet
- Mps Retail PVT LTD.: Personal DetailsDocument4 pagesMps Retail PVT LTD.: Personal DetailsSelvarajNo ratings yet
- SLB ApplicationDocument2 pagesSLB Applicationapi-317585432No ratings yet
- School Trip Form ApprovalDocument1 pageSchool Trip Form ApprovalspoonkyspiderNo ratings yet
- SFR Investments: Rental ApplicationDocument6 pagesSFR Investments: Rental ApplicationgigiNo ratings yet
- British Virgin IslandsDocument2 pagesBritish Virgin IslandsNoushin ShaikNo ratings yet
- Reimbursement Request FormDocument1 pageReimbursement Request FormdebralcampNo ratings yet
- Tenant ApplicationDocument2 pagesTenant ApplicationHoggz PhotographyNo ratings yet
- Contact InformationDocument1 pageContact InformationDevin HouseholderNo ratings yet
- 00 CP Rental Application 3Document2 pages00 CP Rental Application 3g7pp8djyvhNo ratings yet
- Employment / Job Application: Personal InformationDocument4 pagesEmployment / Job Application: Personal Informationapi-532516385No ratings yet
- My New Questionnaire in 2003Document3 pagesMy New Questionnaire in 2003SuniliNo ratings yet
- CAR Application - Marsh, KDocument2 pagesCAR Application - Marsh, Keap6482No ratings yet
- MontoyaDocument4 pagesMontoyaapi-531942769No ratings yet
- Simple Preschool Registration FormDocument3 pagesSimple Preschool Registration FormSir CalaqueiNo ratings yet
- Sample Preschool Registration FormDocument4 pagesSample Preschool Registration FormSir CalaqueiNo ratings yet
- Initial Application Kindergarten REVISEDDocument2 pagesInitial Application Kindergarten REVISEDSir CalaqueiNo ratings yet
- Extended Daycare Registration FormDocument1 pageExtended Daycare Registration FormSir CalaqueiNo ratings yet
- Formal Preschool Registration Form in PDFDocument2 pagesFormal Preschool Registration Form in PDFSir CalaqueiNo ratings yet
- SWK291 - JAN - 2021 - Exam PaperDocument3 pagesSWK291 - JAN - 2021 - Exam PaperKng LayHongNo ratings yet
- Lesson Plan Fractions RobotDocument6 pagesLesson Plan Fractions Robotapi-372535556No ratings yet
- CS Form No. 212 PDS Sample Juan Macabugto Dela CruzDocument4 pagesCS Form No. 212 PDS Sample Juan Macabugto Dela CruzJANE PAGLINAWANNo ratings yet
- 16 MLT PDFDocument148 pages16 MLT PDFTanveer100% (1)
- Deped Early Language Literacy and Numeracy Program Salve J. Hosain and Liza Marie M. Manoos PDFDocument11 pagesDeped Early Language Literacy and Numeracy Program Salve J. Hosain and Liza Marie M. Manoos PDFmoreforlessprintsNo ratings yet
- EE481 Course SpecificationsDocument9 pagesEE481 Course SpecificationsahmedNo ratings yet
- Eylf Belonging Being Becoming PDFDocument2 pagesEylf Belonging Being Becoming PDFMarcusNo ratings yet
- L'Aventure Secondary School Mathematics School Based Assessment (SBA)Document17 pagesL'Aventure Secondary School Mathematics School Based Assessment (SBA)Natasha JohnsonNo ratings yet
- 2020-2021 Syllabus: AP English Literature and CompositionDocument7 pages2020-2021 Syllabus: AP English Literature and CompositionNour AllahhamNo ratings yet
- Harry PotterDocument3 pagesHarry Potterapi-528364692No ratings yet
- Nicole A. Rosario 11 - Animation Practical Research Lesson 1 What I KnowDocument7 pagesNicole A. Rosario 11 - Animation Practical Research Lesson 1 What I KnowAnalyn RosarioNo ratings yet
- Annex 4 Identifying Priority Improvement AreasDocument2 pagesAnnex 4 Identifying Priority Improvement AreasNica SalentesNo ratings yet
- Evaluation - Tyes, Tests, ToolsDocument15 pagesEvaluation - Tyes, Tests, ToolsJOSLINNo ratings yet
- Adult Learning PrinciplesDocument7 pagesAdult Learning PrinciplesmonaNo ratings yet
- HBSC1203 V2Document6 pagesHBSC1203 V2TAY JIUN HOANG MoeNo ratings yet
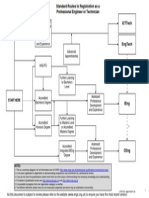
- Ceng Flowchart Showing Standard Routes To RegistrationDocument1 pageCeng Flowchart Showing Standard Routes To RegistrationAkinbode Sunday OluwagbengaNo ratings yet
- Fraction Lesson PlanDocument3 pagesFraction Lesson Planapi-286475437No ratings yet
- Internship Report On Oxford BooksDocument54 pagesInternship Report On Oxford BooksMaryam KhadimNo ratings yet
- Circular of Harvard Model Congress Leadership Summer CampDocument2 pagesCircular of Harvard Model Congress Leadership Summer Campegboezinne12No ratings yet
- Jurnal Pengembangan Profesi Guru Madrasah SwastaDocument18 pagesJurnal Pengembangan Profesi Guru Madrasah SwastaAndiSuhandiNo ratings yet
- BSC Management and Security Studies: BusinessDocument6 pagesBSC Management and Security Studies: BusinessToby LimNo ratings yet
- Japan-Imf Scholarship Program For Asia: To Foster Future Macroeconomic PolicymakersDocument34 pagesJapan-Imf Scholarship Program For Asia: To Foster Future Macroeconomic PolicymakersimanNo ratings yet
- Math-6-DLP-Quarter-3-Week-4 Day 5Document4 pagesMath-6-DLP-Quarter-3-Week-4 Day 5Rubin RubinNo ratings yet
- 2012-13 Graduate ErbulletinDocument452 pages2012-13 Graduate ErbulletinAlqoshYimedMathwathaNo ratings yet
- LegoDocument3 pagesLegomohammadNo ratings yet
- Cambridge International Examinations: Physics 0625/23 May/June 2017Document3 pagesCambridge International Examinations: Physics 0625/23 May/June 2017Mignus CarlsenNo ratings yet
- Orientation Manual: Your First Step Towards A Brighter FutureDocument18 pagesOrientation Manual: Your First Step Towards A Brighter FutureMeer MomiNo ratings yet