Download as pdf or txt
You might also like
- Now I Know 4 Students BookDocument101 pagesNow I Know 4 Students BookMaharramli Zarifa100% (9)
- Manthena VantaluDocument7 pagesManthena Vantalukalyani200996% (25)
- Bolus Vs ContinuousDocument5 pagesBolus Vs ContinuousMiaNo ratings yet
- NutritionDocument27 pagesNutritionjoke clubNo ratings yet
- Home Blenderized Tube Feeding: A Practical Guide For Clinical PracticeDocument4 pagesHome Blenderized Tube Feeding: A Practical Guide For Clinical PracticeFitri WulandariNo ratings yet
- Articulo-Blenderized Tube FeedingsDocument30 pagesArticulo-Blenderized Tube FeedingsXimena GarcíaNo ratings yet
- Blended Tube Feeding Prevalence, Ef Ficacy, and Safety: What Does The Literature Say?Document8 pagesBlended Tube Feeding Prevalence, Ef Ficacy, and Safety: What Does The Literature Say?Fitri WulandariNo ratings yet
- Peripheral Parental NutritionDocument11 pagesPeripheral Parental Nutritiontaner_soysurenNo ratings yet
- 1 s2.0 S0021755721000991 MainDocument8 pages1 s2.0 S0021755721000991 MainF Gonzales XtlvNo ratings yet
- Enteral Nutrition: Sanja KolačekDocument5 pagesEnteral Nutrition: Sanja KolačekManuela MontesNo ratings yet
- Baby-Led Weaning: What A Systematic Review of The Literature Adds OnDocument11 pagesBaby-Led Weaning: What A Systematic Review of The Literature Adds OnMacarena VargasNo ratings yet
- April Church Enteral Nutrition Product Formulations ADocument24 pagesApril Church Enteral Nutrition Product Formulations Aivan.purca3No ratings yet
- Chapter One - ThreeDocument26 pagesChapter One - ThreeSamson ikenna OkonkwoNo ratings yet
- Prebiotic Supplementation Improves Apetite Control in Children With Overweight and Obesity, A Randomized Controlled TrialDocument11 pagesPrebiotic Supplementation Improves Apetite Control in Children With Overweight and Obesity, A Randomized Controlled TrialJUAN SEBASTIAN AVELLANEDA MARTINEZNo ratings yet
- Freire Opazo BLWDocument25 pagesFreire Opazo BLWAmi R. VirueteNo ratings yet
- MT-Campoy C, Campos D, Cerdó T Et Al Complementary Feeding in Developed Countries-The 3 Ws (When, What, and WhyDocument10 pagesMT-Campoy C, Campos D, Cerdó T Et Al Complementary Feeding in Developed Countries-The 3 Ws (When, What, and WhyCaro FreireNo ratings yet
- Do South Asian Nutrition Guidelines For Critically Ill Recommend Commercial Feeds or Blended Tube Feeds? - A Narrative ReviewDocument5 pagesDo South Asian Nutrition Guidelines For Critically Ill Recommend Commercial Feeds or Blended Tube Feeds? - A Narrative ReviewFitri WulandariNo ratings yet
- Javma-Javma 2001 218 705Document5 pagesJavma-Javma 2001 218 705ErikkuOtakuNo ratings yet
- Pulse Crop Effects On Gut Microbial Populations, Intestinal Function, and Adiposity in A Mouse Model of Diet-Induced Obesity John N. McginleyDocument40 pagesPulse Crop Effects On Gut Microbial Populations, Intestinal Function, and Adiposity in A Mouse Model of Diet-Induced Obesity John N. Mcginleyzora.mendez637100% (10)
- Jurnal PICO 1 PDFDocument5 pagesJurnal PICO 1 PDFrikaNo ratings yet
- Restrictive Feeding and Excessive Hunger in Young Children With Obesity: A Case SeriesDocument6 pagesRestrictive Feeding and Excessive Hunger in Young Children With Obesity: A Case SeriespingkyNo ratings yet
- Alimentatia Complementara MetodeDocument15 pagesAlimentatia Complementara MetodeIoana IsarieNo ratings yet
- North American GuidesDocument5 pagesNorth American Guidesnta.gloffkaNo ratings yet
- Physicochemical and Nutricional Characteristics of Handmade Enteral DietsDocument7 pagesPhysicochemical and Nutricional Characteristics of Handmade Enteral DietsFitri WulandariNo ratings yet
- 1 s2.0 S2405457723000979 MainDocument8 pages1 s2.0 S2405457723000979 MainJ CNo ratings yet
- Foods: Alternatives To Cow's Milk-Based Infant Formulas in The Prevention and Management of Cow's Milk AllergyDocument40 pagesFoods: Alternatives To Cow's Milk-Based Infant Formulas in The Prevention and Management of Cow's Milk AllergyClaudia Andreea StroiaNo ratings yet
- CrossmDocument14 pagesCrossmIra DwijayantiNo ratings yet
- Nut in Clin Prac - 2023 - Mohamed Elfadil - Peptide Based Formula Clinical Applications and BenefitsDocument11 pagesNut in Clin Prac - 2023 - Mohamed Elfadil - Peptide Based Formula Clinical Applications and BenefitshizburNo ratings yet
- The Use of Prebiotics and Probiotics in Infant FormulaDocument3 pagesThe Use of Prebiotics and Probiotics in Infant Formula517wangyiqiNo ratings yet
- Saint Louis University School of Nursing Nutrition Return DemonstrationDocument4 pagesSaint Louis University School of Nursing Nutrition Return DemonstrationShaina Fe RabaneraNo ratings yet
- 2012 Complementary Feeding Book FinalDocument37 pages2012 Complementary Feeding Book FinalpingkanppNo ratings yet
- Consideraciones Al Planear Dietas Veganas en BebésDocument8 pagesConsideraciones Al Planear Dietas Veganas en BebésLuciano MirianiNo ratings yet
- Clinical NutritionDocument6 pagesClinical NutritionaliyaNo ratings yet
- Risks and Benefits of Vegan and Vegetarian Diets in ChildrenDocument6 pagesRisks and Benefits of Vegan and Vegetarian Diets in ChildrenMostafa McheikNo ratings yet
- Comparative Nutrient Analysis of Regular Organic and Homemade Infant and Toddler Foods 2472 1182 1000119Document6 pagesComparative Nutrient Analysis of Regular Organic and Homemade Infant and Toddler Foods 2472 1182 1000119Anonymous LJTx5UztNo ratings yet
- Studyprotocol Open AccessDocument11 pagesStudyprotocol Open Accesshye jinNo ratings yet
- Proximate Composition of Fortified Filipino Snacks For Picky EatersDocument9 pagesProximate Composition of Fortified Filipino Snacks For Picky EatersDa Eun Ji HyeNo ratings yet
- PIIS2475299124000118Document18 pagesPIIS2475299124000118Reeds LaurelNo ratings yet
- A. Fnri and Food Guide Pyramid: George Dewey Medical CollegeDocument4 pagesA. Fnri and Food Guide Pyramid: George Dewey Medical CollegeTheresa FortalezaNo ratings yet
- J Human Nutrition Diet - 2018 - Breaks - Blended Diets For Gastrostomy Fed Children and Young People A Scoping ReviewDocument13 pagesJ Human Nutrition Diet - 2018 - Breaks - Blended Diets For Gastrostomy Fed Children and Young People A Scoping ReviewMARDONES MEJIAS KATTERINE NICOLENo ratings yet
- TPN Ensuring Safe and Appropriate Use ASHP 2017Document54 pagesTPN Ensuring Safe and Appropriate Use ASHP 2017Michael FreudigerNo ratings yet
- 1 s2.0 S0195666318313412 MainDocument10 pages1 s2.0 S0195666318313412 MainRomane AracenaNo ratings yet
- Am J Clin Nutr 2007 Fewtrell 635S 8SggDocument4 pagesAm J Clin Nutr 2007 Fewtrell 635S 8SggMariaNo ratings yet
- Feeding The Premature InfantDocument3 pagesFeeding The Premature InfantMano RanjaniNo ratings yet
- J of App Behav Analysis - 2023 - Haney - An Evaluation of Negative Reinforcement To Increase Self Feeding and Self DrinkingDocument20 pagesJ of App Behav Analysis - 2023 - Haney - An Evaluation of Negative Reinforcement To Increase Self Feeding and Self DrinkingmarwaNo ratings yet
- Alimentos Funcionais em UanDocument12 pagesAlimentos Funcionais em UanEduardo MartinsNo ratings yet
- Nutrients 15 02244Document14 pagesNutrients 15 02244rafrejuNo ratings yet
- A Disseration Submitted As A Partial Fulfilment For Award of The Diploma in Community Nutrition.Document8 pagesA Disseration Submitted As A Partial Fulfilment For Award of The Diploma in Community Nutrition.Prince HakimNo ratings yet
- Diet SeratDocument7 pagesDiet Seratpenyimpanankoas8No ratings yet
- 395 FullDocument7 pages395 Fullsundaybush045No ratings yet
- Fomula Standar Lactante BIREF 2017Document4 pagesFomula Standar Lactante BIREF 2017HakundusNo ratings yet
- Abeshu, Lelisa, Geleta - 2016 - Complementary Feeding Review of Recommendations, Feeding Practices, and Adequacy of Homemade ComplemenDocument9 pagesAbeshu, Lelisa, Geleta - 2016 - Complementary Feeding Review of Recommendations, Feeding Practices, and Adequacy of Homemade ComplemenSeptian TheaNo ratings yet
- Fnut 03 00041Document9 pagesFnut 03 00041Arie Dwi ANo ratings yet
- Weaning Foods-Nutrition PerspectiveDocument10 pagesWeaning Foods-Nutrition PerspectivemadhujayarajNo ratings yet
- E20160772 FullDocument10 pagesE20160772 FullRaehana AlaydrusNo ratings yet
- NAH Determinants of Normal Nutrition Among 0-59-Month-Old Filipino Children Living in Low-Income HouseholdsDocument12 pagesNAH Determinants of Normal Nutrition Among 0-59-Month-Old Filipino Children Living in Low-Income Householdsnung09No ratings yet
- 1 s2.0 S0195666316305645 MainDocument7 pages1 s2.0 S0195666316305645 MainCaritoSanchezNo ratings yet
- Diet As Adjunctive Treatment For Inflammatory Bowel Disease: Review and Update of The Latest LiteratureDocument13 pagesDiet As Adjunctive Treatment For Inflammatory Bowel Disease: Review and Update of The Latest LiteratureNejc KovačNo ratings yet
- Medicamentos e AlimentosDocument8 pagesMedicamentos e AlimentosPhilipe VieiraNo ratings yet
- Appetite: Hannah Rowan, Cristen HarrisDocument4 pagesAppetite: Hannah Rowan, Cristen HarrisSofia GkanaNo ratings yet
- Timely Introduction of Complementary Feeding Among Caregivers of Children 612 Month Sodo Town EthiopiaDocument3 pagesTimely Introduction of Complementary Feeding Among Caregivers of Children 612 Month Sodo Town EthiopiaProdi S1- 1BNo ratings yet
- Kilimo Komaswa 2Document8 pagesKilimo Komaswa 2joseenyamaoNo ratings yet
- NRM Pig Nutrition Guide A5-FINALDocument32 pagesNRM Pig Nutrition Guide A5-FINALOkechukwu KaluNo ratings yet
- Nutrition and Physical Activity - An Obesity Medicine Association (OMA) Clinical Practice Statement 2022Document16 pagesNutrition and Physical Activity - An Obesity Medicine Association (OMA) Clinical Practice Statement 2022nur ainiNo ratings yet
- Ageloc Tr90 Flyer EngDocument2 pagesAgeloc Tr90 Flyer EngAinNo ratings yet
- Blue Lake Dairy Group Pty LTD: Finished Product SpecificationDocument3 pagesBlue Lake Dairy Group Pty LTD: Finished Product SpecificationmarilouNo ratings yet
- Biodiversity and The Healthy SocietyDocument25 pagesBiodiversity and The Healthy SocietyCarmela Grace RamosNo ratings yet
- Use of Trina Dhanya According To Aahara Vidhi VishDocument4 pagesUse of Trina Dhanya According To Aahara Vidhi Vishumapati 1505No ratings yet
- Perilaku Komsumsi Buah Dan Sayur Anak Sekolah Dasar Negeri 020583 Binjai EstateDocument8 pagesPerilaku Komsumsi Buah Dan Sayur Anak Sekolah Dasar Negeri 020583 Binjai Estateahmad yusniNo ratings yet
- Pentaksiran Sumatif Pertengahan Tahun 2021 - Cefr English Form 1 (Reading) 3Document8 pagesPentaksiran Sumatif Pertengahan Tahun 2021 - Cefr English Form 1 (Reading) 3angora6750232No ratings yet
- SkillsDocument26 pagesSkillsMariana ParfenieNo ratings yet
- 2 Leaf SamplingDocument4 pages2 Leaf SamplingShami KamisNo ratings yet
- Sleep Health and The Connection To Nutrition 1Document11 pagesSleep Health and The Connection To Nutrition 1api-534396790No ratings yet
- Acr.2 NCM119 (Monreal)Document4 pagesAcr.2 NCM119 (Monreal)Karen Joy MonrealNo ratings yet
- BeynenAC2018 BeetpulpindogfoodDocument8 pagesBeynenAC2018 BeetpulpindogfoodaquarianchemNo ratings yet
- Product Specifications: CreamDocument1 pageProduct Specifications: CreamJason Thornton0% (1)
- Đề Kiểm Tra Đt Lần 4 - KeyDocument20 pagesĐề Kiểm Tra Đt Lần 4 - KeyPhuong AnhNo ratings yet
- NRC Kucing Dan AnjingDocument2 pagesNRC Kucing Dan AnjingAdelia Rosa MahadewiNo ratings yet
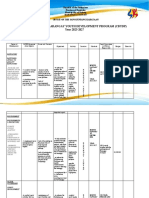
- Cauyan Comprehensive-Barangay-Youth-Development-PlanDocument9 pagesCauyan Comprehensive-Barangay-Youth-Development-PlanKENNETH ANINZONo ratings yet
- A Multiobjective Diet Planning Model For Diabetic Patients in The Moroccan Health Context Using Particle Swarm Intelligence RedDocument11 pagesA Multiobjective Diet Planning Model For Diabetic Patients in The Moroccan Health Context Using Particle Swarm Intelligence Redabdellah.ahouragNo ratings yet
- Nutrition PDFDocument53 pagesNutrition PDFclean makeNo ratings yet
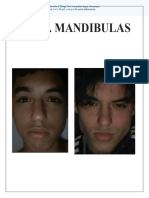
- Mr. Mandibulas: Subscribe To Deepl Pro To Translate Larger Documents. Visit For More InformationDocument87 pagesMr. Mandibulas: Subscribe To Deepl Pro To Translate Larger Documents. Visit For More Informationav495600No ratings yet
- Gizi Perkotaan - Pertemuan 2Document20 pagesGizi Perkotaan - Pertemuan 2natasya amabelNo ratings yet
- Hfen Diet Week 1Document17 pagesHfen Diet Week 1CherryNo ratings yet
- Resume JD MiddletonDocument1 pageResume JD Middletonapi-252717471No ratings yet
- Usda Food GuideDocument7 pagesUsda Food GuideSiegrend GarboNo ratings yet
- Discharge PlanDocument2 pagesDischarge PlanAnjae GariandoNo ratings yet
- BIOL 203 Written AssignmentDocument8 pagesBIOL 203 Written AssignmentLucia LeiNo ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Intervention and Rationale EvaluationDocument23 pagesNursing Care Plan Assessment Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Intervention and Rationale EvaluationyusivileidyNo ratings yet