
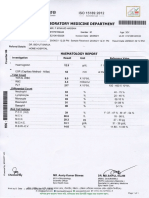
Hemoglobin Concentration
Hemoglobin Concentration
You might also like
- Camera de Numarat Improved NeubauerDocument4 pagesCamera de Numarat Improved NeubauerGeoemilia1No ratings yet
- Lab 9 HemocytometerDocument23 pagesLab 9 HemocytometerRi ChardNo ratings yet
- HW1 Su 10Document3 pagesHW1 Su 10Dylan MaraisNo ratings yet
- Cell Counting HemocytometerDocument4 pagesCell Counting HemocytometerJuan Dela CruzNo ratings yet
- 01.30.55.110-Yeast Propagation and Management 2008 PDFDocument23 pages01.30.55.110-Yeast Propagation and Management 2008 PDFÁnhXuânPhạmNo ratings yet
- Vitamin K TOFDocument5 pagesVitamin K TOFNanank Akhiruddin SyamsaNo ratings yet
- Jenny, Bingham, Padilla-Saravia. 1948. Nitrogen and Organic Matter Contents of Equatorial Soils of Colombia, South AmericaDocument14 pagesJenny, Bingham, Padilla-Saravia. 1948. Nitrogen and Organic Matter Contents of Equatorial Soils of Colombia, South AmericaMaria Victoria Ortega RamosNo ratings yet
- Reliable Tool For: Blood Alcohol Concentration Using Salivary Stick: Departments?Document4 pagesReliable Tool For: Blood Alcohol Concentration Using Salivary Stick: Departments?Lucky_megaNo ratings yet
- Dengue ReportDocument3 pagesDengue Reportakashdeepsharma109No ratings yet
- The First Observation of HB Thalassaemia English Family With of Unsuspected Thalassaemia Minor Its MembersDocument5 pagesThe First Observation of HB Thalassaemia English Family With of Unsuspected Thalassaemia Minor Its MembersChan DavidNo ratings yet
- Morphology and Citric Acid Production of AspergillDocument7 pagesMorphology and Citric Acid Production of AspergillJames ZackNo ratings yet
- Research Memorandum: National Advisory Committee For AeronauticsDocument39 pagesResearch Memorandum: National Advisory Committee For AeronauticsnileshraneNo ratings yet
- Epic 0002Document1 pageEpic 0002Chota BheemNo ratings yet
- L/Ylok: Janasnehi Healthcare Medical SpecialityDocument2 pagesL/Ylok: Janasnehi Healthcare Medical SpecialityRenukaprasad K RNo ratings yet
- مصدر 8Document15 pagesمصدر 8Alaa AskNo ratings yet
- #Relation Betn Speed and Oil Layr ThicknessDocument9 pages#Relation Betn Speed and Oil Layr ThicknessDayee MunafNo ratings yet
- Pharmacology,: CollegeDocument18 pagesPharmacology,: CollegearyNo ratings yet
- Statistics in Metabolomics: David Banks Isds Duke UniversityDocument41 pagesStatistics in Metabolomics: David Banks Isds Duke Universityvijay2109No ratings yet
- Orifice Flow.: IntroductoryDocument14 pagesOrifice Flow.: IntroductoryAhmedNo ratings yet
- Ni Ni: TfferffiftDocument1 pageNi Ni: Tfferffiftthein zawNo ratings yet
- The Preparation and Function of The Hypertensin-Converting EnzymeDocument5 pagesThe Preparation and Function of The Hypertensin-Converting EnzymeDana MNo ratings yet
- Measurement of The Effects of Physical and Chemical Variables On Bubble SizeDocument11 pagesMeasurement of The Effects of Physical and Chemical Variables On Bubble SizerajuvadlakondaNo ratings yet
- Tsai 1999Document2 pagesTsai 1999kontiki500No ratings yet
- Sedimentation in Tilted VesselsDocument12 pagesSedimentation in Tilted Vessels2306노강민No ratings yet
- Prothrombin Time in Dicoumarol TherapyDocument4 pagesProthrombin Time in Dicoumarol TherapyplsssssNo ratings yet
- Nautical Almanac 1992Document66 pagesNautical Almanac 1992vishnu kNo ratings yet
- John Macgillivray: SoilDocument6 pagesJohn Macgillivray: SoilagusNo ratings yet
- Perhitungan Dan Ralat Modul 6 PERCOBAAN MELDEDocument18 pagesPerhitungan Dan Ralat Modul 6 PERCOBAAN MELDEGusni HayatiNo ratings yet
- Two-Phase Flow Split at T Junctions Effect of Side Arm Orientation and Downstream GeometryDocument15 pagesTwo-Phase Flow Split at T Junctions Effect of Side Arm Orientation and Downstream GeometryRoss WaringNo ratings yet
- Carrier Lifetime Meassurement in PIN DiodesDocument5 pagesCarrier Lifetime Meassurement in PIN DiodesGuillermo VillarNo ratings yet
- Spector 1966Document20 pagesSpector 1966Rah MliNo ratings yet
- Abeygunawardena 1990Document15 pagesAbeygunawardena 1990Paula Andrea Castro MartinezNo ratings yet
- The Effect of Systox On Ionic Fluxes in Excised Barley RootsDocument10 pagesThe Effect of Systox On Ionic Fluxes in Excised Barley RootsSh1vaNo ratings yet
- Aerosol Penetration ThroughDocument8 pagesAerosol Penetration ThroughAndré Louiz FerreiraNo ratings yet
- Harman PDFDocument1 pageHarman PDFKhusNo ratings yet
- Bartsch 1978Document10 pagesBartsch 1978SaphiraNo ratings yet
- Flooding Characteristics and Separation Efficiencies of Pulsed Sieve-Pla Te ExtractionDocument6 pagesFlooding Characteristics and Separation Efficiencies of Pulsed Sieve-Pla Te ExtractionArunNo ratings yet
- Hem Lab Manual DiffDocument9 pagesHem Lab Manual DiffFatima Mae LusanNo ratings yet
- Well Test Previous Year QuestionDocument13 pagesWell Test Previous Year QuestionDiptoNo ratings yet
- Alzheimer'S Disease and Their Relationship To Ageing and To TheDocument16 pagesAlzheimer'S Disease and Their Relationship To Ageing and To Thedimitri pizarnikNo ratings yet
- Physics Ideal Gas Law NotesDocument5 pagesPhysics Ideal Gas Law NotesSeblewengelNo ratings yet
- Benson 1975, Comparaison Phtalayade Et FluorescamineDocument4 pagesBenson 1975, Comparaison Phtalayade Et Fluorescaminearnaud.fillaudeau44No ratings yet
- Chemistry at The InterfaceDocument28 pagesChemistry at The Interfacebm OUREMNo ratings yet
- Diabetes SensingDocument5 pagesDiabetes SensingmovirjonneNo ratings yet
- Importance of The C7+ Fraction in Phase Behavior Calculations PDFDocument7 pagesImportance of The C7+ Fraction in Phase Behavior Calculations PDFAndrés Eduardo Guzmán VelásquezNo ratings yet
- Chemical PathologyDocument8 pagesChemical PathologyBobskinnyNo ratings yet
- Accencix 3: Field: Is Values in TwoDocument4 pagesAccencix 3: Field: Is Values in TwoArdion Fikri ZatamiNo ratings yet
- 6 C00017457Document6 pages6 C00017457Schwab RealHumanNo ratings yet
- Litx Oo :, Al/L .V'I 1 I/Lgd "1 L - JDocument6 pagesLitx Oo :, Al/L .V'I 1 I/Lgd "1 L - JSinhro018No ratings yet
- Head Packs 3Document5 pagesHead Packs 3Blanca LechugaNo ratings yet
- D.D.S., MS., P. L.D.S., PH.D.: of Michigan, School of Dentistry, Ann Arbor, MichDocument17 pagesD.D.S., MS., P. L.D.S., PH.D.: of Michigan, School of Dentistry, Ann Arbor, MichErika Stephany ValenciaNo ratings yet
- Amp, 255-60Document6 pagesAmp, 255-60adslainerNo ratings yet
- V.-Design 0 A.&Cro Cale - Liq& Chromat Graph-And ITS Application To - Cl4Tion-Exchange Separation of Alkali MetalsDocument8 pagesV.-Design 0 A.&Cro Cale - Liq& Chromat Graph-And ITS Application To - Cl4Tion-Exchange Separation of Alkali MetalsZulNo ratings yet
- 2lewsi Dexter ASD 09.fullDocument17 pages2lewsi Dexter ASD 09.fullprasannasimhaNo ratings yet
- Banco de Baterias ExDocument1 pageBanco de Baterias ExuserapenasNo ratings yet
- 1 s2.0 0090429589903166 MainDocument5 pages1 s2.0 0090429589903166 MainJHON BRAYAN HUANACUNI CONDORINo ratings yet
- Temperature and Water Resistivity: Stafford County, Kansas ViolaDocument8 pagesTemperature and Water Resistivity: Stafford County, Kansas ViolapotNo ratings yet
- Img 20210626 0004Document9 pagesImg 20210626 0004Ñîhâj Æhâmmâd MîstrîNo ratings yet
- Laboratotl'I: IllljDocument1 pageLaboratotl'I: IllljMuhammad TahseenNo ratings yet
- Ambrose1975 - 2 Avaliação ManhãDocument4 pagesAmbrose1975 - 2 Avaliação ManhãSil Franciley QuaresmaNo ratings yet
- Towler Transurethral14346Document4 pagesTowler Transurethral14346Dian NovitasariNo ratings yet
- Paper About AirliftDocument10 pagesPaper About Airliftlrodriguez_892566No ratings yet
- Hydrodynamics Effect PipeDocument4 pagesHydrodynamics Effect PipenuvanNo ratings yet
- Payne 196323Document7 pagesPayne 196323vsvsuresh2099No ratings yet
- Counting of Blood CellsDocument7 pagesCounting of Blood CellsPASUPULA JAGADEESHNo ratings yet
- Presentation On Aber Countstar PDFDocument35 pagesPresentation On Aber Countstar PDFchequillasNo ratings yet
- Applied Microbiology Fall 2015Document56 pagesApplied Microbiology Fall 2015Le HungNo ratings yet
- Monitoring Fermentation With An Aber Yeast MonitorDocument30 pagesMonitoring Fermentation With An Aber Yeast MonitorBahiru Bt0% (1)
- Phyto TechniquesDocument13 pagesPhyto TechniquesIsmail JabbarNo ratings yet
- Antimicrobial Products-Test For Antimicrobial Activity and EfficacyDocument14 pagesAntimicrobial Products-Test For Antimicrobial Activity and EfficacyherfuentesNo ratings yet
- Principle of Biochemical Engineering: Manam Walait Lecturer FLS, UCP LahoreDocument23 pagesPrinciple of Biochemical Engineering: Manam Walait Lecturer FLS, UCP LahoreJawadNo ratings yet
- Pro64-E-01 Body Fluid SOPDocument14 pagesPro64-E-01 Body Fluid SOPmmNo ratings yet
- P.J. Hansen: Use of A HemacytometerDocument2 pagesP.J. Hansen: Use of A HemacytometerSanti WilujengNo ratings yet
- Practical - Blood Cell Counting IDocument36 pagesPractical - Blood Cell Counting Imuny67% (3)
- Cell CountDocument2 pagesCell Countapi-305259644No ratings yet
- Automated Blood Cell Counter: Project Guide: Mr. Maniraj (Associate Professor)Document13 pagesAutomated Blood Cell Counter: Project Guide: Mr. Maniraj (Associate Professor)19R25A0422 KOLLI ABHINAVA JEEVAN TEJANo ratings yet
- Cell Counting Areas in Neubauer ChamberDocument4 pagesCell Counting Areas in Neubauer Chambernice personNo ratings yet
- Cell Counting/Viability Testing: Materials: (White Labs Product Number For Reference)Document4 pagesCell Counting/Viability Testing: Materials: (White Labs Product Number For Reference)RiyanNo ratings yet
- Cell CountDocument2 pagesCell CountBridget HaleyNo ratings yet
- Extraction and Fermentation-Based Purification of Saponins From Sapindus Mukorossi GaertnDocument10 pagesExtraction and Fermentation-Based Purification of Saponins From Sapindus Mukorossi GaertnBình MinhNo ratings yet
- Cell Counting Using A HemacytometerDocument3 pagesCell Counting Using A HemacytometerKris Cahyo Mulyatno100% (1)
- 9216 - Epifluorescence Microscopic MethodDocument2 pages9216 - Epifluorescence Microscopic Methodpollux23No ratings yet
- Introduction To Media EquipmentDocument57 pagesIntroduction To Media EquipmentLaureen CordovaNo ratings yet
- Haemocytometer PPT ANIMAL CELL CULTUREDocument30 pagesHaemocytometer PPT ANIMAL CELL CULTURESarah PavuNo ratings yet
- Fossomatic 7 and Fossomatic 7 DC - Solution - Brochure - GBDocument7 pagesFossomatic 7 and Fossomatic 7 DC - Solution - Brochure - GBManoleteNo ratings yet
- Zoology Field ReportDocument11 pagesZoology Field ReportAnu Neth ThongonNo ratings yet
- Evaluation of Sysmex XN 1000 Hematology Analyzer.49Document4 pagesEvaluation of Sysmex XN 1000 Hematology Analyzer.49ivanNo ratings yet
- Microbio Lab ReportDocument3 pagesMicrobio Lab Reportroque porcelNo ratings yet
- Theory and Measurement of Bacterial GrowthDocument11 pagesTheory and Measurement of Bacterial GrowthBi Anh100% (1)























































































Download as pdf or txt
You might also like
- Camera de Numarat Improved NeubauerDocument4 pagesCamera de Numarat Improved NeubauerGeoemilia1No ratings yet
- Lab 9 HemocytometerDocument23 pagesLab 9 HemocytometerRi ChardNo ratings yet
- HW1 Su 10Document3 pagesHW1 Su 10Dylan MaraisNo ratings yet
- Cell Counting HemocytometerDocument4 pagesCell Counting HemocytometerJuan Dela CruzNo ratings yet
- 01.30.55.110-Yeast Propagation and Management 2008 PDFDocument23 pages01.30.55.110-Yeast Propagation and Management 2008 PDFÁnhXuânPhạmNo ratings yet
- Vitamin K TOFDocument5 pagesVitamin K TOFNanank Akhiruddin SyamsaNo ratings yet
- Jenny, Bingham, Padilla-Saravia. 1948. Nitrogen and Organic Matter Contents of Equatorial Soils of Colombia, South AmericaDocument14 pagesJenny, Bingham, Padilla-Saravia. 1948. Nitrogen and Organic Matter Contents of Equatorial Soils of Colombia, South AmericaMaria Victoria Ortega RamosNo ratings yet
- Reliable Tool For: Blood Alcohol Concentration Using Salivary Stick: Departments?Document4 pagesReliable Tool For: Blood Alcohol Concentration Using Salivary Stick: Departments?Lucky_megaNo ratings yet
- Dengue ReportDocument3 pagesDengue Reportakashdeepsharma109No ratings yet
- The First Observation of HB Thalassaemia English Family With of Unsuspected Thalassaemia Minor Its MembersDocument5 pagesThe First Observation of HB Thalassaemia English Family With of Unsuspected Thalassaemia Minor Its MembersChan DavidNo ratings yet
- Morphology and Citric Acid Production of AspergillDocument7 pagesMorphology and Citric Acid Production of AspergillJames ZackNo ratings yet
- Research Memorandum: National Advisory Committee For AeronauticsDocument39 pagesResearch Memorandum: National Advisory Committee For AeronauticsnileshraneNo ratings yet
- Epic 0002Document1 pageEpic 0002Chota BheemNo ratings yet
- L/Ylok: Janasnehi Healthcare Medical SpecialityDocument2 pagesL/Ylok: Janasnehi Healthcare Medical SpecialityRenukaprasad K RNo ratings yet
- مصدر 8Document15 pagesمصدر 8Alaa AskNo ratings yet
- #Relation Betn Speed and Oil Layr ThicknessDocument9 pages#Relation Betn Speed and Oil Layr ThicknessDayee MunafNo ratings yet
- Pharmacology,: CollegeDocument18 pagesPharmacology,: CollegearyNo ratings yet
- Statistics in Metabolomics: David Banks Isds Duke UniversityDocument41 pagesStatistics in Metabolomics: David Banks Isds Duke Universityvijay2109No ratings yet
- Orifice Flow.: IntroductoryDocument14 pagesOrifice Flow.: IntroductoryAhmedNo ratings yet
- Ni Ni: TfferffiftDocument1 pageNi Ni: Tfferffiftthein zawNo ratings yet
- The Preparation and Function of The Hypertensin-Converting EnzymeDocument5 pagesThe Preparation and Function of The Hypertensin-Converting EnzymeDana MNo ratings yet
- Measurement of The Effects of Physical and Chemical Variables On Bubble SizeDocument11 pagesMeasurement of The Effects of Physical and Chemical Variables On Bubble SizerajuvadlakondaNo ratings yet
- Tsai 1999Document2 pagesTsai 1999kontiki500No ratings yet
- Sedimentation in Tilted VesselsDocument12 pagesSedimentation in Tilted Vessels2306노강민No ratings yet
- Prothrombin Time in Dicoumarol TherapyDocument4 pagesProthrombin Time in Dicoumarol TherapyplsssssNo ratings yet
- Nautical Almanac 1992Document66 pagesNautical Almanac 1992vishnu kNo ratings yet
- John Macgillivray: SoilDocument6 pagesJohn Macgillivray: SoilagusNo ratings yet
- Perhitungan Dan Ralat Modul 6 PERCOBAAN MELDEDocument18 pagesPerhitungan Dan Ralat Modul 6 PERCOBAAN MELDEGusni HayatiNo ratings yet
- Two-Phase Flow Split at T Junctions Effect of Side Arm Orientation and Downstream GeometryDocument15 pagesTwo-Phase Flow Split at T Junctions Effect of Side Arm Orientation and Downstream GeometryRoss WaringNo ratings yet
- Carrier Lifetime Meassurement in PIN DiodesDocument5 pagesCarrier Lifetime Meassurement in PIN DiodesGuillermo VillarNo ratings yet
- Spector 1966Document20 pagesSpector 1966Rah MliNo ratings yet
- Abeygunawardena 1990Document15 pagesAbeygunawardena 1990Paula Andrea Castro MartinezNo ratings yet
- The Effect of Systox On Ionic Fluxes in Excised Barley RootsDocument10 pagesThe Effect of Systox On Ionic Fluxes in Excised Barley RootsSh1vaNo ratings yet
- Aerosol Penetration ThroughDocument8 pagesAerosol Penetration ThroughAndré Louiz FerreiraNo ratings yet
- Harman PDFDocument1 pageHarman PDFKhusNo ratings yet
- Bartsch 1978Document10 pagesBartsch 1978SaphiraNo ratings yet
- Flooding Characteristics and Separation Efficiencies of Pulsed Sieve-Pla Te ExtractionDocument6 pagesFlooding Characteristics and Separation Efficiencies of Pulsed Sieve-Pla Te ExtractionArunNo ratings yet
- Hem Lab Manual DiffDocument9 pagesHem Lab Manual DiffFatima Mae LusanNo ratings yet
- Well Test Previous Year QuestionDocument13 pagesWell Test Previous Year QuestionDiptoNo ratings yet
- Alzheimer'S Disease and Their Relationship To Ageing and To TheDocument16 pagesAlzheimer'S Disease and Their Relationship To Ageing and To Thedimitri pizarnikNo ratings yet
- Physics Ideal Gas Law NotesDocument5 pagesPhysics Ideal Gas Law NotesSeblewengelNo ratings yet
- Benson 1975, Comparaison Phtalayade Et FluorescamineDocument4 pagesBenson 1975, Comparaison Phtalayade Et Fluorescaminearnaud.fillaudeau44No ratings yet
- Chemistry at The InterfaceDocument28 pagesChemistry at The Interfacebm OUREMNo ratings yet
- Diabetes SensingDocument5 pagesDiabetes SensingmovirjonneNo ratings yet
- Importance of The C7+ Fraction in Phase Behavior Calculations PDFDocument7 pagesImportance of The C7+ Fraction in Phase Behavior Calculations PDFAndrés Eduardo Guzmán VelásquezNo ratings yet
- Chemical PathologyDocument8 pagesChemical PathologyBobskinnyNo ratings yet
- Accencix 3: Field: Is Values in TwoDocument4 pagesAccencix 3: Field: Is Values in TwoArdion Fikri ZatamiNo ratings yet
- 6 C00017457Document6 pages6 C00017457Schwab RealHumanNo ratings yet
- Litx Oo :, Al/L .V'I 1 I/Lgd "1 L - JDocument6 pagesLitx Oo :, Al/L .V'I 1 I/Lgd "1 L - JSinhro018No ratings yet
- Head Packs 3Document5 pagesHead Packs 3Blanca LechugaNo ratings yet
- D.D.S., MS., P. L.D.S., PH.D.: of Michigan, School of Dentistry, Ann Arbor, MichDocument17 pagesD.D.S., MS., P. L.D.S., PH.D.: of Michigan, School of Dentistry, Ann Arbor, MichErika Stephany ValenciaNo ratings yet
- Amp, 255-60Document6 pagesAmp, 255-60adslainerNo ratings yet
- V.-Design 0 A.&Cro Cale - Liq& Chromat Graph-And ITS Application To - Cl4Tion-Exchange Separation of Alkali MetalsDocument8 pagesV.-Design 0 A.&Cro Cale - Liq& Chromat Graph-And ITS Application To - Cl4Tion-Exchange Separation of Alkali MetalsZulNo ratings yet
- 2lewsi Dexter ASD 09.fullDocument17 pages2lewsi Dexter ASD 09.fullprasannasimhaNo ratings yet
- Banco de Baterias ExDocument1 pageBanco de Baterias ExuserapenasNo ratings yet
- 1 s2.0 0090429589903166 MainDocument5 pages1 s2.0 0090429589903166 MainJHON BRAYAN HUANACUNI CONDORINo ratings yet
- Temperature and Water Resistivity: Stafford County, Kansas ViolaDocument8 pagesTemperature and Water Resistivity: Stafford County, Kansas ViolapotNo ratings yet
- Img 20210626 0004Document9 pagesImg 20210626 0004Ñîhâj Æhâmmâd MîstrîNo ratings yet
- Laboratotl'I: IllljDocument1 pageLaboratotl'I: IllljMuhammad TahseenNo ratings yet
- Ambrose1975 - 2 Avaliação ManhãDocument4 pagesAmbrose1975 - 2 Avaliação ManhãSil Franciley QuaresmaNo ratings yet
- Towler Transurethral14346Document4 pagesTowler Transurethral14346Dian NovitasariNo ratings yet
- Paper About AirliftDocument10 pagesPaper About Airliftlrodriguez_892566No ratings yet
- Hydrodynamics Effect PipeDocument4 pagesHydrodynamics Effect PipenuvanNo ratings yet
- Payne 196323Document7 pagesPayne 196323vsvsuresh2099No ratings yet
- Counting of Blood CellsDocument7 pagesCounting of Blood CellsPASUPULA JAGADEESHNo ratings yet
- Presentation On Aber Countstar PDFDocument35 pagesPresentation On Aber Countstar PDFchequillasNo ratings yet
- Applied Microbiology Fall 2015Document56 pagesApplied Microbiology Fall 2015Le HungNo ratings yet
- Monitoring Fermentation With An Aber Yeast MonitorDocument30 pagesMonitoring Fermentation With An Aber Yeast MonitorBahiru Bt0% (1)
- Phyto TechniquesDocument13 pagesPhyto TechniquesIsmail JabbarNo ratings yet
- Antimicrobial Products-Test For Antimicrobial Activity and EfficacyDocument14 pagesAntimicrobial Products-Test For Antimicrobial Activity and EfficacyherfuentesNo ratings yet
- Principle of Biochemical Engineering: Manam Walait Lecturer FLS, UCP LahoreDocument23 pagesPrinciple of Biochemical Engineering: Manam Walait Lecturer FLS, UCP LahoreJawadNo ratings yet
- Pro64-E-01 Body Fluid SOPDocument14 pagesPro64-E-01 Body Fluid SOPmmNo ratings yet
- P.J. Hansen: Use of A HemacytometerDocument2 pagesP.J. Hansen: Use of A HemacytometerSanti WilujengNo ratings yet
- Practical - Blood Cell Counting IDocument36 pagesPractical - Blood Cell Counting Imuny67% (3)
- Cell CountDocument2 pagesCell Countapi-305259644No ratings yet
- Automated Blood Cell Counter: Project Guide: Mr. Maniraj (Associate Professor)Document13 pagesAutomated Blood Cell Counter: Project Guide: Mr. Maniraj (Associate Professor)19R25A0422 KOLLI ABHINAVA JEEVAN TEJANo ratings yet
- Cell Counting Areas in Neubauer ChamberDocument4 pagesCell Counting Areas in Neubauer Chambernice personNo ratings yet
- Cell Counting/Viability Testing: Materials: (White Labs Product Number For Reference)Document4 pagesCell Counting/Viability Testing: Materials: (White Labs Product Number For Reference)RiyanNo ratings yet
- Cell CountDocument2 pagesCell CountBridget HaleyNo ratings yet
- Extraction and Fermentation-Based Purification of Saponins From Sapindus Mukorossi GaertnDocument10 pagesExtraction and Fermentation-Based Purification of Saponins From Sapindus Mukorossi GaertnBình MinhNo ratings yet
- Cell Counting Using A HemacytometerDocument3 pagesCell Counting Using A HemacytometerKris Cahyo Mulyatno100% (1)
- 9216 - Epifluorescence Microscopic MethodDocument2 pages9216 - Epifluorescence Microscopic Methodpollux23No ratings yet
- Introduction To Media EquipmentDocument57 pagesIntroduction To Media EquipmentLaureen CordovaNo ratings yet
- Haemocytometer PPT ANIMAL CELL CULTUREDocument30 pagesHaemocytometer PPT ANIMAL CELL CULTURESarah PavuNo ratings yet
- Fossomatic 7 and Fossomatic 7 DC - Solution - Brochure - GBDocument7 pagesFossomatic 7 and Fossomatic 7 DC - Solution - Brochure - GBManoleteNo ratings yet
- Zoology Field ReportDocument11 pagesZoology Field ReportAnu Neth ThongonNo ratings yet
- Evaluation of Sysmex XN 1000 Hematology Analyzer.49Document4 pagesEvaluation of Sysmex XN 1000 Hematology Analyzer.49ivanNo ratings yet
- Microbio Lab ReportDocument3 pagesMicrobio Lab Reportroque porcelNo ratings yet
- Theory and Measurement of Bacterial GrowthDocument11 pagesTheory and Measurement of Bacterial GrowthBi Anh100% (1)