Download as pdf or txt
You might also like
- Rapid Hypnotic InductionDocument8 pagesRapid Hypnotic Inductionzev0No ratings yet
- Case Study Questionnaire For Malnourished ChildrenDocument5 pagesCase Study Questionnaire For Malnourished ChildrenSta Cruz BacnotanNo ratings yet
- How Does Hypnosis Work Ebook Uncommon KnowledgeDocument12 pagesHow Does Hypnosis Work Ebook Uncommon KnowledgeHarsh TripathiNo ratings yet
- Guidelines For The Rational Use of Blood Blood ProductsDocument120 pagesGuidelines For The Rational Use of Blood Blood ProductsHafiz Hamidi100% (1)
- Self-Hypnosis For Sleep Disturbances - OTTEpdfDocument3 pagesSelf-Hypnosis For Sleep Disturbances - OTTEpdflucasaguiar1996No ratings yet
- Etiology and Pathophysiology of InsomniaDocument12 pagesEtiology and Pathophysiology of InsomniaArif KumalaNo ratings yet
- Pato Insomnia PDFDocument14 pagesPato Insomnia PDFdilaNo ratings yet
- Treatment of InsomniaDocument11 pagesTreatment of Insomniajosif22No ratings yet
- Sleep 29 11 1398Document17 pagesSleep 29 11 1398M SNo ratings yet
- 1 s2.0 S1389945718306750 MainDocument11 pages1 s2.0 S1389945718306750 MainaybedcNo ratings yet
- E Insomni9aDocument3 pagesE Insomni9aAnni SholihahNo ratings yet
- Pre-Sleep Cognitive Intrusions AND Treatment of Onset-InsomniaDocument9 pagesPre-Sleep Cognitive Intrusions AND Treatment of Onset-Insomniajakejib775No ratings yet
- Chest 147 4 1179Document14 pagesChest 147 4 1179Albert TandyNo ratings yet
- Managing Adult Insomnia ConfidentlyDocument8 pagesManaging Adult Insomnia ConfidentlyJuliana RodriguezNo ratings yet
- The Diagnosis and Treatment of Chronic Insomnia in Adults: EditorialDocument2 pagesThe Diagnosis and Treatment of Chronic Insomnia in Adults: EditorialFiddien InderaNo ratings yet
- Sleep Disorders: Review Neurology Series Editor, William J. Mullally, MDDocument8 pagesSleep Disorders: Review Neurology Series Editor, William J. Mullally, MDniNo ratings yet
- Antenatal Self-Hypnosis For Labour and Childbirth: A Pilot StudyDocument6 pagesAntenatal Self-Hypnosis For Labour and Childbirth: A Pilot StudyRahma WatiNo ratings yet
- Practitioner's Corner: Sleeping Without A Pill: Nonpharmacologic Treatments For InsomniaDocument5 pagesPractitioner's Corner: Sleeping Without A Pill: Nonpharmacologic Treatments For InsomniaEDGAR DÍAZ URDANETANo ratings yet
- DEEP SLEEP: Unlocking the Secrets to Restorative and Rejuvenating Sleep (2023 Guide for Beginners)From EverandDEEP SLEEP: Unlocking the Secrets to Restorative and Rejuvenating Sleep (2023 Guide for Beginners)No ratings yet
- Chronic Insomnia: Matt T. Bianchi, MD, PHDDocument6 pagesChronic Insomnia: Matt T. Bianchi, MD, PHDAlex BorroelNo ratings yet
- Diagnosis and Treatment of InsomniaDocument8 pagesDiagnosis and Treatment of InsomniaPutu MulyatiNo ratings yet
- Management of Insomnia A Tailored Behavioural Approach 107 110Document4 pagesManagement of Insomnia A Tailored Behavioural Approach 107 110YogaNo ratings yet
- Insomniaprevalenceconseque PDFDocument6 pagesInsomniaprevalenceconseque PDFYumna Satyani LasiyoNo ratings yet
- Aromatherapy On InsomniaDocument8 pagesAromatherapy On InsomniaJacob KuperstokNo ratings yet
- Insomnia: A Presentation byDocument19 pagesInsomnia: A Presentation byHerlina HasibuanNo ratings yet
- Cognitive Behavior Therapy and Pharmacotherapy For Insomnia: A Randomized Controlled Trial and Direct ComparisonDocument9 pagesCognitive Behavior Therapy and Pharmacotherapy For Insomnia: A Randomized Controlled Trial and Direct ComparisonArief Rachman HakimNo ratings yet
- Treatment of Insomnia: An Alternative Approach: Anoja S. Attele, DDS, Jing-Tian Xie, MD, and Chun-Su Yuan, MD, PHDDocument11 pagesTreatment of Insomnia: An Alternative Approach: Anoja S. Attele, DDS, Jing-Tian Xie, MD, and Chun-Su Yuan, MD, PHDimamlutfi13No ratings yet
- Sleep DisordersDocument45 pagesSleep DisordersOse IbhadodeNo ratings yet
- Review InsomniaDocument17 pagesReview InsomniaIta Punya ShintaNo ratings yet
- Stepanski2003 Use of Sleep Hygiene in The Treatment of InsomniaDocument11 pagesStepanski2003 Use of Sleep Hygiene in The Treatment of InsomniaM SNo ratings yet
- The Effects of Sleep Deprivation On Pain Inhibition and Spontaneous Pain in WomanDocument12 pagesThe Effects of Sleep Deprivation On Pain Inhibition and Spontaneous Pain in Womanveigaarthur84No ratings yet
- Hypnosis 0001 PDFDocument11 pagesHypnosis 0001 PDFalanNo ratings yet
- Treatment of Primary InsomniaDocument8 pagesTreatment of Primary Insomniadanny17phNo ratings yet
- Complementary Therapies in MedicineDocument9 pagesComplementary Therapies in MedicinewilmaNo ratings yet
- Behavioral Management of HipersomniaDocument7 pagesBehavioral Management of HipersomniaHernán MarínNo ratings yet
- Nonpharmacologic Approaches To The 55Document7 pagesNonpharmacologic Approaches To The 55Hendra Pulungan100% (1)
- Aaft 14 I 1 P 33Document3 pagesAaft 14 I 1 P 33Zihan viranandaNo ratings yet
- HypnotherapyDocument6 pagesHypnotherapyAnnisa Walidatus0% (1)
- Sleep Quality and Neural Circuit Function Supporting Emotion RegulationDocument9 pagesSleep Quality and Neural Circuit Function Supporting Emotion RegulationRealidades InfinitasNo ratings yet
- Pain Coping Strategies For Tension-Type Headache: Possible Implications For Insomnia?Document5 pagesPain Coping Strategies For Tension-Type Headache: Possible Implications For Insomnia?Meilinda RosaNo ratings yet
- Comprehensive PsychiatryDocument7 pagesComprehensive PsychiatryOrangee JuceeyNo ratings yet
- TMP 624 EDocument7 pagesTMP 624 EFrontiersNo ratings yet
- Simulation 102Document41 pagesSimulation 102nidhiNo ratings yet
- Sleep DisordersDocument23 pagesSleep DisordersBEA RADANo ratings yet
- At Behavioural Approach InsomniaStudy 2011Document11 pagesAt Behavioural Approach InsomniaStudy 2011Guilherme MeirelesNo ratings yet
- Order #112566709Document5 pagesOrder #112566709Kibegwa MoriaNo ratings yet
- How Does Hypnosis WorkDocument11 pagesHow Does Hypnosis WorkchoileoNo ratings yet
- LAPMAN - 6130020049 Maulidatul Jinani FDocument22 pagesLAPMAN - 6130020049 Maulidatul Jinani FFirda JinanNo ratings yet
- 46 1 172 1 10 20160902 PDFDocument9 pages46 1 172 1 10 20160902 PDFDede FathurrahmanNo ratings yet
- Hypnosis and Cingulate-Mediated Mechanisms of AnalgesiaDocument20 pagesHypnosis and Cingulate-Mediated Mechanisms of AnalgesiaCristian GondacNo ratings yet
- Depression and Sleep Pathophysiology and TreatmentDocument11 pagesDepression and Sleep Pathophysiology and TreatmentHải ĐứcNo ratings yet
- Optimizing Behavioral Sleep StrategiesDocument7 pagesOptimizing Behavioral Sleep Strategiesdr.cidgutNo ratings yet
- A Working Model of The Neurophysiology o PDFDocument19 pagesA Working Model of The Neurophysiology o PDFOlivier BenarrocheNo ratings yet
- Sleep DisordersDocument5 pagesSleep DisorderssookoojessicaNo ratings yet
- Alvászavar És MigrénDocument10 pagesAlvászavar És MigrénLindenberger BoriszNo ratings yet
- Insomnio CronicoDocument17 pagesInsomnio CronicoDra Carolina Escalante Neurologa de AdultosNo ratings yet
- Insomnia ReviewDocument5 pagesInsomnia ReviewMartini ListrikNo ratings yet
- HUL261: Introduction To Psychology: Altered State of ConsciousnessDocument6 pagesHUL261: Introduction To Psychology: Altered State of ConsciousnessEkant YadavNo ratings yet
- HypnotherapyDocument2 pagesHypnotherapySamiha DuzaNo ratings yet
- Sleep Disturbance and Nonmalignant Chronic PainDocument17 pagesSleep Disturbance and Nonmalignant Chronic Painveigaarthur84No ratings yet
- Treating Comorbid Insomnia in Older Adults Via Cognitive-Behavioural Treatment, Bright Light and ExerciseDocument9 pagesTreating Comorbid Insomnia in Older Adults Via Cognitive-Behavioural Treatment, Bright Light and ExerciseFiddien InderaNo ratings yet
- Physical Anthropology Forensic Psychiatry Tests On Primates and Placebo Effect 14112022 111557pmDocument9 pagesPhysical Anthropology Forensic Psychiatry Tests On Primates and Placebo Effect 14112022 111557pmMaryam Talha SandhuNo ratings yet
- Menopause: Hormones, Lifestyle, and Optimizing AgingDocument15 pagesMenopause: Hormones, Lifestyle, and Optimizing Agingsetya riniNo ratings yet
- Menopause 1 Bu MaeDocument7 pagesMenopause 1 Bu Maesetya riniNo ratings yet
- Laporan PKM September 2021Document5 pagesLaporan PKM September 2021setya riniNo ratings yet
- d3 Kebidanan MetroDocument1 paged3 Kebidanan Metrosetya riniNo ratings yet
- Suicide in Children and Adolescents Cambridge Child and Adolescent PsychiatryDocument333 pagesSuicide in Children and Adolescents Cambridge Child and Adolescent PsychiatryFlorin Tudose100% (1)
- Hashimoto's Triggers-Advanced Reader Copy-V2Document332 pagesHashimoto's Triggers-Advanced Reader Copy-V2Anonymous XiymFuQdF100% (2)
- Las-Peh q1 Week1Document4 pagesLas-Peh q1 Week1Lemuel Dave AzañaNo ratings yet
- Cagayan State University-Carig Campus: College of Medicine and SurgeryDocument11 pagesCagayan State University-Carig Campus: College of Medicine and SurgeryRich MarkNo ratings yet
- Bordetella PertussisDocument8 pagesBordetella PertussisDANIELLA LOMA CAPONPONNo ratings yet
- Cervical Incompetence: Diagnostic TestsDocument2 pagesCervical Incompetence: Diagnostic TestsCHRISTIAN CALAMBANo ratings yet
- JHA Construction of Drain and SumpDocument6 pagesJHA Construction of Drain and SumpSamsiah TolaNo ratings yet
- SAGES Consent 2019 2023Document16 pagesSAGES Consent 2019 2023cNo ratings yet
- Safety Seal Presentation For DepEdDocument11 pagesSafety Seal Presentation For DepEdjoy sotoNo ratings yet
- Acute Coronary Syndrome - PatientDocument4 pagesAcute Coronary Syndrome - Patientaasuman123No ratings yet
- Pathophysiology of Breast CancerDocument3 pagesPathophysiology of Breast Cancerpauline mangadaNo ratings yet
- Pediatric Trauma Life Support 3e Update 2017 FINALDocument21 pagesPediatric Trauma Life Support 3e Update 2017 FINALAnita MacdanielNo ratings yet
- Allied Health ProfessionDocument51 pagesAllied Health ProfessionLovelyn Calaramo BelloNo ratings yet
- GP Maternal NICE Final 1Document1 pageGP Maternal NICE Final 1Guillermo CalderaroNo ratings yet
- Composite Vs Amalgam PowerpointDocument17 pagesComposite Vs Amalgam Powerpointapi-322463366100% (1)
- Wiac - Info PDF 771 Advances in Dga Interpretation PRDocument77 pagesWiac - Info PDF 771 Advances in Dga Interpretation PRChemist Ahmed FoudaNo ratings yet
- HSG PresentationDocument18 pagesHSG Presentationashikin92No ratings yet
- 2020 Status Report As of August 31, 2021Document192 pages2020 Status Report As of August 31, 2021Jasper Kenneth PeraltaNo ratings yet
- Nursing Care Plan For Insufficient Breast Milk ProductionDocument4 pagesNursing Care Plan For Insufficient Breast Milk ProductionHina FatimaNo ratings yet
- IAF MD 8 2011 Application of ISO 17011 in MDQMS (ISO 13485) Issue 1 2011Document17 pagesIAF MD 8 2011 Application of ISO 17011 in MDQMS (ISO 13485) Issue 1 2011carlosprieto36No ratings yet
- Malady List - Mms Wiki - Jim Humble - Genesis II Church - Mmswiki IsDocument8 pagesMalady List - Mms Wiki - Jim Humble - Genesis II Church - Mmswiki Isapi-301431920No ratings yet
- Local Anesthesia in Dental HygieneDocument5 pagesLocal Anesthesia in Dental Hygieneapi-702868085No ratings yet
- Unit 2Document45 pagesUnit 2Dsce BtNo ratings yet
- OBDocument4 pagesOBCharlie Cotoner FalgueraNo ratings yet
- Module 6 - Philippine E-Health Strategic Plan (PeHSP) and Philippine Health Information Exchange (PHIE)Document19 pagesModule 6 - Philippine E-Health Strategic Plan (PeHSP) and Philippine Health Information Exchange (PHIE)Zuriel San PedroNo ratings yet
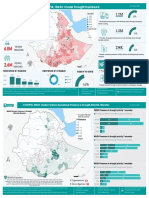
- 2023 WASH Cluster Drought Product JuneDocument2 pages2023 WASH Cluster Drought Product JuneResilient GemeNo ratings yet
- Counselling On BFDocument7 pagesCounselling On BFAndrea Díaz RodríguezNo ratings yet
- D.S.S Aiims Prepration Test Series DR - SANJAY 7014964651Document7 pagesD.S.S Aiims Prepration Test Series DR - SANJAY 7014964651Dr-Sanjay SinghaniaNo ratings yet