Download as xlsx, pdf, or txt
You might also like
- A Folklore Bestiary (High-Res) (OSE)Document160 pagesA Folklore Bestiary (High-Res) (OSE)Digs31100% (2)
- Revised Incident Record FormDocument2 pagesRevised Incident Record FormRafael Juico100% (4)
- Edpm SbaDocument1 pageEdpm SbaDuhguy Marvin Charles60% (5)
- Chapter Ten Historical Development of Human RightsDocument11 pagesChapter Ten Historical Development of Human Rightslm100% (1)
- Incident Report FormDocument2 pagesIncident Report FormBryan Cesar V. Asiatico100% (1)
- Session 2 - Benihana - StudentsDocument18 pagesSession 2 - Benihana - StudentsRonex OnnetNo ratings yet
- Preventive Maintenance and Inspection ProceduresDocument13 pagesPreventive Maintenance and Inspection ProceduresOsagie AlfredNo ratings yet
- Freemasonry and The TarotDocument37 pagesFreemasonry and The TarotΔημητρης Ιατριδης0% (1)
- QP-2040 Box Ways Machining CenterDocument11 pagesQP-2040 Box Ways Machining CenterSergio LopezNo ratings yet
- AIF Guide June 2019Document33 pagesAIF Guide June 2019Harsh ChhabraNo ratings yet
- Annex 2i Investigation Form 29092020Document6 pagesAnnex 2i Investigation Form 29092020nik mohamad zulfikriNo ratings yet
- Cdi 21 Final ReqDocument18 pagesCdi 21 Final ReqJehu FerrarenNo ratings yet
- Passport Form 2Document3 pagesPassport Form 2Philip PinesNo ratings yet
- Group4 Case Folder Robbery With ArsonDocument20 pagesGroup4 Case Folder Robbery With ArsonGian Verga100% (1)
- Azara Application FormDocument6 pagesAzara Application FormKristijan PolicNo ratings yet
- Incident Record FormDocument3 pagesIncident Record FormIronman SpongebobNo ratings yet
- D StatmentDocument8 pagesD StatmentHihiNo ratings yet
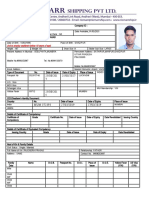
- Ship Management Pvt. LTD.: Application Form / Personal Data Update FormDocument5 pagesShip Management Pvt. LTD.: Application Form / Personal Data Update FormViorel StanNo ratings yet
- BI FORM (Latest As of June 13, 2010)Document6 pagesBI FORM (Latest As of June 13, 2010)PAPARUSANo ratings yet
- Las Piñas CIFDocument1 pageLas Piñas CIFchrisNo ratings yet
- City Epidemilogy Surveillance Unit: Delta Variant ReportDocument8 pagesCity Epidemilogy Surveillance Unit: Delta Variant ReportKathy OrtizNo ratings yet
- Tylers House ApplicationDocument4 pagesTylers House Applicationapi-351805649No ratings yet
- Arrival Card in PH 1Document2 pagesArrival Card in PH 1gleric custodioNo ratings yet
- DOH PIDSR COVID-19 CIF TemplateDocument1 pageDOH PIDSR COVID-19 CIF TemplateMargaux Faith CCNo ratings yet
- F3 Malaria In-Patient Registry FormDocument1 pageF3 Malaria In-Patient Registry FormJumar CarpeNo ratings yet
- Application For Resident Guest Scheme of Sri Lanka: Single Married Widowed Divorced SeparatedDocument6 pagesApplication For Resident Guest Scheme of Sri Lanka: Single Married Widowed Divorced Separateda769No ratings yet
- No. Date Area Emp No.: 1 11/112/2021 Caraga East 16769Document29 pagesNo. Date Area Emp No.: 1 11/112/2021 Caraga East 16769jay-ann dahunogNo ratings yet
- Renewal Application Adult01Document2 pagesRenewal Application Adult01scribideeNo ratings yet
- 2021112163Document3 pages2021112163Niranjan UniqueNo ratings yet
- Application Form: Professional Regulation CommissionDocument1 pageApplication Form: Professional Regulation Commissionhector anonuevoNo ratings yet
- Fit 2 Work Form 2013 - 2Document5 pagesFit 2 Work Form 2013 - 2suneerav174633No ratings yet
- District State: Note: For NMR Entry Highest Education Qualification (Up To Class X Only)Document2 pagesDistrict State: Note: For NMR Entry Highest Education Qualification (Up To Class X Only)Anonymous ovq7UE2WzNo ratings yet
- Coronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalDocument1 pageCoronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalKarsenley Cal-el Iddig BurigsayNo ratings yet
- 1.officers Application Form RiomarrDocument5 pages1.officers Application Form RiomarrÁřvíňď PřášáďNo ratings yet
- Application Form: Professional Regulation CommissionDocument1 pageApplication Form: Professional Regulation CommissionKurt HendiveNo ratings yet
- Passport Application Form ENGDocument3 pagesPassport Application Form ENGEtuate CockerNo ratings yet
- Renewal Regular Passport Application Form (Adult) : Department of Foreign AffairsDocument2 pagesRenewal Regular Passport Application Form (Adult) : Department of Foreign AffairsMary JoyNo ratings yet
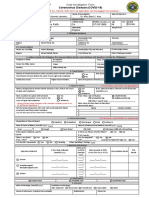
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormMizraim TupazNo ratings yet
- Psi Blank DocumentDocument6 pagesPsi Blank Documentapi-266547891No ratings yet
- Cs Form 100 Rev Nov 2012Document2 pagesCs Form 100 Rev Nov 2012Amanda PattersonNo ratings yet
- Cs Form 100 Rev 2012Document2 pagesCs Form 100 Rev 2012AnnNo ratings yet
- Notification DMHO West Godavari Staff Nurse Lab Technician Other PostsDocument3 pagesNotification DMHO West Godavari Staff Nurse Lab Technician Other PostsrajaNo ratings yet
- Registraion Form Arrival Date: Dd-Mm-Yyyy Departure Date: Dd-Mm-YyyyDocument1 pageRegistraion Form Arrival Date: Dd-Mm-Yyyy Departure Date: Dd-Mm-YyyySmart WorkNo ratings yet
- Frustrated Homicide - Serious Physical Injury - Murder - Rape - Attempted Rape - Acts of Lasciviousness - Possible Law Violated: - Other IncidentDocument3 pagesFrustrated Homicide - Serious Physical Injury - Murder - Rape - Attempted Rape - Acts of Lasciviousness - Possible Law Violated: - Other IncidentRoel Angelu C. TelbaNo ratings yet
- Registration Card Sample 5Document1 pageRegistration Card Sample 5Nina OaipNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormShiela E. EladNo ratings yet
- I-589 CompletoDocument12 pagesI-589 CompletoGrenNe FuenBarNo ratings yet
- Philippine Embassy, Rome: Appointment Verification: RemarksDocument2 pagesPhilippine Embassy, Rome: Appointment Verification: RemarksNick DimaanoNo ratings yet
- F1 Malaria Patient Registry FormDocument1 pageF1 Malaria Patient Registry FormCha Tuban DianaNo ratings yet
- Gil Sanchez, Labason Zamboanga Del Norte: AmacaDocument2 pagesGil Sanchez, Labason Zamboanga Del Norte: AmacaMacky BirdNo ratings yet
- Post EnconterDocument2 pagesPost Enconterjoeceltorres48No ratings yet
- Hiring Application FormDocument6 pagesHiring Application FormAnonymous QHfIVes9r100% (1)
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormPresinto Dos Parañaque KnightsNo ratings yet
- New Regular Passport Application (Adult)Document2 pagesNew Regular Passport Application (Adult)Cherrie Mae ReyesNo ratings yet
- Case FolderDocument27 pagesCase FolderMa. Dolores JoaquinNo ratings yet
- New Regular Passport Application (Adult) : Form No. 1-ENGLISHDocument2 pagesNew Regular Passport Application (Adult) : Form No. 1-ENGLISHJaira EbronNo ratings yet
- Renewal Regular Passport Application Form (Adult) : Department of Foreign AffairsDocument2 pagesRenewal Regular Passport Application Form (Adult) : Department of Foreign AffairsTahinay KarlNo ratings yet
- Important RemindersDocument3 pagesImportant RemindersAizaNo ratings yet
- Passport Application Adult RenewalDocument2 pagesPassport Application Adult RenewalGarcia efrilNo ratings yet
- Renewal Regular Passport Application Form (Adult) : Department of Foreign AffairsDocument2 pagesRenewal Regular Passport Application Form (Adult) : Department of Foreign Affairsmartie avancenaNo ratings yet
- Renewal Regular Passport Application Form (Adult) : Department of Foreign AffairsDocument2 pagesRenewal Regular Passport Application Form (Adult) : Department of Foreign Affairsmartie avancenaNo ratings yet
- Item "A" - Reporting Person: Philippine National PoliceDocument5 pagesItem "A" - Reporting Person: Philippine National PoliceRomnese SantiagoNo ratings yet
- Personal Data Sheet: Beboso Ernest JOY QuijanoDocument10 pagesPersonal Data Sheet: Beboso Ernest JOY QuijanoErgo WingsNo ratings yet
- Item "A" - Reporting Person: Philippine National PoliceDocument5 pagesItem "A" - Reporting Person: Philippine National PoliceRomnese SantiagoNo ratings yet
- Eppt App Form2 Renewal For AdultDocument2 pagesEppt App Form2 Renewal For Adultdan maliwat100% (1)
- 2012 Renewal FormDocument2 pages2012 Renewal FormDanhil Ramos100% (1)
- The Psychology of False Confessions: Forty Years of Science and PracticeFrom EverandThe Psychology of False Confessions: Forty Years of Science and PracticeNo ratings yet
- EasyNotes 20240116 080857 096Document2 pagesEasyNotes 20240116 080857 096lmNo ratings yet
- I NtercomDocument1 pageI NtercomlmNo ratings yet
- New 3Document4 pagesNew 3lmNo ratings yet
- NEW2Document3 pagesNEW2lmNo ratings yet
- Modern Political Thought PDF FinalDocument42 pagesModern Political Thought PDF FinallmNo ratings yet
- Chapter Three Medieval Political Thought 2020Document21 pagesChapter Three Medieval Political Thought 2020lmNo ratings yet
- Kisii University Business Mathematics II: Course Title: Course Code: BBAM 171Document2 pagesKisii University Business Mathematics II: Course Title: Course Code: BBAM 171lmNo ratings yet
- Bbam 170 Topic 1Document16 pagesBbam 170 Topic 1lmNo ratings yet
- Chapter 5Document2 pagesChapter 5Paul JonesNo ratings yet
- Transgressions and IniquityDocument22 pagesTransgressions and IniquitySishaj P SimonNo ratings yet
- FA2Document77 pagesFA2shahreen arshad0% (1)
- Practical Design To Eurocode 2 - Lecture 1 Intro and BackgroundDocument39 pagesPractical Design To Eurocode 2 - Lecture 1 Intro and Background이동욱No ratings yet
- Pay Slip: Institute of Liver and Biliary SciencesDocument1 pagePay Slip: Institute of Liver and Biliary SciencesAbhimanyu SahaabNo ratings yet
- MUET (Reading)Document18 pagesMUET (Reading)Zuraida YusoffNo ratings yet
- Cybercrime Awarenessand Perceptionamong Studentsof Saint Michael Collegeof CaragaDocument11 pagesCybercrime Awarenessand Perceptionamong Studentsof Saint Michael Collegeof CaragaRonel DayoNo ratings yet
- Please Note: Fields Marked With: (Red Asterisk) Are Mandatory Fields and Need To Be Filled UpDocument20 pagesPlease Note: Fields Marked With: (Red Asterisk) Are Mandatory Fields and Need To Be Filled UpHinglaj SinghNo ratings yet
- Southworth v. OliverDocument2 pagesSouthworth v. OlivercrlstinaaaNo ratings yet
- Kick Off Meeting BPI 2020Document70 pagesKick Off Meeting BPI 2020Stella AngelicaNo ratings yet
- Powering The World: With Ge'S Solutions For Nuclear Turbine IslandsDocument24 pagesPowering The World: With Ge'S Solutions For Nuclear Turbine IslandsShanon RustoffNo ratings yet
- Mississippi Innocence Project and Innocence Project Client Eddie Lee Howard PDFDocument2 pagesMississippi Innocence Project and Innocence Project Client Eddie Lee Howard PDFWLBT NewsNo ratings yet
- Subodh KhareDocument10 pagesSubodh Kharepragmatic.desiNo ratings yet
- Luxury Wine Case StudyDocument14 pagesLuxury Wine Case Studyapi-308966986No ratings yet
- Case 4Document4 pagesCase 4Zhenyi ZhuNo ratings yet
- 5 Lessons That Jacob's Night of Wrestling Teaches Us About PrayerDocument2 pages5 Lessons That Jacob's Night of Wrestling Teaches Us About PrayerJosephine Chirwa100% (1)
- Acdasoa On The Spot Logo Making Contest GuidelinesDocument2 pagesAcdasoa On The Spot Logo Making Contest GuidelinesAlma Reynaldo TucayNo ratings yet
- Emergency Motion Darrell VolentineDocument12 pagesEmergency Motion Darrell VolentinesmallcapsmarketNo ratings yet
- Vi-Complete The ConversationDocument3 pagesVi-Complete The ConversationjoseNo ratings yet
- J. Robert OppenheimerDocument3 pagesJ. Robert OppenheimerKath DeguzmanNo ratings yet
- Shantanu Agnihotri - HistoryDocument31 pagesShantanu Agnihotri - HistoryShantanu AgnihotriNo ratings yet
- 6 Volunteer ManagementDocument12 pages6 Volunteer ManagementHafedh Ben MiledNo ratings yet
- Macalintal vs. COMELECDocument1 pageMacalintal vs. COMELECRTC OCCNo ratings yet