Download as docx, pdf, or txt
You might also like
- Postoperative Nursing Care Plan For Cesarian Section Patient Case Pres-ORDocument6 pagesPostoperative Nursing Care Plan For Cesarian Section Patient Case Pres-ORMae Azores93% (99)
- NCP - Impaired Skin IntegrityDocument3 pagesNCP - Impaired Skin IntegrityFlauros Ryu Jabien90% (30)
- Case Study StacDocument2 pagesCase Study StacJanelle Cabida Supnad0% (1)
- NCM 118 Ed Lecture Learning Material 1: College of NursingDocument20 pagesNCM 118 Ed Lecture Learning Material 1: College of NursingJanelle Cabida SupnadNo ratings yet
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- Introduction To GlobalizationDocument35 pagesIntroduction To GlobalizationJanelle Cabida SupnadNo ratings yet
- Nursing Care Plan Impaired CommunicationDocument3 pagesNursing Care Plan Impaired CommunicationRamiel ChristopherNo ratings yet
- Copy of NCP Format)Document4 pagesCopy of NCP Format)shai raNo ratings yet
- 3 Ncp'sDocument3 pages3 Ncp'sJohn Michael EstevesNo ratings yet
- Clinical Portrait Pertinent DataDocument9 pagesClinical Portrait Pertinent DataGermin CesaNo ratings yet
- Drug Study Threatened AbortionDocument4 pagesDrug Study Threatened AbortionKath CastilloNo ratings yet
- NCP AlteredDocument3 pagesNCP AlteredShaira TillahNo ratings yet
- Ms. Ann Female 48 Years Old Diabetes Mellitus Foot/diabetes Mellitus Joseph MDocument10 pagesMs. Ann Female 48 Years Old Diabetes Mellitus Foot/diabetes Mellitus Joseph MFielMendozaNo ratings yet
- Nursing Care Plan Acute Pain (Surgery AMB Incision)Document3 pagesNursing Care Plan Acute Pain (Surgery AMB Incision)deric100% (23)
- NCP TemplateDocument3 pagesNCP TemplateJUNNEL JAMES A. CALATRAVANo ratings yet
- JournalDocument15 pagesJournalRodolfo CampoNo ratings yet
- Jose Abad NCP 2Document2 pagesJose Abad NCP 2bryan.zabala.mnlNo ratings yet
- UntitledDocument4 pagesUntitledAnnika Ysabelle S. LedesmaNo ratings yet
- Nursing Care Plan: Third Rotation: Metro Vigan Hospital-WardDocument5 pagesNursing Care Plan: Third Rotation: Metro Vigan Hospital-WardKrizha Angela NicolasNo ratings yet
- NCP CnsDocument3 pagesNCP Cnsandrea salesNo ratings yet
- Risk For Fall (Zika Virus)Document10 pagesRisk For Fall (Zika Virus)Fhey Bernadette BeltranNo ratings yet
- NCP HypertensionDocument7 pagesNCP HypertensionMARY ROSE DOLOGUINNo ratings yet
- Risk For Ineffective Airway Clearance 1Document8 pagesRisk For Ineffective Airway Clearance 1kint manlangitNo ratings yet
- NCPDocument1 pageNCPSherry Ann FayeNo ratings yet
- (NCPS) Impaired Physical Mobility 2Document2 pages(NCPS) Impaired Physical Mobility 2roren100% (1)
- Concepcion NCPDocument2 pagesConcepcion NCPLevi ConcepcionNo ratings yet
- 2 NCP CvaDocument5 pages2 NCP CvaLord Allen B. GomezNo ratings yet
- FUNDA RLE-ACTIVITYDocument3 pagesFUNDA RLE-ACTIVITYElaisha Mae C. CarsulaNo ratings yet
- Agn NCPDocument6 pagesAgn NCPJewel AnneNo ratings yet
- Nursing Care Plan For HemorrhoidsDocument3 pagesNursing Care Plan For HemorrhoidsFaith Marfil100% (2)
- Intussuception Is A Condition in Which Part of The Intestine Folds Into The Section Next To ItDocument3 pagesIntussuception Is A Condition in Which Part of The Intestine Folds Into The Section Next To ItEduard GarchitorenaNo ratings yet
- NCP Stab Wound (Artillo)Document7 pagesNCP Stab Wound (Artillo)Al TheóNo ratings yet
- Jen NCPICUDocument3 pagesJen NCPICUJennifer AlamonNo ratings yet
- Safran, Jayrelle Aldrin Shayne D. - Act # 4finals (8th Rotation)Document5 pagesSafran, Jayrelle Aldrin Shayne D. - Act # 4finals (8th Rotation)Jayrelle D. SafranNo ratings yet
- Nursing Care Plan Cues Nursing DX. Analysis Goals & Objectives Nsg. Intervention Rationale EvaluationDocument2 pagesNursing Care Plan Cues Nursing DX. Analysis Goals & Objectives Nsg. Intervention Rationale EvaluationkerbyannmNo ratings yet
- NCP AppendicitisDocument2 pagesNCP Appendicitismnms0708100% (2)
- Head and Neck NCPDocument2 pagesHead and Neck NCPAngelo AbiganiaNo ratings yet
- 000print or NCPDocument6 pages000print or NCPAngie MandeoyaNo ratings yet
- NCP GeriaDocument2 pagesNCP GeriaEitan LopezNo ratings yet
- Giman NCPDocument3 pagesGiman NCPJoedelynne Diane Endaya GarciaNo ratings yet
- Fundalec 2Document1 pageFundalec 2bienne carpioNo ratings yet
- Nursing Care Plan: Phinma University of IloiloDocument1 pageNursing Care Plan: Phinma University of IloiloArianne Nicole PinuelaNo ratings yet
- PainDocument1 pagePainbienne carpioNo ratings yet
- Disturbed Visual Sensory Perception Related: Nursing Care PlanDocument3 pagesDisturbed Visual Sensory Perception Related: Nursing Care PlanMae Therese B. MAGNONo ratings yet
- Cues Nursing Diagnosi S Analysis Goal Intervention Rationale EvaluationDocument3 pagesCues Nursing Diagnosi S Analysis Goal Intervention Rationale EvaluationKae MacalinaoNo ratings yet
- NCP Villahermosa CTSDocument6 pagesNCP Villahermosa CTSJv Jore VillahermosaNo ratings yet
- Spina Bifida NCPDocument3 pagesSpina Bifida NCPShahzad GulfamNo ratings yet
- PseudoDocument6 pagesPseudoJessa Mhae AvelinoNo ratings yet
- Assessment Diagnosis Rationale Planning Implementation Rationale Evaluation Subjective Data Short-Term: Independent Short-TermDocument2 pagesAssessment Diagnosis Rationale Planning Implementation Rationale Evaluation Subjective Data Short-Term: Independent Short-TermDiane Krystel G. MoralesNo ratings yet
- Actual Problem: Assessment Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Short-Term ObjectivesDocument3 pagesActual Problem: Assessment Explanation of The Problem Planning Intervention Rationale Evaluation Subjective: Short-Term ObjectivesSherilyn BarbozaNo ratings yet
- Nursing-Care-Plan-J P VDocument8 pagesNursing-Care-Plan-J P VMa. Ferimi Gleam BajadoNo ratings yet
- NCP Post Op (Impaired and Risk For Infection)Document4 pagesNCP Post Op (Impaired and Risk For Infection)Carl J.No ratings yet
- Nursing Care Plan DX: Risk For Fall Related To Loss of Skeletal Integrity (Fractures) /movement of BoneDocument4 pagesNursing Care Plan DX: Risk For Fall Related To Loss of Skeletal Integrity (Fractures) /movement of BoneYosef OxinioNo ratings yet
- 9 Fracture Nursing Care Plans: PathophysiologyDocument15 pages9 Fracture Nursing Care Plans: PathophysiologyMaryrose RamirezNo ratings yet
- Updated NCPrisk For InjuryDocument1 pageUpdated NCPrisk For InjuryChucky VergaraNo ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Vascular Surgery, Neurosurgery, Lower Extremity Ulcers, Antimicrobials, Wound Assessment, Care, Measurement and RepairFrom EverandVascular Surgery, Neurosurgery, Lower Extremity Ulcers, Antimicrobials, Wound Assessment, Care, Measurement and RepairNo ratings yet
- Fractures of the Wrist: A Clinical CasebookFrom EverandFractures of the Wrist: A Clinical CasebookNirmal C. TejwaniNo ratings yet
- First Aid & Emergency Companions: First Aid & Emergencies at SeaFrom EverandFirst Aid & Emergency Companions: First Aid & Emergencies at SeaNo ratings yet
- Alien Hand Syndrome, (Dr Strangelove Syndrome) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAlien Hand Syndrome, (Dr Strangelove Syndrome) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- UNP-CN Do Not Reproduce: Learning Pocket DescriptionDocument37 pagesUNP-CN Do Not Reproduce: Learning Pocket DescriptionJanelle Cabida SupnadNo ratings yet
- Physiologic Function and Appearance of The NewbornDocument5 pagesPhysiologic Function and Appearance of The NewbornJanelle Cabida SupnadNo ratings yet
- NPI and Health TeachingDocument4 pagesNPI and Health TeachingJanelle Cabida SupnadNo ratings yet
- Upon Admission (15 PTS) in The Intensive Care Unit (15 PTS) : ? (5 Pts Each Parameter A Total of 15 Points)Document5 pagesUpon Admission (15 PTS) in The Intensive Care Unit (15 PTS) : ? (5 Pts Each Parameter A Total of 15 Points)Janelle Cabida SupnadNo ratings yet
- University of Northern PhilippinesDocument7 pagesUniversity of Northern PhilippinesJanelle Cabida SupnadNo ratings yet
- Asepsis: (You Can Use The Back of This Paper or Other Paper)Document12 pagesAsepsis: (You Can Use The Back of This Paper or Other Paper)Janelle Cabida SupnadNo ratings yet
- Nursing Care Management 109 (Skills) Medication: Drug Type Description ExamplesDocument9 pagesNursing Care Management 109 (Skills) Medication: Drug Type Description ExamplesJanelle Cabida SupnadNo ratings yet
- Chapter 2 (Computer Hardware)Document69 pagesChapter 2 (Computer Hardware)Janelle Cabida SupnadNo ratings yet
- NCM 101: Care of The Mother, Child and FAMILY (Pedia Part) NCM 101: Care of The Mother, Child and FAMILY (Pedia Part)Document38 pagesNCM 101: Care of The Mother, Child and FAMILY (Pedia Part) NCM 101: Care of The Mother, Child and FAMILY (Pedia Part)Janelle Cabida SupnadNo ratings yet
- Basic Nutrition and Diet TherapyDocument108 pagesBasic Nutrition and Diet TherapyJanelle Cabida SupnadNo ratings yet
- Chapter 4 (Computer Software)Document33 pagesChapter 4 (Computer Software)Janelle Cabida SupnadNo ratings yet
- Chapter 3Document65 pagesChapter 3Janelle Cabida SupnadNo ratings yet
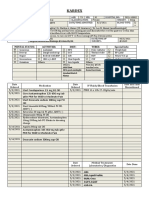
- Kardex: Mental Status: Activities: Diet: Tubes: Special InfoDocument3 pagesKardex: Mental Status: Activities: Diet: Tubes: Special InfoJanelle Cabida SupnadNo ratings yet
- Chapter 1 (Historical Perspective of Nursing Informatics)Document49 pagesChapter 1 (Historical Perspective of Nursing Informatics)Janelle Cabida SupnadNo ratings yet
- Ni TelehealthDocument3 pagesNi TelehealthJanelle Cabida SupnadNo ratings yet
- Care of The Woman With Complications During LaborDocument20 pagesCare of The Woman With Complications During LaborJanelle Cabida SupnadNo ratings yet
- FORM 08.1 Medication Card TemplateDocument5 pagesFORM 08.1 Medication Card TemplateJanelle Cabida SupnadNo ratings yet
- Spinal Cord Injury: Cedric Muceros BSN 3CDocument4 pagesSpinal Cord Injury: Cedric Muceros BSN 3CJanelle Cabida SupnadNo ratings yet
- Debakey Forceps Are A Type of Atraumatic Tissue ForcepsDocument3 pagesDebakey Forceps Are A Type of Atraumatic Tissue ForcepsJanelle Cabida SupnadNo ratings yet
- Factors in The Relationship Between Epilepsy and Behavioral DisordersDocument19 pagesFactors in The Relationship Between Epilepsy and Behavioral DisordersEdya YopiNo ratings yet
- Medical Surgical Nursing ReviewDocument97 pagesMedical Surgical Nursing ReviewBernadeth Josefa BorelaNo ratings yet
- VertigoDocument37 pagesVertigoDevi AswandiNo ratings yet
- Dizziness and VertigoDocument32 pagesDizziness and Vertigoabdisalaan hassanNo ratings yet
- Complex Regional Pain SyndromeDocument24 pagesComplex Regional Pain SyndromeJanine RustNo ratings yet
- BeraDocument20 pagesBeraMuhamad SyaifulNo ratings yet
- Autism and Abnormalities in The BrainDocument9 pagesAutism and Abnormalities in The BrainAlan Challoner100% (1)
- Case English 2 - Atypical Absence SeizureDocument25 pagesCase English 2 - Atypical Absence SeizuresyongebobNo ratings yet
- T01 Introduction To Disabilities (12.07.2021)Document4 pagesT01 Introduction To Disabilities (12.07.2021)suraj singhNo ratings yet
- 3 RD Year BSC NursingDocument67 pages3 RD Year BSC NursingSURAJ2792100% (1)
- Rehabilitacion PlasticidadDocument9 pagesRehabilitacion Plasticidadn_almagroNo ratings yet
- Case #1: Current Visit: 23 Year Old Man Returns For Follow Up Having Been Last Seen Six Months Ago. He Reports No ChangeDocument11 pagesCase #1: Current Visit: 23 Year Old Man Returns For Follow Up Having Been Last Seen Six Months Ago. He Reports No ChangeRehan SaleemNo ratings yet
- FunctionalDocument82 pagesFunctionalaydhoooNo ratings yet
- Medical SpecialistDocument9 pagesMedical SpecialistDhiya MaralinNo ratings yet
- Nerve Muscle PhysioDocument30 pagesNerve Muscle Physiopatel_hanisha06No ratings yet
- Daftar Pasien Neurologi RABU 22 APRIL 2020: Lontara 3 Saraf Kamar 1Document4 pagesDaftar Pasien Neurologi RABU 22 APRIL 2020: Lontara 3 Saraf Kamar 1Ilham Habib DjarkoniNo ratings yet
- Week 9.1Document41 pagesWeek 9.1firefaerieNo ratings yet
- Then and Now: Chemistry & Society: Chronic Traumatic EncephalopathyDocument4 pagesThen and Now: Chemistry & Society: Chronic Traumatic Encephalopathyapi-269382043No ratings yet
- Cerebrovascular Disease BleedDocument2 pagesCerebrovascular Disease BleedJogyBoyLunaNo ratings yet
- Pysche OSCE - EPSE ExaminationDocument1 pagePysche OSCE - EPSE ExaminationAmber WangNo ratings yet
- Muscular SystemmDocument2 pagesMuscular SystemmPearl PearlNo ratings yet
- ENT BCQsDocument19 pagesENT BCQsSajid AliNo ratings yet
- Question-Bank: Round-1 Non-Passing Round Instructions For RoundDocument17 pagesQuestion-Bank: Round-1 Non-Passing Round Instructions For RoundBhawna PandhuNo ratings yet
- Neurosky TechnologyDocument23 pagesNeurosky TechnologyTejasriVarma100% (2)
- 7th Cranial Nerve PalsyDocument7 pages7th Cranial Nerve PalsySundarajan Mani100% (1)
- Shamol CT ScanDocument197 pagesShamol CT ScannaimNo ratings yet
- Scientific Events Distribution PDFDocument9 pagesScientific Events Distribution PDFCodrin FodorNo ratings yet
- Neuro QuizDocument16 pagesNeuro QuizarzeManzanoNo ratings yet
- Atypical Parkinsonian Disorders PDFDocument515 pagesAtypical Parkinsonian Disorders PDFskyclad_21100% (3)
- Pathophysiology of Tinnitus and Evidence-Based Options For Tinnitus ManagementDocument12 pagesPathophysiology of Tinnitus and Evidence-Based Options For Tinnitus ManagementEli HuertaNo ratings yet