Download as pdf or txt
You might also like
- TGD 13Document3 pagesTGD 13Latanya JenkinsNo ratings yet
- Organisational Behaviour Understanding People in Healthcare OrganisationsDocument17 pagesOrganisational Behaviour Understanding People in Healthcare OrganisationsJehan L.No ratings yet
- Jurnal Kbs 2Document24 pagesJurnal Kbs 2Dee SariNo ratings yet
- Strategic ConvergenceDocument42 pagesStrategic ConvergencerajneeshchowdhuryNo ratings yet
- Modul 04 MK Ars 201 Hospitall Entrepreuneurship LeadershipDocument14 pagesModul 04 MK Ars 201 Hospitall Entrepreuneurship Leadershipenik utmawatiNo ratings yet
- Leadership and Management in HealthcareDocument4 pagesLeadership and Management in HealthcareMuhamad FirdausNo ratings yet
- Healthcare Physicians As Practice Administrators: Running Head: RESEARCH PAPER 1Document7 pagesHealthcare Physicians As Practice Administrators: Running Head: RESEARCH PAPER 1iqraNo ratings yet
- Power, Leadership and TransformationDocument10 pagesPower, Leadership and TransformationJonathanPantaleonNo ratings yet
- Clinical LeadershipDocument16 pagesClinical LeadershipShiller MaroufzadehNo ratings yet
- Managerial Control Vs Professional AutonomyDocument9 pagesManagerial Control Vs Professional AutonomyDoğan Nadi LeblebiciNo ratings yet
- The Clinical Teacher - 2011 - Swanwick - What Is Clinical Leadership and Why Is It ImportantDocument5 pagesThe Clinical Teacher - 2011 - Swanwick - What Is Clinical Leadership and Why Is It Importantslahri7No ratings yet
- Sample 2 DissertationDocument49 pagesSample 2 DissertationTutors SectionNo ratings yet
- Sample 2 DissertationDocument49 pagesSample 2 DissertationTutors SectionNo ratings yet
- Jones and Fulop (2021)Document8 pagesJones and Fulop (2021)Khoulita CherifNo ratings yet
- Transformative Leadership Training in Medical Education A TopologyDocument9 pagesTransformative Leadership Training in Medical Education A Topologyslahri7No ratings yet
- Creating+Order+Out+of+Chaos+ +a+Leadership+Approach+ +2010 +2010 +2010 +2010 +2010Document18 pagesCreating+Order+Out+of+Chaos+ +a+Leadership+Approach+ +2010 +2010 +2010 +2010 +2010Anita FaúndezNo ratings yet
- Nursing AutonomyDocument7 pagesNursing Autonomywafa materNo ratings yet
- Interprofessional Communication Between Medical Technologist and Health Care Professionals in Oriental Mindoro Provincial HospitalDocument58 pagesInterprofessional Communication Between Medical Technologist and Health Care Professionals in Oriental Mindoro Provincial Hospitalroneldayo62No ratings yet
- Leadership Is Important in Healthcare Now To AddressDocument3 pagesLeadership Is Important in Healthcare Now To AddressDheeraj KumarNo ratings yet
- Leadership Styles: March 2018Document7 pagesLeadership Styles: March 2018Zoe NguyenNo ratings yet
- Clinical Supervision: A Means of Promoting Reciprocity Between Practitioners and AcademicsDocument11 pagesClinical Supervision: A Means of Promoting Reciprocity Between Practitioners and AcademicsempananNo ratings yet
- Leadership and Its Effect On Health ManagementDocument14 pagesLeadership and Its Effect On Health ManagementChandu PanditNo ratings yet
- Masters ThesisDocument33 pagesMasters ThesisChristine Elaine Batusin IlaganNo ratings yet
- Challenges & Issues in Nursing LeadershipDocument3 pagesChallenges & Issues in Nursing LeadershipFrancis Adrian50% (2)
- Challenge Leading Nursing in Healthcare TeamsDocument17 pagesChallenge Leading Nursing in Healthcare TeamsAnisah WijayaNo ratings yet
- Framework Final FlowDocument6 pagesFramework Final FlowJelyza Jade Davidao BiolNo ratings yet
- Clinical Leadership Development and Education For NursesDocument10 pagesClinical Leadership Development and Education For NursesVia Eliadora TogatoropNo ratings yet
- 00006216-200801000-00008 Fewster-Thuente Velsor FriedrichDocument9 pages00006216-200801000-00008 Fewster-Thuente Velsor FriedrichÀi ZìjǐNo ratings yet
- Chapter 2 PDFDocument64 pagesChapter 2 PDFsubiNo ratings yet
- Medical Education - 2017 - Cleland - Using Paradox Theory To Understand Responses To Tensions Between Service and TrainingDocument14 pagesMedical Education - 2017 - Cleland - Using Paradox Theory To Understand Responses To Tensions Between Service and TrainingJack WaltonNo ratings yet
- Ten Principles of Good Interdisciplinary Team Work: Research Open AccessDocument11 pagesTen Principles of Good Interdisciplinary Team Work: Research Open AccessfairwoodsNo ratings yet
- Dimensions of Learning Organizations Questionnaire (DLOQ) in A Low-Resource Health Care Setting in NepalDocument8 pagesDimensions of Learning Organizations Questionnaire (DLOQ) in A Low-Resource Health Care Setting in Nepalsapit90No ratings yet
- The Role of Re Ective Practice in Pharmacy: Education For Health April 2003Document8 pagesThe Role of Re Ective Practice in Pharmacy: Education For Health April 2003Muh. Miftahul IchsanNo ratings yet
- The Physician Leader: Teaching Leadership in MedicineDocument7 pagesThe Physician Leader: Teaching Leadership in MedicineKUTLUHAN YILMAZ Prof DrNo ratings yet
- Transdisciplinarity What Competencies Do Future Healthcare Managers Need To SucceedDocument6 pagesTransdisciplinarity What Competencies Do Future Healthcare Managers Need To SucceedJoyce OpingaNo ratings yet
- Nursing Management and Leadership Approaches From The Perspective of Registered Nurses in PortugalDocument8 pagesNursing Management and Leadership Approaches From The Perspective of Registered Nurses in PortugalLyaNo ratings yet
- Ethics in Nursing Leadership: Transactional, Transformational, and Authentic Leadership Are Popular ModelsDocument10 pagesEthics in Nursing Leadership: Transactional, Transformational, and Authentic Leadership Are Popular ModelsJmarie Brillantes PopiocoNo ratings yet
- GREENER - Health Management As Strategic BehaviourDocument17 pagesGREENER - Health Management As Strategic Behaviourryan yeomanNo ratings yet
- Artikel BagusDocument13 pagesArtikel BagusAtikah AbayNo ratings yet
- Karam 2018Document14 pagesKaram 2018Sigit Nian PrasetyoNo ratings yet
- Nurses' Policy in Uence: A Concept Analysis: ArticleDocument9 pagesNurses' Policy in Uence: A Concept Analysis: ArticleTria PratiwiNo ratings yet
- 0rder 271 NRS-493 - PROFESSIONAL CAPSTONE & PRACTICUMDocument18 pages0rder 271 NRS-493 - PROFESSIONAL CAPSTONE & PRACTICUMjoshua chegeNo ratings yet
- Increasing The Relevance of Research ToDocument10 pagesIncreasing The Relevance of Research ToagvhvwnetlkqubeckwNo ratings yet
- Readings - Prof. MG JomonDocument78 pagesReadings - Prof. MG JomonParth SarthiNo ratings yet
- Production and Operations ManagementDocument10 pagesProduction and Operations Managementbirbal mahato0% (1)
- Jurnal Retensi 2Document20 pagesJurnal Retensi 2tasyaNo ratings yet
- Leadership Styles A Case of Two Hospitals in The USDocument23 pagesLeadership Styles A Case of Two Hospitals in The USWagiono Suparan100% (2)
- Health CollaborationsDocument13 pagesHealth CollaborationsVivi DionNo ratings yet
- Nembhard Edmondson - 2006 Making It Safe-The Effects of Leader Inclusiveness PDFDocument26 pagesNembhard Edmondson - 2006 Making It Safe-The Effects of Leader Inclusiveness PDFMd. Shahfayet JinnahNo ratings yet
- Pakistan Health SolutionsDocument43 pagesPakistan Health SolutionsShayan Abbas100% (1)
- Setting The Agenda For Nurse Leadership in India: What Is MissingDocument10 pagesSetting The Agenda For Nurse Leadership in India: What Is MissingAnnamaria FoladoriNo ratings yet
- Why Money Are Not So Effective To PhysiciansDocument17 pagesWhy Money Are Not So Effective To PhysiciansLeonardo SimonciniNo ratings yet
- Empirical Research in Clinical Supervision: A Systematic Review and Suggestions For Future StudiesDocument11 pagesEmpirical Research in Clinical Supervision: A Systematic Review and Suggestions For Future StudiesStefan BasilNo ratings yet
- PurposeDocument1 pagePurposeZed MatthewNo ratings yet
- DMC 110117012353 Phpapp02 PDFDocument16 pagesDMC 110117012353 Phpapp02 PDFJalajarani AridassNo ratings yet
- SJP 14 31 PDFDocument8 pagesSJP 14 31 PDFDaniela EscalanteNo ratings yet
- Strategic Elements of Residency Training in China: Transactional Leadership, Self-Efficacy, and Employee-Orientation CultureDocument8 pagesStrategic Elements of Residency Training in China: Transactional Leadership, Self-Efficacy, and Employee-Orientation CultureChenpeng FENGNo ratings yet
- Fischer 2017Document7 pagesFischer 2017tiago alvesNo ratings yet
- Handbook of Healthcare Management ChapteDocument17 pagesHandbook of Healthcare Management ChapteoidiegopmNo ratings yet
- Leadership in NursingDocument14 pagesLeadership in NursingzainuddinNo ratings yet
- Spesifikasi, SONOSCAPE Video Endoscope System HD-500Document3 pagesSpesifikasi, SONOSCAPE Video Endoscope System HD-500Ang Timotius Raymond AngkajayaNo ratings yet
- The Challenges of Leadership: Robert C. Myrtle, DPADocument6 pagesThe Challenges of Leadership: Robert C. Myrtle, DPAAng Timotius Raymond AngkajayaNo ratings yet
- The Revolution in Hospital ManagementDocument22 pagesThe Revolution in Hospital ManagementAng Timotius Raymond AngkajayaNo ratings yet
- Parand 2014 Sys Rev MGT BMJODocument17 pagesParand 2014 Sys Rev MGT BMJOAng Timotius Raymond AngkajayaNo ratings yet
- THE Impact OF Organizational Structure AND Administrative Polices of Hospitals On Delivering Quality of Service For Patients SatisfactionDocument10 pagesTHE Impact OF Organizational Structure AND Administrative Polices of Hospitals On Delivering Quality of Service For Patients SatisfactionAng Timotius Raymond AngkajayaNo ratings yet
- Recovering Restoring and Renewing The FoundationsDocument14 pagesRecovering Restoring and Renewing The FoundationsAng Timotius Raymond AngkajayaNo ratings yet
- Presentasi Kasus: Gangguan Afektif Bipolar Episode Kini Depresif Ringan Atau SedangDocument1 pagePresentasi Kasus: Gangguan Afektif Bipolar Episode Kini Depresif Ringan Atau SedangAng Timotius Raymond AngkajayaNo ratings yet
- 6802 4301 Data AnalysisDocument31 pages6802 4301 Data AnalysisAnsuman PrasadNo ratings yet
- Long Division WorksheetDocument12 pagesLong Division WorksheetHoi Yuet ChauNo ratings yet
- Guidelines For Admission To MCA Program at HBTU, Kanpur For Session 2019-20 (Offline-On Campus Counselling)Document4 pagesGuidelines For Admission To MCA Program at HBTU, Kanpur For Session 2019-20 (Offline-On Campus Counselling)Nikky SinghNo ratings yet
- 印尼演讲稿1Document36 pages印尼演讲稿1ekounidhaNo ratings yet
- Math Majorship 1Document13 pagesMath Majorship 1Charl Niño CutamoraNo ratings yet
- Industrial Visit To HNL: IEEE Student Branch Rajiv Gandhi Institute of Technology, KottayamDocument3 pagesIndustrial Visit To HNL: IEEE Student Branch Rajiv Gandhi Institute of Technology, KottayamSoanz AugustineNo ratings yet
- Sales Document StructureDocument5 pagesSales Document StructureShashi RayappagariNo ratings yet
- Energy Led: TV3170 / 3190 HDTVDocument25 pagesEnergy Led: TV3170 / 3190 HDTVVladimir PašićNo ratings yet
- 8 Module VIII Disaster Risk Reduction and ManagementDocument39 pages8 Module VIII Disaster Risk Reduction and ManagementSunny SshiNo ratings yet
- (TDB) Single For Europe (R32, HP) Ver.3.1 - 200326Document376 pages(TDB) Single For Europe (R32, HP) Ver.3.1 - 200326DAV DavdNo ratings yet
- Kasuda Ground Temp ProfileDocument3 pagesKasuda Ground Temp ProfileTe PaixonoNo ratings yet
- Mahle Air Filter (Primary) For CaterpillarDocument12 pagesMahle Air Filter (Primary) For Caterpillarsuraj pandeyNo ratings yet
- Transport Department, Uttar PradeshDocument2 pagesTransport Department, Uttar PradeshNishant100% (1)
- PhotodetectorsDocument46 pagesPhotodetectorsShivam AgarwalNo ratings yet
- Sheikhupura 500Kv Grid Station: Usaid Energy Policy ProgramDocument9 pagesSheikhupura 500Kv Grid Station: Usaid Energy Policy ProgramMuhammad Ramzan KhanNo ratings yet
- Heavy Engineering Corporation Project ReportDocument28 pagesHeavy Engineering Corporation Project ReportAshish jhaNo ratings yet
- Bridge Loading in Malaysia Past Present and The FuDocument12 pagesBridge Loading in Malaysia Past Present and The FuOscarKonzultNo ratings yet
- Resume Tracy 2018 Portfolio2Document2 pagesResume Tracy 2018 Portfolio2api-418542159No ratings yet
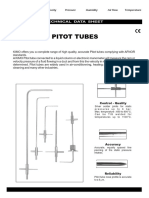
- FT Pitot Type LDocument4 pagesFT Pitot Type LThai VoNo ratings yet
- lm723 PDFDocument21 pageslm723 PDFjet_media100% (1)
- Bendixson-Dulac Criterion and Reduction To Global Uniqueness in The Problem of Estimating The Number of Limit CyclesDocument9 pagesBendixson-Dulac Criterion and Reduction To Global Uniqueness in The Problem of Estimating The Number of Limit CyclesChristopher LimachiNo ratings yet
- Ganpat University U.V. Patel College of Engineering Mechatronics Engineering Department Experiment: - 4Document5 pagesGanpat University U.V. Patel College of Engineering Mechatronics Engineering Department Experiment: - 4Jaygopal SharmaNo ratings yet
- Roland Sh-201 - Guide Book EnGLISHDocument15 pagesRoland Sh-201 - Guide Book EnGLISHHURRYSTARNo ratings yet
- O M ManualDocument8 pagesO M ManualAmjed HNo ratings yet
- 10% Persuasive Speech Outline Template s12021Document8 pages10% Persuasive Speech Outline Template s12021Zulkhairi AlzuhdiNo ratings yet
- International Journal of Mineral Processing: Senol Cetinkaya, Serafettin ErogluDocument3 pagesInternational Journal of Mineral Processing: Senol Cetinkaya, Serafettin ErogluMIzan NursiadiNo ratings yet
- Improvement Effect of Vacuum Consolidation and Prefabricated Vertical Drain in Peat GroundDocument10 pagesImprovement Effect of Vacuum Consolidation and Prefabricated Vertical Drain in Peat GroundMark MengNo ratings yet
- Dubai Metro ProjectDocument67 pagesDubai Metro ProjectMustafa Uzyardoğan100% (4)
- Invotech Scroll - YM - YF - RefrigerationDocument31 pagesInvotech Scroll - YM - YF - RefrigerationDiego Elías SuazoNo ratings yet