Download as xlsx, pdf, or txt
You might also like
- Report Industry TrainingDocument44 pagesReport Industry Trainingaaaa67% (6)
- Campushash: Evolving Business Model of An Entrepreneurial VentureDocument10 pagesCampushash: Evolving Business Model of An Entrepreneurial VentureTanujSood100% (1)
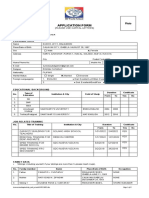
- Application Form - Mayapada Healthcare GroupDocument6 pagesApplication Form - Mayapada Healthcare GroupShirohigeNo ratings yet
- Jacobin 1 PDFDocument23 pagesJacobin 1 PDFPabloNo ratings yet
- A Written Reflection On Work Experience 2011Document13 pagesA Written Reflection On Work Experience 2011Chris-AnnHunterNo ratings yet
- Internet Expenses Data SheetDocument2 pagesInternet Expenses Data Sheetmiguelsias127100% (1)
- Modern Challenges in Operations ManagementDocument2 pagesModern Challenges in Operations ManagementRachit Arora71% (7)
- MayapadaDocument4 pagesMayapadaDika Adhi SriwigunaNo ratings yet
- NEW Application Form - Mayapada Healthcare GroupDocument4 pagesNEW Application Form - Mayapada Healthcare GroupFicky Haryudi50% (2)
- CHRIS JEFRY WONTE - Application Form Final - Mayapada Healthcare GroupDocument6 pagesCHRIS JEFRY WONTE - Application Form Final - Mayapada Healthcare GroupHiskia rambeNo ratings yet
- Silva Sri Nurwahyuni - Bidan MayapadaDocument4 pagesSilva Sri Nurwahyuni - Bidan MayapadaSilva SnwNo ratings yet
- NEW Application Form - Mayapada Healthcare Group FixDocument4 pagesNEW Application Form - Mayapada Healthcare Group FixGebastianvverlove Yolandasforevera AkanslalusetyapdasatuhatiNo ratings yet
- FormDocument1 pageFormSebri Yunita NakluyNo ratings yet
- NEW Application Form - Mayapada Healthcare Group (31) SalinanDocument6 pagesNEW Application Form - Mayapada Healthcare Group (31) SalinanAtika NrhdNo ratings yet
- NEW Application Form - Mayapada Healthcare GroupDocument4 pagesNEW Application Form - Mayapada Healthcare GroupMoch Naufal MahbubyNo ratings yet
- Regional Office: Dav Institutions, Odisha Zone-Ii Dr. A. N. Khosla Dav Public School, RourkelaDocument2 pagesRegional Office: Dav Institutions, Odisha Zone-Ii Dr. A. N. Khosla Dav Public School, RourkelaRajat Kumar PadhanNo ratings yet
- Job Application FormDocument3 pagesJob Application FormmarstafatahilahNo ratings yet
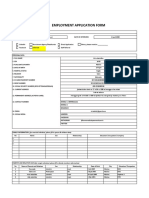
- Employment Application Form: 1.position Applying For 2.employee InformationDocument3 pagesEmployment Application Form: 1.position Applying For 2.employee InformationDasep PratamaNo ratings yet
- Application Form 2022Document4 pagesApplication Form 2022Eunice Joy Cuntapay BalganionNo ratings yet
- Bal IqbalDocument2 pagesBal IqbalIqbal OktafianNo ratings yet
- APPLICATION FORM - Revisi Terbaru SD IsiDocument10 pagesAPPLICATION FORM - Revisi Terbaru SD IsiAldy BimaNo ratings yet
- Application Form - Indolab Mayapada Healthcare Group (37) ZDocument5 pagesApplication Form - Indolab Mayapada Healthcare Group (37) ZAnas SyafaatNo ratings yet
- Form Lamaran IngDocument2 pagesForm Lamaran IngFahmi Nur'AfifNo ratings yet
- IqbalDocument2 pagesIqbalIqbal OktafianNo ratings yet
- Employment Application Form: 1.position Applying For 2.employee InformationDocument3 pagesEmployment Application Form: 1.position Applying For 2.employee InformationDasep PratamaNo ratings yet
- Employment Application Form: 1.position Applying For 2.employee InformationDocument3 pagesEmployment Application Form: 1.position Applying For 2.employee InformationMuhammad KafiNo ratings yet
- Form Application BankShinhanDocument6 pagesForm Application BankShinhanRafi MahendraNo ratings yet
- Employment Application Form: 1.position Applying For Operator Production 2.employee InformationDocument3 pagesEmployment Application Form: 1.position Applying For Operator Production 2.employee InformationTrio Ary Agung YunartoNo ratings yet
- Application Form: (Please Fill in Details Below For Our Reference) Job Application FormDocument6 pagesApplication Form: (Please Fill in Details Below For Our Reference) Job Application Formmutia makhfirahNo ratings yet
- WawaDocument5 pagesWawaLuthfie ZulkarnaenNo ratings yet
- Form Application SENTRA BOGADocument8 pagesForm Application SENTRA BOGANasir MuhammadNo ratings yet
- Employment Form - Aulia PitalokaDocument3 pagesEmployment Form - Aulia PitalokaRuby AfifahNo ratings yet
- HRD-QOHSER-002 Application FormDocument7 pagesHRD-QOHSER-002 Application FormMajestik ggNo ratings yet
- Form Application MNC Land Rev1Document6 pagesForm Application MNC Land Rev1Syukron Khotibul UmamNo ratings yet
- Rahmat Tri Fauzi Manujal: Bukittinggi, IndonesiaDocument1 pageRahmat Tri Fauzi Manujal: Bukittinggi, IndonesiaIqbal Afriansyah ZainNo ratings yet
- Application For Employement Form: PT Apexindo Pratama Duta TBKDocument6 pagesApplication For Employement Form: PT Apexindo Pratama Duta TBKYoung BrotherNo ratings yet
- ApplicationDocument6 pagesApplicationYohanes DogomoNo ratings yet
- Uthman Bin Affan Foundation Academy Inc. Application FormDocument5 pagesUthman Bin Affan Foundation Academy Inc. Application FormShaira MPNo ratings yet
- Copy of Form Aplikasi Pelamar New(1)Document2 pagesCopy of Form Aplikasi Pelamar New(1)26franskiesNo ratings yet
- Applicationform - Ferdy Suhanda S.M.Document7 pagesApplicationform - Ferdy Suhanda S.M.Ratih SekarNo ratings yet
- Curriculum Vitae (CV) : 1. Personal DetailDocument1 pageCurriculum Vitae (CV) : 1. Personal DetailMutia RamdaniNo ratings yet
- Modified Basic Education Enrollment Form / /: Annex 1Document2 pagesModified Basic Education Enrollment Form / /: Annex 1F-CABAGUING, HANNAH M.No ratings yet
- 1. Form Aplikasi Pelamar_mentari pDocument4 pages1. Form Aplikasi Pelamar_mentari plabpkmpakuhajiNo ratings yet
- Admissiondavwalmi - Davonline.in XIReport - Aspx Applicant 2106Document2 pagesAdmissiondavwalmi - Davonline.in XIReport - Aspx Applicant 2106tilawatequran7860No ratings yet
- MPDF PDFDocument4 pagesMPDF PDFramharimbaNo ratings yet
- Rujean Miguel Suratos: Banaoang West, Mangaldanpangasinan 09075896925/09159885444Document3 pagesRujean Miguel Suratos: Banaoang West, Mangaldanpangasinan 09075896925/09159885444Rose Ann Miguel SuratosNo ratings yet
- Sbi Education Loan FormDocument4 pagesSbi Education Loan FormHarish MishraNo ratings yet
- Student Directory 2022 2023 10 PIETYDocument4 pagesStudent Directory 2022 2023 10 PIETYGlory Ann DelovioNo ratings yet
- Cv. DediDocument1 pageCv. DediCitra PermatasariNo ratings yet
- Jl. Mama Salim No.02 Kp. Rancatimah RT 04/06 Kel. Cijorolebak Kec - Rangkasbitung Kab. Lebak Banten HPDocument3 pagesJl. Mama Salim No.02 Kp. Rancatimah RT 04/06 Kel. Cijorolebak Kec - Rangkasbitung Kab. Lebak Banten HPHerli YantoNo ratings yet
- Emey C. Adjedan ResumeeDocument2 pagesEmey C. Adjedan ResumeeAnonymous YxngpcBDDNo ratings yet
- Employment Application Form - Biyan Abi YogaDocument7 pagesEmployment Application Form - Biyan Abi YogaBiyan YogaNo ratings yet
- Ahmad Faraz Icp)Document2 pagesAhmad Faraz Icp)Ahmad Faraz VirkNo ratings yet
- Application FormDocument2 pagesApplication FormBevNo ratings yet
- Screenshot 2023-03-30 at 3.37.25 PMDocument12 pagesScreenshot 2023-03-30 at 3.37.25 PMrohit020304No ratings yet
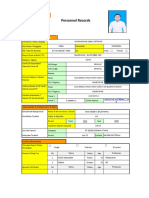
- Re (Form) Personnel Record JO - r2Document2 pagesRe (Form) Personnel Record JO - r2Jhon TonyNo ratings yet
- Wa0011Document6 pagesWa0011Andre CandraNo ratings yet
- Enc Encoded DgzJ24D4OGdhO1jSF2vObZDg5ZyYmvzocLabBA4iKz K6H ZHtUgtwvJpPQC8i0BogDocument28 pagesEnc Encoded DgzJ24D4OGdhO1jSF2vObZDg5ZyYmvzocLabBA4iKz K6H ZHtUgtwvJpPQC8i0BogIRENE MAY LEGASPINo ratings yet
- CV YabesDocument1 pageCV YabesOji SaputraNo ratings yet
- Hr-Form - Application FormDocument4 pagesHr-Form - Application Formavy mariel alcantaraNo ratings yet
- HRC - Forms - Employee Application Maria AyuDocument3 pagesHRC - Forms - Employee Application Maria Ayucontact.nonagonNo ratings yet
- Security Services Division Ministry of Home Affairs: Government of The People's Republic of BangladeshDocument1 pageSecurity Services Division Ministry of Home Affairs: Government of The People's Republic of Bangladeshshakil ahmedNo ratings yet
- h1 Student Profile.Document1 pageh1 Student Profile.Alexis jhoanne QuiranteNo ratings yet
- FM.03.HCD - Employment Application Form (Biyan Abi Yoga)Document8 pagesFM.03.HCD - Employment Application Form (Biyan Abi Yoga)Biyan YogaNo ratings yet
- Rujean Miguel Suratos: Banaoang West, Mangaldanpangasinan 09388128764Document6 pagesRujean Miguel Suratos: Banaoang West, Mangaldanpangasinan 09388128764Rose Ann Miguel SuratosNo ratings yet
- Ongc Pension&MediDocument17 pagesOngc Pension&MediNatarajan HariharanNo ratings yet
- BM ReviewDocument10 pagesBM ReviewFish SuperNo ratings yet
- Laborjure 2007Document120 pagesLaborjure 2007JenniferPizarrasCadiz-CarullaNo ratings yet
- Eugenio vs. CSC, 242 SCRA 196 (1995)Document10 pagesEugenio vs. CSC, 242 SCRA 196 (1995)Christiaan CastilloNo ratings yet
- Camelle Johnson V Happiest Baby LawsuitDocument28 pagesCamelle Johnson V Happiest Baby LawsuitJake SwearingenNo ratings yet
- Mu 0016Document306 pagesMu 0016rakeshrakeshNo ratings yet
- Regulation No 342 2015 Employment Relations Established by Religious and Charitable OrganizationsDocument4 pagesRegulation No 342 2015 Employment Relations Established by Religious and Charitable OrganizationsKidistNo ratings yet
- Parikrama Movie App ReportDocument25 pagesParikrama Movie App ReportPranav ShitoleNo ratings yet
- Jackson CaseDocument1 pageJackson CaseTasmia AhmedNo ratings yet
- Fuji v. Espiritu - CaseDocument21 pagesFuji v. Espiritu - CaseRobeh AtudNo ratings yet
- Civil Service CommissionDocument20 pagesCivil Service CommissionClea Amber FullanteNo ratings yet
- NUWHRAIN Vs SOLEDocument2 pagesNUWHRAIN Vs SOLECristelle Elaine ColleraNo ratings yet
- Labor Standars CasesDocument24 pagesLabor Standars CasesanjisyNo ratings yet
- Consequences of Industry 4.0 On Human Labour and Work OrganisationDocument8 pagesConsequences of Industry 4.0 On Human Labour and Work Organisationelif aslanNo ratings yet
- The Questionnaire On Employment Condition of College StudentsDocument5 pagesThe Questionnaire On Employment Condition of College Studentsyantao318No ratings yet
- Managing The Environment and THE Organization'S Culture: Principl Es of Management Mgts F 211Document39 pagesManaging The Environment and THE Organization'S Culture: Principl Es of Management Mgts F 211Sharwin NeemaNo ratings yet
- Labor LawDocument4 pagesLabor LawGrace EnriquezNo ratings yet
- Model Constitution For A CharitableDocument14 pagesModel Constitution For A Charitableal mooreNo ratings yet
- Art. 168. Compulsory Coverage.: With The Employee andDocument4 pagesArt. 168. Compulsory Coverage.: With The Employee andmarie deniegaNo ratings yet
- Trevon Office Administration SBADocument25 pagesTrevon Office Administration SBAArisha Nichols100% (2)
- Case Study - Labour LawDocument3 pagesCase Study - Labour LawAnoma Godage0% (2)
- SALARYDocument19 pagesSALARYHrishit Raj SardaNo ratings yet
- 2013-14 Teacher HandbookDocument47 pages2013-14 Teacher Handbook5cr1bdNo ratings yet
- Staffing Business Proposal: Mivian International Pvt. LTDDocument14 pagesStaffing Business Proposal: Mivian International Pvt. LTDSABYASACHINo ratings yet