Download as pdf or txt
You might also like
- NN10600-000 72s2Document24 pagesNN10600-000 72s2tommiyauNo ratings yet
- Handle Large Messages in Apache KafkaDocument59 pagesHandle Large Messages in Apache KafkaBùi Văn KiênNo ratings yet
- Cruickshank Et Al 2008 Revised National Guidelines For Analysis of Cerebrospinal Fluid For Bilirubin in SuspectedDocument25 pagesCruickshank Et Al 2008 Revised National Guidelines For Analysis of Cerebrospinal Fluid For Bilirubin in Suspectedshaun tanNo ratings yet
- CSF XanthochromiaDocument3 pagesCSF XanthochromiaShaikh Ghassan AbidNo ratings yet
- Standards For Analysis of Cerebrospinal Fluid CSF For XanthochromiaDocument2 pagesStandards For Analysis of Cerebrospinal Fluid CSF For XanthochromiaanggaririnNo ratings yet
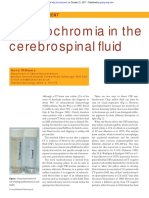
- Xanthochromia in The Cerebrospinal FL Uid: Image of The MomentDocument3 pagesXanthochromia in The Cerebrospinal FL Uid: Image of The MomentNutthawut JuldenNo ratings yet
- Ainsley H. Chalmers and Michelle Kiley (Departments of HaemaDocument3 pagesAinsley H. Chalmers and Michelle Kiley (Departments of HaemaswasahmedNo ratings yet
- 10.1515 - CCLM 2021 1320Document5 pages10.1515 - CCLM 2021 1320geo4maryNo ratings yet
- Utility - of - Scatterplot - Patterns - of - Automated - Hematology Analysers 2020Document6 pagesUtility - of - Scatterplot - Patterns - of - Automated - Hematology Analysers 2020tufis02No ratings yet
- Int J Lab Hematology - 2022 - Marinov - Validation of A Single Tube 3 Colour Immature Red Blood Cell Screening Assay ForDocument7 pagesInt J Lab Hematology - 2022 - Marinov - Validation of A Single Tube 3 Colour Immature Red Blood Cell Screening Assay ForMaria SousaNo ratings yet
- Ok 2Document7 pagesOk 2cydolusNo ratings yet
- 4-Hematology Analyzer - Detecting Erroneous Blood CountsDocument23 pages4-Hematology Analyzer - Detecting Erroneous Blood CountsRajeshNo ratings yet
- Performance Evaluation of The Body Fluid Mode On The Platform Sysmex XE-5000 Series Automated Hematology AnalyzerDocument9 pagesPerformance Evaluation of The Body Fluid Mode On The Platform Sysmex XE-5000 Series Automated Hematology AnalyzerbalkisNo ratings yet
- Briggs2006 PDFDocument10 pagesBriggs2006 PDFRonal WinterNo ratings yet
- Sysmex ScattergramsDocument7 pagesSysmex ScattergramsRuxandra Mesaros100% (1)
- Sop CBCDocument3 pagesSop CBCYousef AlshawafahNo ratings yet
- Pie 2018Document5 pagesPie 2018Tina HerreraNo ratings yet
- 2 The Use of The Laboratory: 1 Introducing Clinical BiochemistryDocument2 pages2 The Use of The Laboratory: 1 Introducing Clinical BiochemistryAmelia PebriantiNo ratings yet
- Indications Trephine BiopsyDocument6 pagesIndications Trephine Biopsyoki harisandiNo ratings yet
- El Examen de Sedimento de Orina Proporciona Más Información Diagnóstica en AKI Que Biomarcadores. 2022Document3 pagesEl Examen de Sedimento de Orina Proporciona Más Información Diagnóstica en AKI Que Biomarcadores. 2022Edwin Fabian Paz UrbanoNo ratings yet
- Erythrocyte and Plasma Volume MeasurementDocument6 pagesErythrocyte and Plasma Volume MeasurementMillenial AcousticsNo ratings yet
- CSF, UF 1000i, 2015Document11 pagesCSF, UF 1000i, 2015balkisNo ratings yet
- Evaluation of The Performance of Sysmex XN-3100 Automated Hematology Analyzer Regarding The Sysmex XE-2100 and Microscopic ExaminationDocument9 pagesEvaluation of The Performance of Sysmex XN-3100 Automated Hematology Analyzer Regarding The Sysmex XE-2100 and Microscopic ExaminationbalkisNo ratings yet
- Endourology and Stones Predictive Value of Leukocytosis For Infectious Complications After Percutaneous NephrolithotomyDocument5 pagesEndourology and Stones Predictive Value of Leukocytosis For Infectious Complications After Percutaneous NephrolithotomyJufrialdy AldyNo ratings yet
- Renal BiopsyDocument4 pagesRenal BiopsyDeshan AdikariNo ratings yet
- Efficacy of Ascitic Acid Dipstick Leukocyte Esterase Activity in Early Diagnosis of Spontaneous Bacterial PeritonitisDocument6 pagesEfficacy of Ascitic Acid Dipstick Leukocyte Esterase Activity in Early Diagnosis of Spontaneous Bacterial PeritonitisIJAR JOURNALNo ratings yet
- Pathophysiology of Ischaemic Stroke: Insights From Imaging, and Implications For Therapy and Drug DiscoveryDocument11 pagesPathophysiology of Ischaemic Stroke: Insights From Imaging, and Implications For Therapy and Drug DiscoveryryanafitrianaNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument10 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- 10 1111@ijlh 12760Document6 pages10 1111@ijlh 12760Hedo HidayatNo ratings yet
- HaematologyDocument11 pagesHaematologyIkram AzmanNo ratings yet
- The Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CanDocument9 pagesThe Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CananggaririnNo ratings yet
- Histoneur Hepatology PDFDocument7 pagesHistoneur Hepatology PDFmarianNo ratings yet
- Cardiac Output Estimation Using Ballistocardiography: A Feasibility Study in Healthy SubjectsDocument9 pagesCardiac Output Estimation Using Ballistocardiography: A Feasibility Study in Healthy SubjectsshucksmaamNo ratings yet
- Comparison of Cerebellomedullary and Lumbar CSF in Dogs With Neurological Disease Jvim.15700Document6 pagesComparison of Cerebellomedullary and Lumbar CSF in Dogs With Neurological Disease Jvim.15700hematologiaNo ratings yet
- New QuantitiesDocument6 pagesNew Quantities20100117 Bùi Thùy VyNo ratings yet
- Diagnosis of Brucella: Prepared By: Bahaa Mostafa Kamel 415Document6 pagesDiagnosis of Brucella: Prepared By: Bahaa Mostafa Kamel 415Bahaa ShaabanNo ratings yet
- Feline Blood Film 230902 043358Document13 pagesFeline Blood Film 230902 04335897namithaNo ratings yet
- Science: Assessment of The Reliability of The Sysmex XE-5000 Analyzer To Detect Platelet ClumpsDocument6 pagesScience: Assessment of The Reliability of The Sysmex XE-5000 Analyzer To Detect Platelet ClumpsnivmastNo ratings yet
- 12 White Blood Cell Counting Techniques in BirdsDocument5 pages12 White Blood Cell Counting Techniques in BirdsPablo LópezNo ratings yet
- 01 STR 8 5 613Document5 pages01 STR 8 5 613Seblewengel AbateNo ratings yet
- Yield of Induced Sputum in Clinically Diagnosed Pulmonary TuberculosisDocument7 pagesYield of Induced Sputum in Clinically Diagnosed Pulmonary TuberculosisIJAR JOURNALNo ratings yet
- Clasificacion de Biopsias Ellis Et Al.Document6 pagesClasificacion de Biopsias Ellis Et Al.tatianaNo ratings yet
- Ann Clin Biochem-2009-Guy-468-76Document9 pagesAnn Clin Biochem-2009-Guy-468-76keyssiNo ratings yet
- Cerebrospinal FluidDocument16 pagesCerebrospinal FluidSolomon Fallah Foa SandyNo ratings yet
- Review Article Perfusion Imaging in Ischaemic StrokeDocument4 pagesReview Article Perfusion Imaging in Ischaemic Strokesepty_auliaNo ratings yet
- Optimal Blood Pressure During CPBDocument7 pagesOptimal Blood Pressure During CPBAdy WarsanaNo ratings yet
- Neonatal Neurosonography: A Pictorial Essay: EuroradiologyDocument13 pagesNeonatal Neurosonography: A Pictorial Essay: EuroradiologyAnom RahartoNo ratings yet
- Leaders Bone Marrow Aspiration: BjbainDocument7 pagesLeaders Bone Marrow Aspiration: BjbaintmrezatandiNo ratings yet
- Design and Analysis of HSC-BPPV Diagnostic ManeuveDocument11 pagesDesign and Analysis of HSC-BPPV Diagnostic ManeuveSelinay YAȘANo ratings yet
- Clinical Biochemistry: E. Schapkaitz, S. RaburabuDocument7 pagesClinical Biochemistry: E. Schapkaitz, S. RaburabuMunawwar SaukaniNo ratings yet
- EASL Clinical Practice Guidelines On Sclerosing Cholangitis Elsevier Enhanced ReaderDocument1 pageEASL Clinical Practice Guidelines On Sclerosing Cholangitis Elsevier Enhanced Readerchiara valentina luglioNo ratings yet
- Letter To The Editor: Comparison Between Automated and Microscopic Analysis in Body Fluids CytologyDocument3 pagesLetter To The Editor: Comparison Between Automated and Microscopic Analysis in Body Fluids CytologybalkisNo ratings yet
- Zhang 2000Document6 pagesZhang 2000hoangkiett0904No ratings yet
- JR2 RizaDocument3 pagesJR2 RizaCitra DewiNo ratings yet
- 10.1515 - Labmed 2023 0064Document9 pages10.1515 - Labmed 2023 0064Arturo Eduardo Huarcaya OntiverosNo ratings yet
- Basics of Kidney Biopsy: A Nephrologist's Perspective: Review ArticleDocument11 pagesBasics of Kidney Biopsy: A Nephrologist's Perspective: Review ArticleBilal MaloukaNo ratings yet
- BlacT Package InsertDocument2 pagesBlacT Package InsertaliborabasNo ratings yet
- XN 3000 VS BeckmanDocument8 pagesXN 3000 VS BeckmanZied FehriNo ratings yet
- Kjtcs 47 124Document5 pagesKjtcs 47 124dalozpa23No ratings yet
- HaematologiDocument10 pagesHaematologigroup3akademikNo ratings yet
- 10 0000@www Jrheum Org@32@5@828Document5 pages10 0000@www Jrheum Org@32@5@828Yasser AlghrafyNo ratings yet
- Clinical Neuroanatomical TechniquesDocument6 pagesClinical Neuroanatomical TechniquesMWNo ratings yet
- Cha 10Document2 pagesCha 10MWNo ratings yet
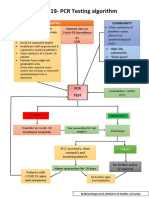
- CovidpcrtestingalgorithmDocument1 pageCovidpcrtestingalgorithmMWNo ratings yet
- Original Article: Macroenzyme Detection by Polyethylene Glycol PrecipitationDocument7 pagesOriginal Article: Macroenzyme Detection by Polyethylene Glycol PrecipitationMWNo ratings yet
- Color Atlas of BrainDocument8 pagesColor Atlas of BrainMWNo ratings yet
- Case Report: Excessive Calcium Ingestion Leading To Milk-Alkali SyndromeDocument3 pagesCase Report: Excessive Calcium Ingestion Leading To Milk-Alkali SyndromeMWNo ratings yet
- Validation Vs VerificationDocument46 pagesValidation Vs VerificationMW100% (2)
- Case ReportDocument3 pagesCase ReportMWNo ratings yet
- WHO Practical GuideDocument113 pagesWHO Practical GuideMWNo ratings yet
- Short ReportDocument4 pagesShort ReportMWNo ratings yet
- Reference Intervals - Direct Priori MethodDocument5 pagesReference Intervals - Direct Priori MethodMWNo ratings yet
- AACB 2013 Lab QCDocument9 pagesAACB 2013 Lab QCMW100% (1)
- Hazardous Materials Operating GuideDocument128 pagesHazardous Materials Operating GuidenhishamNo ratings yet
- Understanding and Responding To Self-Harm by Allan HouseDocument9 pagesUnderstanding and Responding To Self-Harm by Allan HousesimasNo ratings yet
- Identifikasi Kondisi Dan Penanganan Bangunan Pelengkap Infrastruktur JalanDocument6 pagesIdentifikasi Kondisi Dan Penanganan Bangunan Pelengkap Infrastruktur JalanFarhanNo ratings yet
- Implications of Covid-19 For Mental Health.Document3 pagesImplications of Covid-19 For Mental Health.Lina CasasNo ratings yet
- Base Oils: Technical Data Sheet NEXBASE 3043Document2 pagesBase Oils: Technical Data Sheet NEXBASE 3043Axel Mahya AvichenaNo ratings yet
- Political Science Assignment: POL QDocument4 pagesPolitical Science Assignment: POL QEktaNo ratings yet
- Abs Sire Directory 23Document40 pagesAbs Sire Directory 23sfranjul64No ratings yet
- True or False (8 PTS.) : Bio 11 2 Lecture LE Mock Exam October 2015Document8 pagesTrue or False (8 PTS.) : Bio 11 2 Lecture LE Mock Exam October 2015Alexander Miguel SyNo ratings yet
- STEB Asia - Biskuat FIFA Promo 2021Document4 pagesSTEB Asia - Biskuat FIFA Promo 2021imeldaNo ratings yet
- Hearst Demystifying Media Fireside Chat - The Bloomberg Way With Matthew WinklerDocument16 pagesHearst Demystifying Media Fireside Chat - The Bloomberg Way With Matthew WinklerDemystifying MediaNo ratings yet
- Microsoft-Case StudyDocument26 pagesMicrosoft-Case StudyHiten GuptaNo ratings yet
- Customer Satisfaction and Employee InvolvementDocument36 pagesCustomer Satisfaction and Employee InvolvementMaria Rebecca Toledo SalarNo ratings yet
- Analysis and Design of A Charge Pump Circuit For High CurrentDocument4 pagesAnalysis and Design of A Charge Pump Circuit For High CurrenthsharghiNo ratings yet
- SKYPAD Pocket Firmware Instructions PDFDocument3 pagesSKYPAD Pocket Firmware Instructions PDFAbelito FloresNo ratings yet
- Creation, Torah, and Revealed Wisdom in Some Second Temple Sapiential Texts (Sirach, 4qinstruction, 4Q185, and 4Q525) : A Response To John KampenDocument24 pagesCreation, Torah, and Revealed Wisdom in Some Second Temple Sapiential Texts (Sirach, 4qinstruction, 4Q185, and 4Q525) : A Response To John KampenKent Jerson CasianoNo ratings yet
- The Pavilion Lounge: A Cricket Themed LoungeDocument34 pagesThe Pavilion Lounge: A Cricket Themed LoungeShreya DGNo ratings yet
- Benevision N22/N19/N17/N15/ N12: Quick Reference GuideDocument40 pagesBenevision N22/N19/N17/N15/ N12: Quick Reference GuideVinoth RaviNo ratings yet
- Prevalence of Interpersonal Violence Against Athletes in The Sport Context (2017)Document5 pagesPrevalence of Interpersonal Violence Against Athletes in The Sport Context (2017)Juan Kmilo Martinez FernandezNo ratings yet
- CSC 218 Notes 3Document8 pagesCSC 218 Notes 3Musa JubrilNo ratings yet
- Assignment 2 Lesson Plan AnalysisDocument14 pagesAssignment 2 Lesson Plan Analysisapi-373008418No ratings yet
- Janome 900CPX Coverstitch Sewing Machine Instruction ManualDocument26 pagesJanome 900CPX Coverstitch Sewing Machine Instruction ManualiliiexpugnansNo ratings yet
- Neos 100Document34 pagesNeos 100David Bustamante ReyNo ratings yet
- Lesson Plan Year 3 LNS Pets WorldDocument6 pagesLesson Plan Year 3 LNS Pets WorldtgDeanNo ratings yet
- Helsinki Finnish Linus Torvalds Linux KernelDocument6 pagesHelsinki Finnish Linus Torvalds Linux KernelArnav PrasadNo ratings yet
- Draft Minutes Apr 5, 2023Document5 pagesDraft Minutes Apr 5, 2023PPSMU PAMPANGA PPONo ratings yet
- Inductive and Deductive ReasoningDocument6 pagesInductive and Deductive Reasoningkiahjessie100% (3)
- The Nature of Human Resource ManagementDocument14 pagesThe Nature of Human Resource ManagementEmerito PerezNo ratings yet
- Modal Testing of A Flexible Wing On A Dynamically Active Test Fixture Using The Fixed Base Correction MethodDocument22 pagesModal Testing of A Flexible Wing On A Dynamically Active Test Fixture Using The Fixed Base Correction Methodscramjet007No ratings yet