Download as pdf or txt
You might also like
- Progressive Insurance Card PDFDocument3 pagesProgressive Insurance Card PDFjmvredskinsNo ratings yet
- Allstate Declaration - 20221110 - 0001Document4 pagesAllstate Declaration - 20221110 - 0001Shilyn KaufmanNo ratings yet
- Verification of InsuranceDocument1 pageVerification of InsuranceJeremy Ware100% (2)
- AT&TDocument2 pagesAT&TSteffani GuzmánNo ratings yet
- Auto Insurance Coverage Summary This Is A Copy of Your Declarations PageDocument3 pagesAuto Insurance Coverage Summary This Is A Copy of Your Declarations PageMorenita ParelesNo ratings yet
- Declarations Page 1Document3 pagesDeclarations Page 1Reospro21 lopezNo ratings yet
- Auto Insurance Policy Amended Declarations: Named Insured VehiclesDocument2 pagesAuto Insurance Policy Amended Declarations: Named Insured VehiclesSMART CHOICE AUTO GROUPNo ratings yet
- Estmt - 2023 06 15Document14 pagesEstmt - 2023 06 15lorielys0909No ratings yet
- CODE - 00491630201020000022: Declaration of Insurance PolicyDocument2 pagesCODE - 00491630201020000022: Declaration of Insurance PolicyKeller Brown Jnr100% (1)
- DeclarationsPage PDFDocument2 pagesDeclarationsPage PDFGuy GuyersonNo ratings yet
- Verification of InsuranceDocument1 pageVerification of InsuranceMorenita ParelesNo ratings yet
- Account StatementDocument6 pagesAccount StatementHxor Haxor0% (1)
- Customer PDFDocument2 pagesCustomer PDFSuraj BhandariNo ratings yet
- Verification of Insurance-2Document1 pageVerification of Insurance-2DebNo ratings yet
- AP Driving Licence ImagesDocument14 pagesAP Driving Licence ImagesKolasani MohanNo ratings yet
- Declarations Page (Auto Insurance Coverage Summary) : © 2012-2021 Metromile Inc. All Rights Reserved. OR-AD-0618Document2 pagesDeclarations Page (Auto Insurance Coverage Summary) : © 2012-2021 Metromile Inc. All Rights Reserved. OR-AD-0618Srinivasan PNo ratings yet
- ABB Case StudyDocument4 pagesABB Case StudyAl Moazer Abdulaal AbdulateefNo ratings yet
- October 20, 2022 Account Number: 100 146 720 485 Amount Due: $49.14 Due Date: November 09, 2022Document2 pagesOctober 20, 2022 Account Number: 100 146 720 485 Amount Due: $49.14 Due Date: November 09, 2022Carlos Andres Barrera CastillaNo ratings yet
- Verification of InsuranceDocument1 pageVerification of InsuranceMarco Antonio SalgadoNo ratings yet
- Customer Agreement H1935-108804Document3 pagesCustomer Agreement H1935-108804Angel RamírezNo ratings yet
- PolicyconfirmationDocument1 pagePolicyconfirmationTascie CookNo ratings yet
- Glober Pro SpecimenDocument2 pagesGlober Pro SpecimenEduardo PerezNo ratings yet
- 2019 Master Piping Products Price List (Effective 8-15-2019) Rev-FinalDocument108 pages2019 Master Piping Products Price List (Effective 8-15-2019) Rev-FinalpogisimpatikoNo ratings yet
- Invoice For Missed Toll: Second NoticeDocument2 pagesInvoice For Missed Toll: Second NoticeTKnowlesNo ratings yet
- Eoi 35695472Document2 pagesEoi 35695472D SkaNo ratings yet
- Root Declarations Page 20210916Document4 pagesRoot Declarations Page 20210916SMART CHOICE AUTO GROUPNo ratings yet
- AmazonBusinessInvoice#1T73 L4P7 FHGCDocument2 pagesAmazonBusinessInvoice#1T73 L4P7 FHGCRohan SINGHNo ratings yet
- Jinny Choe Temp Mem CardDocument1 pageJinny Choe Temp Mem CardginauineNo ratings yet
- Estatement Chase JuneDocument6 pagesEstatement Chase JuneAtta ur RehmanNo ratings yet
- CustomerOrder#H4705 208050 PDFDocument3 pagesCustomerOrder#H4705 208050 PDFSindy CruzNo ratings yet
- BillDocument6 pagesBillitteahad zihanNo ratings yet
- Shewale Light BillDocument1 pageShewale Light BillArman TamboliNo ratings yet
- Farmers Insurance - Auto Quote - AnakarenDocument6 pagesFarmers Insurance - Auto Quote - Anakarenluisalcantara12345678No ratings yet
- Billing Invoice Statement Template-67448Document1 pageBilling Invoice Statement Template-67448Neil ScribdNo ratings yet
- Utility Bill Free TemplateDocument2 pagesUtility Bill Free TemplateelaamlyNo ratings yet
- View Bill 08302023Document6 pagesView Bill 08302023Steven NietoNo ratings yet
- IDCARDDocument1 pageIDCARDroshawn waldenNo ratings yet
- 4600229175 - CopyDocument2 pages4600229175 - CopyData BaseNo ratings yet
- Confirmation: 1-888-205-8118 M-F 6:30am PST To 5:30pm PSTDocument1 pageConfirmation: 1-888-205-8118 M-F 6:30am PST To 5:30pm PSTKarthik SheshadriNo ratings yet
- Details For Order #408-5642390-7631512: Not Yet DispatchedDocument1 pageDetails For Order #408-5642390-7631512: Not Yet DispatchedJerin PeterNo ratings yet
- Payment Information Below, Bill Details Begin On The Next PageDocument6 pagesPayment Information Below, Bill Details Begin On The Next PageJUAN ESTRADANo ratings yet
- Nebraska Insurance Card Nebraska Insurance CardDocument2 pagesNebraska Insurance Card Nebraska Insurance CardRon FreemanNo ratings yet
- 138 July Bill PDFDocument1 page138 July Bill PDFThanh Duyên Phan ThịNo ratings yet
- Auto Policy BillDocument2 pagesAuto Policy BillSetri jobsNo ratings yet
- Brandenton FL SpecDocument4 pagesBrandenton FL Specstevenlantigua95No ratings yet
- Important Billing Information Enclosed: Contact UsDocument40 pagesImportant Billing Information Enclosed: Contact UsJoseph GlaserNo ratings yet
- Florida Driver License and Identification Card: 2D Barcode Reader Calibration Sheet - 2016 AAMVA StandardDocument2 pagesFlorida Driver License and Identification Card: 2D Barcode Reader Calibration Sheet - 2016 AAMVA StandardNestor MartinezNo ratings yet
- CFSB FIXNOOK Sep-Feb 24Document7 pagesCFSB FIXNOOK Sep-Feb 24DjibzlaeNo ratings yet
- Dec BillDocument12 pagesDec BillDestiny SmithNo ratings yet
- 2017 Toyota Highlander Limited - Limited PlatinumDocument4 pages2017 Toyota Highlander Limited - Limited PlatinumGeorge ZabarasNo ratings yet
- Fay Bellas CK Stub 3Document1 pageFay Bellas CK Stub 3donerightsvcs100% (3)
- Revised Auto QuoteDocument3 pagesRevised Auto Quotesreek7red7aNo ratings yet
- State of New Jersey Department of The Treasury Unclaimed Property Administration P. O. Box 214 Trenton, NJ 08625Document3 pagesState of New Jersey Department of The Treasury Unclaimed Property Administration P. O. Box 214 Trenton, NJ 08625Tommy GraceNo ratings yet
- Sprint AgreementDocument4 pagesSprint AgreementAnonymous RadSWG3kyNo ratings yet
- Inity - L Nity M I I Re Trol M: When YouDocument2 pagesInity - L Nity M I I Re Trol M: When YouBrandon CallahanNo ratings yet
- Homepo NTDocument1 pageHomepo NTMissa RoseNo ratings yet
- GeicoDocument2 pagesGeicotfuyuicgufgyu5469No ratings yet
- PDF Statement DetailsDocument2 pagesPDF Statement Detailsluzmaria140190No ratings yet
- This Study Resource Was: Ontrack Billing Details Your Electric Usage ProfileDocument2 pagesThis Study Resource Was: Ontrack Billing Details Your Electric Usage ProfileJohn BeanNo ratings yet
- US Bank StatementDocument3 pagesUS Bank StatementAundy loveNo ratings yet
- Comerica E Statement 1 PDFDocument5 pagesComerica E Statement 1 PDFJonathan Seagull LivingstonNo ratings yet
- Insurance CardDocument1 pageInsurance Cardspurlock90No ratings yet
- Root Declarations Page 20210916Document4 pagesRoot Declarations Page 20210916SMART CHOICE AUTO GROUPNo ratings yet
- Practice Test 2017-2020: N F M C F T TDocument6 pagesPractice Test 2017-2020: N F M C F T TSMART CHOICE AUTO GROUPNo ratings yet
- Practice Test 2017-2020: N F M C F T TDocument6 pagesPractice Test 2017-2020: N F M C F T TSMART CHOICE AUTO GROUPNo ratings yet
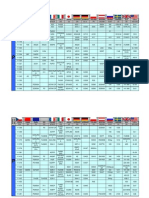
- Time Table:-"Warm Up" Classes Senior Secondary SESSION 2023-24 DATE: 24/03/2023 Venue: B.D.M.I. Milestone Building (P2) TIMING: 7:00 Am - 10:30 AmDocument1 pageTime Table:-"Warm Up" Classes Senior Secondary SESSION 2023-24 DATE: 24/03/2023 Venue: B.D.M.I. Milestone Building (P2) TIMING: 7:00 Am - 10:30 AmSREEJEETA SAHANo ratings yet
- Edu 2019 4229 en t012Document431 pagesEdu 2019 4229 en t012NicolásNo ratings yet
- The Economist 0912Document346 pagesThe Economist 0912Riaz kingNo ratings yet
- Session 5. MDGs and SDGsDocument30 pagesSession 5. MDGs and SDGsJen EspinaNo ratings yet
- Akash GST PPT NEWDocument15 pagesAkash GST PPT NEWAkash GuptaNo ratings yet
- A MateriauDocument29 pagesA MateriaubeforeRGNo ratings yet
- Gold InvestmentDocument4 pagesGold InvestmentvinitclairNo ratings yet
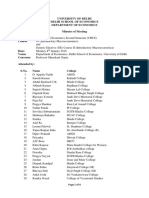
- Revised B.A.Hons - CBCS 2nd Sem. Introductory Macroeconomics GE II Intro. MacDocument4 pagesRevised B.A.Hons - CBCS 2nd Sem. Introductory Macroeconomics GE II Intro. MacHarshit KumarNo ratings yet
- 8820 Depol617 Political Processes in IndiaDocument148 pages8820 Depol617 Political Processes in IndiaRathin ChopraNo ratings yet
- ACT 410 Financial Statement Analysis: Week 2Document35 pagesACT 410 Financial Statement Analysis: Week 2zubaidzamanNo ratings yet
- INSPIRA JOURNAL OF MODERN MANAGEMENT ENTREPRENEURSHIPJMME Vol 08 N0 02 APRIL 2018 Pages 230 To 234Document5 pagesINSPIRA JOURNAL OF MODERN MANAGEMENT ENTREPRENEURSHIPJMME Vol 08 N0 02 APRIL 2018 Pages 230 To 234Manish RohillaNo ratings yet
- Tma 1 EconomicsDocument4 pagesTma 1 Economicsjojo labrinth OliverNo ratings yet
- Arx Malbikunarvaltarar Fra AmmannDocument24 pagesArx Malbikunarvaltarar Fra AmmannhathamphanNo ratings yet
- Rice Milling Report December 16Document23 pagesRice Milling Report December 16Niranjanreddy PuduruNo ratings yet
- Jurnal Anuva Desa GemawangDocument8 pagesJurnal Anuva Desa GemawangBudi SetyawanNo ratings yet
- Karwa Letter 4Document19 pagesKarwa Letter 4Samyak DahaleNo ratings yet
- Banking Audit Practice Guide IDocument118 pagesBanking Audit Practice Guide ISyed RizviNo ratings yet
- The Magic of ZonesDocument7 pagesThe Magic of ZonesAmilcar RivasNo ratings yet
- Od 226071629388983000Document1 pageOd 226071629388983000Sukhpal SinghNo ratings yet
- CIR v. Bank of Commerce (2005) Case DigestDocument2 pagesCIR v. Bank of Commerce (2005) Case DigestShandrei GuevarraNo ratings yet
- Form of Application For Registration of A Public TrustDocument4 pagesForm of Application For Registration of A Public Trustiqbalshaikh1960100% (1)
- 3 FILIPINOzam PDFDocument18 pages3 FILIPINOzam PDFPhilBoardResultsNo ratings yet
- Eir March2021Document1,475 pagesEir March2021Ashutosh BhandekarNo ratings yet
- Managerial Accounting Session 1Document15 pagesManagerial Accounting Session 1cathlenerosetalibgosNo ratings yet
- Aptitude Test 2 AnswersDocument5 pagesAptitude Test 2 AnswersTrung PhạmNo ratings yet
- Topic 3-NIEDocument36 pagesTopic 3-NIEAin ShafikahNo ratings yet
- 3 Cause List As On 06.04.2021Document6 pages3 Cause List As On 06.04.2021Vbs ReddyNo ratings yet
- 06 Assessmentof CO2 EmissionsandcostinflyashconcreteDocument5 pages06 Assessmentof CO2 EmissionsandcostinflyashconcreteshifatNo ratings yet
- 57121-Article Text-177864-1-10-20221011Document10 pages57121-Article Text-177864-1-10-20221011EstefaniaNo ratings yet