Download as pdf or txt
You might also like
- First Aid For The Medicine Clerkship Fourth Edition Kaufman Full ChapterDocument66 pagesFirst Aid For The Medicine Clerkship Fourth Edition Kaufman Full Chapterfelix.atkinson425100% (14)
- Ayurvedic Psychotherapy - Uncrypted PDFDocument152 pagesAyurvedic Psychotherapy - Uncrypted PDFDada DragicNo ratings yet
- Paediatric History and Examination 08092012-2Document10 pagesPaediatric History and Examination 08092012-2Shahin KazemzadehNo ratings yet
- Manovikaras With Special Reference To Udvega (Anxiety) and Vishada (Depression)Document7 pagesManovikaras With Special Reference To Udvega (Anxiety) and Vishada (Depression)suhas MNo ratings yet
- Ayurveda Based Advocacy For Mental HealthDocument8 pagesAyurveda Based Advocacy For Mental Healthrowena.singh2017No ratings yet
- Ayurveda Chikithsa - Mental DisorderDocument2 pagesAyurveda Chikithsa - Mental DisorderShenali Nadeesha0% (1)
- Glimpse of Mental Disorders and Treatment in AyurvedaDocument8 pagesGlimpse of Mental Disorders and Treatment in AyurvedaAnon0123100% (1)
- Manasa Tattva and Its Chikitsa Siddhanta ExplaineDocument4 pagesManasa Tattva and Its Chikitsa Siddhanta ExplaineYajush RaoNo ratings yet
- Mental Disorders in AyurvedaDocument32 pagesMental Disorders in Ayurvedaडा. सत्यदेव त्यागी आर्य50% (2)
- Manasika Roga ChikitsaDocument4 pagesManasika Roga ChikitsaReshma rajNo ratings yet
- Apasmara PaperDocument4 pagesApasmara PaperSamhitha Ayurvedic ChennaiNo ratings yet
- Daiva Vyapashrya ChikitsaDocument4 pagesDaiva Vyapashrya ChikitsaDr. Pavitra MalikNo ratings yet
- Journal Homepage: - : IntroductionDocument6 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- ASpectrumof Psychoactive Drugsin AyurvedaDocument5 pagesASpectrumof Psychoactive Drugsin AyurvedaUPINDERJIT SINGHNo ratings yet
- Ayurvedic Formulations For The Management of PsychDocument5 pagesAyurvedic Formulations For The Management of PsychShaktha Anand NathNo ratings yet
- A Review of Bhramari Pranayamas Impact On MentalDocument4 pagesA Review of Bhramari Pranayamas Impact On Mentala1120005No ratings yet
- Following Table Gives A List of Popular Naimitika RasayanaDocument17 pagesFollowing Table Gives A List of Popular Naimitika RasayanaKanjarla Hanmonthrao Panthulu LaxmanaNo ratings yet
- Satwavajaya Chikitsa in Ayurveda and Its Utility in ChikitsaDocument14 pagesSatwavajaya Chikitsa in Ayurveda and Its Utility in ChikitsaBhagyesha RasalNo ratings yet
- 473-Article Text-1455-1-10-20161206 PDFDocument4 pages473-Article Text-1455-1-10-20161206 PDFmadhuri pcNo ratings yet
- Management of Anxiety in Unani Medicine - A ReviewDocument4 pagesManagement of Anxiety in Unani Medicine - A ReviewDr M RajaramNo ratings yet
- Psychiatry in AyurvedaDocument5 pagesPsychiatry in AyurvedaabhinandanashNo ratings yet
- A Literature Review On Rasayana in Geriatric Mental Health CareDocument4 pagesA Literature Review On Rasayana in Geriatric Mental Health CareIJAR JOURNALNo ratings yet
- The Concept of Psychotherapy in Ayurveda With Special Reference To SatvavajayaDocument9 pagesThe Concept of Psychotherapy in Ayurveda With Special Reference To SatvavajayaMatt AldridgeNo ratings yet
- The Concept of Manas in Ayurveda - A Holistic Approach To Mental WellbeingDocument10 pagesThe Concept of Manas in Ayurveda - A Holistic Approach To Mental WellbeingpreethpadmanabhannambiarNo ratings yet
- Manovikara in AyurvedaDocument13 pagesManovikara in Ayurvedatihomiho100% (1)
- Anurag WJPR MentalHealthDocument10 pagesAnurag WJPR MentalHealthMadhura Pushpa kumaraNo ratings yet
- Ayurvedic Psychotherapy Uncrypted PDFDocument152 pagesAyurvedic Psychotherapy Uncrypted PDFAvinash AdhangleNo ratings yet
- Concept of Psychosomatic Disorders in Ayurveda PDFDocument5 pagesConcept of Psychosomatic Disorders in Ayurveda PDFNinaBudziszewskaNo ratings yet
- Ayurvedic Concept of Rasayan TherapyDocument14 pagesAyurvedic Concept of Rasayan TherapyKanjarla Hanmonthrao Panthulu Laxmana100% (1)
- S: Alternative System of Health & Complementary Therapies: Eminar OnDocument111 pagesS: Alternative System of Health & Complementary Therapies: Eminar OnMonika shankarNo ratings yet
- Ayurvedic PsychiatryDocument5 pagesAyurvedic PsychiatryabhinandanashNo ratings yet
- 676-Article Text-1373-1-10-20210423Document11 pages676-Article Text-1373-1-10-20210423Tania ChandraNo ratings yet
- S: Alternative System of Health & Complementary Therapies: Eminar OnDocument111 pagesS: Alternative System of Health & Complementary Therapies: Eminar OnMonika shankarNo ratings yet
- 1823 PDFDocument4 pages1823 PDFSruthikunaparajuNo ratings yet
- Spiritual Ayush - 5118173Document5 pagesSpiritual Ayush - 5118173marvel mNo ratings yet
- AYURVEDADocument4 pagesAYURVEDASelena CookNo ratings yet
- UnmadaaDocument34 pagesUnmadaaArathi laxman100% (1)
- KayaDocument5 pagesKayaPathik Nira YogaNo ratings yet
- 300-Article Text-1071-1-10-20160305Document5 pages300-Article Text-1071-1-10-20160305Sruthi Lal KrishnaNo ratings yet
- Shirodhara in Psycho DisordersDocument9 pagesShirodhara in Psycho DisordersOlga RodriguesNo ratings yet
- Mental IllnessDocument22 pagesMental Illnesssfgfg2100% (1)
- Multidimensional Effects of Shirodhara On Psycho-Somatic Axis in The Management of Psycho-Physiological DisordersDocument9 pagesMultidimensional Effects of Shirodhara On Psycho-Somatic Axis in The Management of Psycho-Physiological DisordersMatt AldridgeNo ratings yet
- Philosophy in The Interpretation of The Science of Ayurveda - Raghavan ThirumulpadDocument10 pagesPhilosophy in The Interpretation of The Science of Ayurveda - Raghavan Thirumulpaddr_saketram6146100% (1)
- Rejuvination BakuchiDocument12 pagesRejuvination BakuchiAmbesh jhaNo ratings yet
- Cam 4TH SeminarDocument54 pagesCam 4TH SeminarJisha JanardhanNo ratings yet
- Alternative and Complementary System in Health and TherapiesDocument48 pagesAlternative and Complementary System in Health and TherapiesDurga Charan Pradhan67% (3)
- 871 BookDocument4 pages871 Bookmurty99No ratings yet
- 252 1 828 1 10 20170711Document10 pages252 1 828 1 10 20170711MSKCNo ratings yet
- Therapeutic Formulations of Nasya in Charak SamhitaDocument7 pagesTherapeutic Formulations of Nasya in Charak SamhitacantuscantusNo ratings yet
- On The Effectiveness of Ayurvedic Medical Treatment Humoural Pharmacology, Positivistic Science, and Soteriology - Maarten BodeDocument24 pagesOn The Effectiveness of Ayurvedic Medical Treatment Humoural Pharmacology, Positivistic Science, and Soteriology - Maarten BodesadabrjNo ratings yet
- Effect of Vedic Mantra Treatment in Reduction of Depressive Syndrome and AnxietyDocument4 pagesEffect of Vedic Mantra Treatment in Reduction of Depressive Syndrome and AnxietymaninagaNo ratings yet
- A Handbook On Ayurvedic Intranasal Drug Therapy: Nasya Karma ChikitsaFrom EverandA Handbook On Ayurvedic Intranasal Drug Therapy: Nasya Karma ChikitsaRating: 3.5 out of 5 stars3.5/5 (3)
- GSM Alternative and Complemantary TherapiesDocument98 pagesGSM Alternative and Complemantary TherapiesMonika shankarNo ratings yet
- Ashwagandha As Anti-StressDocument9 pagesAshwagandha As Anti-StressAlna TechnicalNo ratings yet
- AYURVEDADocument20 pagesAYURVEDAAnkit KainNo ratings yet
- Ayurvedic PharmacologyandherbalmedicinesDocument7 pagesAyurvedic PharmacologyandherbalmedicinesBhavana GangurdeNo ratings yet
- 1882-Article Text-3908-2-10-20220717Document7 pages1882-Article Text-3908-2-10-20220717DrVivek JogNo ratings yet
- Ayush Content MatterDocument12 pagesAyush Content MatterJEEJANo ratings yet
- Ayurveda and Geriatric CareDocument56 pagesAyurveda and Geriatric CareCYBERPHARMNo ratings yet
- RasayanaDocument11 pagesRasayanaRajesh Nanoo100% (1)
- Ayurveda 101: Ayurveda Basics for The Absolute Beginner [Achieve Natural Health and Well Being through Ayurveda]From EverandAyurveda 101: Ayurveda Basics for The Absolute Beginner [Achieve Natural Health and Well Being through Ayurveda]Rating: 4 out of 5 stars4/5 (25)
- NSTP QUIZ - Feb. 14, 2022 - Google FormsDocument3 pagesNSTP QUIZ - Feb. 14, 2022 - Google FormsDarlene De PazNo ratings yet
- Victims of Charity / Animal ExperimentsDocument48 pagesVictims of Charity / Animal ExperimentsVegan FutureNo ratings yet
- Impact Factor of JournalsDocument227 pagesImpact Factor of Journalsalexpharm50% (2)
- Taboga Chiara - PainDocument2 pagesTaboga Chiara - PainAntea AssociazioneNo ratings yet
- OSU Orthopaedics Accomplishments Report 2010Document32 pagesOSU Orthopaedics Accomplishments Report 2010osuorthopaedicsNo ratings yet
- TramadolDocument2 pagesTramadoldwightciderNo ratings yet
- NCP Elective (Impaired Skin Integrity)Document1 pageNCP Elective (Impaired Skin Integrity)student_019No ratings yet
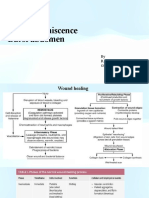
- Wound Dehiscence Burst Abdomen: by R.V.Kalyani Gen Surgery V UnitDocument25 pagesWound Dehiscence Burst Abdomen: by R.V.Kalyani Gen Surgery V Unitvinitha kattaNo ratings yet
- Gastroesophageal Reflux Disease: What Is LES?Document3 pagesGastroesophageal Reflux Disease: What Is LES?Irish Eunice Felix100% (1)
- 2011 Veterinary Vaccinesand Their Importanceto Animal Healthand Public HealthDocument11 pages2011 Veterinary Vaccinesand Their Importanceto Animal Healthand Public HealthCARLOTA DIAZ AGUILARNo ratings yet
- The Treatment and Management of Selfharm in Emergency Departments Slide Set Powerpoint 189897661Document41 pagesThe Treatment and Management of Selfharm in Emergency Departments Slide Set Powerpoint 189897661Zorbey TurkalpNo ratings yet
- PublicationsDocument23 pagesPublicationssahoosanjib48No ratings yet
- Midterm - Chapter 7Document6 pagesMidterm - Chapter 7mark OrpillaNo ratings yet
- Shy BookletDocument28 pagesShy BookletDesmond ScottNo ratings yet
- Different Physiotherapy Protocols After Coronary Artery Bypass Graft Surgery: A Randomized Controlled TrialDocument8 pagesDifferent Physiotherapy Protocols After Coronary Artery Bypass Graft Surgery: A Randomized Controlled Trialratnayanti udinNo ratings yet
- Case-Scenario No. 2 Ectopic-PregnancyDocument2 pagesCase-Scenario No. 2 Ectopic-PregnancyJoegie ArioNo ratings yet
- Create That Demand - Website SpecsDocument8 pagesCreate That Demand - Website SpecsRoshan KumarNo ratings yet
- Chapter 16: Breastfeeding Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument4 pagesChapter 16: Breastfeeding Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Bpharm Sem 6 Biopharm Ques PaperDocument3 pagesBpharm Sem 6 Biopharm Ques PaperNavam KumarNo ratings yet
- Practical Clinical Pharmacy II - Lab. 5Document3 pagesPractical Clinical Pharmacy II - Lab. 5Ali AbrahimNo ratings yet
- Torsio Testis FDHDocument21 pagesTorsio Testis FDHDwiyanti OktaviaNo ratings yet
- Tugas Lapsus Dentine-Hypersensitivity-A-ReviewDocument7 pagesTugas Lapsus Dentine-Hypersensitivity-A-ReviewSyifa MedikaNo ratings yet
- ICU As High Reliability OrganizationDocument66 pagesICU As High Reliability OrganizationRakhatiar TiarNo ratings yet
- Kayleigh M Gifford Resume UpdatedDocument2 pagesKayleigh M Gifford Resume Updatedapi-498468880No ratings yet
- SucralfateDocument10 pagesSucralfateherlika gustineNo ratings yet
- A Case of Myocardial Bridging: Marco Guglielmo, MD, Feacvi, FSCCTDocument23 pagesA Case of Myocardial Bridging: Marco Guglielmo, MD, Feacvi, FSCCTRaul CincaNo ratings yet
- Electrocardiograph Y (ECG / Ekg) : Rose Dyane F - Nunag, RMT, MPHDocument52 pagesElectrocardiograph Y (ECG / Ekg) : Rose Dyane F - Nunag, RMT, MPHClaire GonoNo ratings yet
- Kahoot (1) MergedDocument8 pagesKahoot (1) MergedNathaly MoraNo ratings yet





























































![Ayurveda 101: Ayurveda Basics for The Absolute Beginner [Achieve Natural Health and Well Being through Ayurveda]](https://imgv2-1-f.scribdassets.com/img/word_document/249204336/149x198/b6d9971e91/1718637513?v=1)