
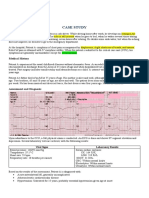
Acute Anterior Wall Myocardial Infarction
Acute Anterior Wall Myocardial Infarction
You might also like
- Inotropes and Vasoconstictor PackageDocument25 pagesInotropes and Vasoconstictor PackageYoussef MokdadNo ratings yet
- Final Examination Managerial EconomicsDocument2 pagesFinal Examination Managerial EconomicsMelinda Cariño BallonNo ratings yet
- NCM 107 Learning Packet On Related Learning Experience Rle Focus Unit: Care For High-Risk PregnancyDocument7 pagesNCM 107 Learning Packet On Related Learning Experience Rle Focus Unit: Care For High-Risk PregnancyMelinda Cariño BallonNo ratings yet
- Etruscan DictionaryDocument23 pagesEtruscan DictionaryHakki YazganNo ratings yet
- Angina PectorisDocument8 pagesAngina PectorisJoanne LagusadNo ratings yet
- Pulmonary ComplicationsDocument45 pagesPulmonary Complicationskyla arachelleNo ratings yet
- NCP Chest PainDocument2 pagesNCP Chest PainLinsae Troy50% (2)
- Activity 5Document4 pagesActivity 5AngieNo ratings yet
- Angina PectorisDocument4 pagesAngina PectorisJohiarra Madanglog TabigneNo ratings yet
- PericarditisDocument3 pagesPericarditisececasselNo ratings yet
- NCP Chest PainDocument2 pagesNCP Chest PainCG Patron BamboNo ratings yet
- Acute Coronary SyndromeDocument27 pagesAcute Coronary SyndromeSahr Anne Pilar B. ParreñoNo ratings yet
- Heart - CaDocument313 pagesHeart - Cafrenee aradanasNo ratings yet
- IM Cardiology Samplex All-In - LDocument35 pagesIM Cardiology Samplex All-In - LDeepbluexNo ratings yet
- Anesthetic Management of A Patient of Valvular Heart Disease Posted For Inguinal Hernioplasty A Case ReportDocument3 pagesAnesthetic Management of A Patient of Valvular Heart Disease Posted For Inguinal Hernioplasty A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Medip, IJAM-724 CDocument3 pagesMedip, IJAM-724 CKhalilSemlaliNo ratings yet
- Coronary Artery Disease Cvs 2 Es 1 1230806172121287 1 1Document30 pagesCoronary Artery Disease Cvs 2 Es 1 1230806172121287 1 1sara rababahNo ratings yet
- Abc Lec NotesDocument5 pagesAbc Lec NoteshanhananicasNo ratings yet
- Myocardial InfarctionDocument1 pageMyocardial InfarctionjljoioiuNo ratings yet
- (Antianginal Agents) Pharmacology Ass. Pabello Angelica S. BSN-2B 1946115Document9 pages(Antianginal Agents) Pharmacology Ass. Pabello Angelica S. BSN-2B 1946115Angelica PabelloNo ratings yet
- Angina PectorisDocument45 pagesAngina PectorisClarisse Biagtan CerameNo ratings yet
- ECG WorksheetDocument4 pagesECG WorksheetNikki GuisonNo ratings yet
- Concept Map For Anterior Myocardial Infarction: I. Introduction and ObjectivesDocument6 pagesConcept Map For Anterior Myocardial Infarction: I. Introduction and ObjectivesLouise GudmalinNo ratings yet
- Hypovolemic Shock: Dr. Sherwin BuluranDocument8 pagesHypovolemic Shock: Dr. Sherwin BuluranChristian UretaNo ratings yet
- 50 Emergency DrugsDocument70 pages50 Emergency DrugsderizNo ratings yet
- OxytocinDocument2 pagesOxytocinshefawNo ratings yet
- Short Cardic TabDocument4 pagesShort Cardic TabthackeryuktaNo ratings yet
- Cardio CH 27 NotesDocument8 pagesCardio CH 27 NotesMonica JubaneNo ratings yet
- Jam IsolaDocument11 pagesJam IsolaCAMOMILLE ROSE JAMISOLANo ratings yet
- Emmergency MedicineDocument48 pagesEmmergency MedicineSherein HagrasNo ratings yet
- Drug Study ORDocument3 pagesDrug Study ORIvan Jules P. PALMARESNo ratings yet
- DAY 6 SHOCK StudentsDocument38 pagesDAY 6 SHOCK StudentsTrisha UmaliNo ratings yet
- Cardiorespiratory Arrest (FS)Document55 pagesCardiorespiratory Arrest (FS)Ahmad AzharNo ratings yet
- Congestive Heart Failure and Pulmonary Edema: Nursing Diagnoses InterventionsDocument1 pageCongestive Heart Failure and Pulmonary Edema: Nursing Diagnoses InterventionsLovely CacapitNo ratings yet
- 15) Stable AnginaDocument3 pages15) Stable AnginaAris PaparisNo ratings yet
- Case Study With ECG Reading OcañaDocument3 pagesCase Study With ECG Reading OcañaNicole Chloe OcanaNo ratings yet
- Pericardial DiseasesDocument28 pagesPericardial DiseasesVrushali DNo ratings yet
- Pedia Cardio Lecture AidDocument5 pagesPedia Cardio Lecture AidStephanie Pearl AldaNo ratings yet
- Cardiac Exercise TableDocument16 pagesCardiac Exercise TablePreet KaurNo ratings yet
- 1.assignment On CPRDocument7 pages1.assignment On CPRsantosh kumarNo ratings yet
- Hypovolemic Shock Neurogenic ShockDocument40 pagesHypovolemic Shock Neurogenic ShockWemslaiNo ratings yet
- Haas 2008Document4 pagesHaas 2008Ana CortezNo ratings yet
- 401 ReviewerDocument30 pages401 ReviewerSheryl Anne GonzagaNo ratings yet
- CVS1 - K25 - Cardiac EmergencyDocument34 pagesCVS1 - K25 - Cardiac EmergencyAdmin neuro-usu.idNo ratings yet
- Hematologic Acute or Chronic Problems: ScenarioDocument36 pagesHematologic Acute or Chronic Problems: Scenariobhavana100% (1)
- Tatalaksana Sindroma Koroner Akut (Acute Coronary Syndrome)Document48 pagesTatalaksana Sindroma Koroner Akut (Acute Coronary Syndrome)Andrey ParhusipNo ratings yet
- AnesthesiaDocument8 pagesAnesthesiaYavani KulasinghamNo ratings yet
- Circulation AssessmentDocument8 pagesCirculation AssessmentalhassanmohamedNo ratings yet
- Journal Reading Acute Spinal Cord InjuryDocument14 pagesJournal Reading Acute Spinal Cord InjuryamandaNo ratings yet
- Cardiopulmonary ResuscitationDocument30 pagesCardiopulmonary ResuscitationAngel RituNo ratings yet
- Angina PectorisDocument19 pagesAngina PectorisRenas SalayNo ratings yet
- MYOCARDIAL INFARCTION EditedDocument27 pagesMYOCARDIAL INFARCTION Editedczars cajayonNo ratings yet
- Care of Clients With Physiologic and Psychosocial Alterations - Doc Version 1Document46 pagesCare of Clients With Physiologic and Psychosocial Alterations - Doc Version 1CLAIRE VillaviejaNo ratings yet
- Surgery Trauma - ShockDocument2 pagesSurgery Trauma - ShockyamaNo ratings yet
- MI SlidesDocument65 pagesMI SlidesJobelyn TunayNo ratings yet
- Acs - 12.01.2022Document41 pagesAcs - 12.01.2022SabariNo ratings yet
- Mi PresentationDocument65 pagesMi PresentationJobelyn TunayNo ratings yet
- Complications of Myocardial InfarctionDocument50 pagesComplications of Myocardial InfarctionAli Baker Algelane50% (2)
- Pericardial Effusion and Cardiac TamponadeDocument2 pagesPericardial Effusion and Cardiac TamponadeececasselNo ratings yet
- Cardiac Out Put NCPDocument3 pagesCardiac Out Put NCPTel EscorialNo ratings yet
- Concept Map MI 2Document1 pageConcept Map MI 2nicole barcenaNo ratings yet
- JurnalDocument4 pagesJurnalWaode Rifa AdhianiNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- 2021 - 2022 Tracheostomy Care ProcedureDocument69 pages2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNo ratings yet
- 2021 - 2022 Tracheostomy Care ProcedureDocument69 pages2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNo ratings yet
- Myocardial Infarction: - Mercy Grace DucusinDocument17 pagesMyocardial Infarction: - Mercy Grace DucusinMelinda Cariño BallonNo ratings yet
- Lecture 3: Sampling and Sample DistributionDocument30 pagesLecture 3: Sampling and Sample DistributionMelinda Cariño BallonNo ratings yet
- Urinary Interventions: By: Nursing Skills Laboratory GroupDocument57 pagesUrinary Interventions: By: Nursing Skills Laboratory GroupMelinda Cariño BallonNo ratings yet
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDocument3 pagesNursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceMelinda Cariño BallonNo ratings yet
- This Study Resource Was: Postpartum HemorrhageDocument2 pagesThis Study Resource Was: Postpartum HemorrhageMelinda Cariño BallonNo ratings yet
- Scope of Work (For 15 Working Days)Document2 pagesScope of Work (For 15 Working Days)Melinda Cariño BallonNo ratings yet
- KARDEXDocument2 pagesKARDEXMelinda Cariño BallonNo ratings yet
- NCM 107 Learning Packet On Related Learning Experience Rle Focus Unit: Care of NewbornDocument8 pagesNCM 107 Learning Packet On Related Learning Experience Rle Focus Unit: Care of NewbornMelinda Cariño BallonNo ratings yet
- Implications of Demographics of AgingDocument2 pagesImplications of Demographics of AgingMelinda Cariño BallonNo ratings yet
- Nurses' Notes: Patient Name: Age: Hospital No: Physician: Sex: Female Ward/Room: NicuDocument4 pagesNurses' Notes: Patient Name: Age: Hospital No: Physician: Sex: Female Ward/Room: NicuMelinda Cariño BallonNo ratings yet
- Drug Study-Ballon, Karlo C.Document5 pagesDrug Study-Ballon, Karlo C.Melinda Cariño BallonNo ratings yet
- NCM 109 LP RLE On HIGH RISK FOR PEDIATRIC CASE 1Document7 pagesNCM 109 LP RLE On HIGH RISK FOR PEDIATRIC CASE 1Melinda Cariño BallonNo ratings yet
- Journal Analysis-BALLON, Karlo CDocument4 pagesJournal Analysis-BALLON, Karlo CMelinda Cariño BallonNo ratings yet
- Autism: Assessment Diagnostic ManagementDocument1 pageAutism: Assessment Diagnostic ManagementMelinda Cariño BallonNo ratings yet
- Case Study Physiologic Changes in pregnancy-BALLON, KARLO C.Document3 pagesCase Study Physiologic Changes in pregnancy-BALLON, KARLO C.Melinda Cariño BallonNo ratings yet
- Sodium Bicarbonate Drug StudyDocument2 pagesSodium Bicarbonate Drug StudyMelinda Cariño BallonNo ratings yet
- This Study Resource Was Shared ViaDocument6 pagesThis Study Resource Was Shared ViaMelinda Cariño BallonNo ratings yet
- Journal Analysis-BALLON, Karlo CDocument4 pagesJournal Analysis-BALLON, Karlo CMelinda Cariño BallonNo ratings yet
- Reaction-paper-NURSE-INFORMATICS-ROLE - BALLON, KARLO C.Document2 pagesReaction-paper-NURSE-INFORMATICS-ROLE - BALLON, KARLO C.Melinda Cariño Ballon100% (1)
- DRUG-STUDY - BALLON, Karlo CDocument6 pagesDRUG-STUDY - BALLON, Karlo CMelinda Cariño BallonNo ratings yet
- Case Analaysis On infertility-BALLON-Karlo CDocument4 pagesCase Analaysis On infertility-BALLON-Karlo CMelinda Cariño BallonNo ratings yet
- Drug Study-Nifedipine-BALLON, Karlo C.Document2 pagesDrug Study-Nifedipine-BALLON, Karlo C.Melinda Cariño Ballon100% (1)
- Your Score: 100% (50/50) : CorrectDocument53 pagesYour Score: 100% (50/50) : CorrectMelinda Cariño BallonNo ratings yet
- M20 LatticeDocument30 pagesM20 LatticeKerwin Cley UgaleNo ratings yet
- Ignition Loss of Cured Reinforced Resins: Standard Test Method ForDocument3 pagesIgnition Loss of Cured Reinforced Resins: Standard Test Method ForElida SanchezNo ratings yet
- Wollo University: Kombolcha Institute of TechnologyDocument12 pagesWollo University: Kombolcha Institute of Technologymike workuNo ratings yet
- Lab 7 QUBE-Servo PD Control WorkbookDocument6 pagesLab 7 QUBE-Servo PD Control WorkbookLuis EnriquezNo ratings yet
- Hus3-C M8 Bolt For Brick WallDocument22 pagesHus3-C M8 Bolt For Brick WallANGEL MUÑOZNo ratings yet
- Stratified RocksDocument16 pagesStratified RocksJanuxie ParkNo ratings yet
- Unit Two. Dominant Theories Approaches: Positivism Rational Choice Theory MarxismDocument8 pagesUnit Two. Dominant Theories Approaches: Positivism Rational Choice Theory MarxismPaul RicoNo ratings yet
- Total Result 2594 Total Result 2583Document2,897 pagesTotal Result 2594 Total Result 2583anjali shilpa kajalNo ratings yet
- Are Urbanization, Industrialization and CO2 Emissions Cointegrated?Document30 pagesAre Urbanization, Industrialization and CO2 Emissions Cointegrated?doctshNo ratings yet
- Reimagine RTS Final ReportDocument88 pagesReimagine RTS Final ReportWXXI NewsNo ratings yet
- Urinary SystemDocument9 pagesUrinary SystemMary Joyce RamosNo ratings yet
- Real Analysis Problems - Cristian E. GutierrezDocument23 pagesReal Analysis Problems - Cristian E. GutierrezSanotestNo ratings yet
- Bending Stresses in BeamsDocument25 pagesBending Stresses in Beamsrajatapc12007No ratings yet
- Pathway - Skoliosis GROUPDocument12 pagesPathway - Skoliosis GROUPAnonymous NZTQVgjaNo ratings yet
- Fluid Mechanics PDFDocument48 pagesFluid Mechanics PDFrakib hasanNo ratings yet
- Our Own English High School, Sharjah Look Who'S Answering Quiz Club Group I (Grade 1) Question Bank - MAY 2019Document3 pagesOur Own English High School, Sharjah Look Who'S Answering Quiz Club Group I (Grade 1) Question Bank - MAY 2019Abimanyu ShenilNo ratings yet
- Comparison of The Ratios of Coca Cola and PepsiDocument6 pagesComparison of The Ratios of Coca Cola and PepsiassadullahNo ratings yet
- Research On Sustainable Development of Textile Industrial Clusters in The Process of GlobalizationDocument5 pagesResearch On Sustainable Development of Textile Industrial Clusters in The Process of GlobalizationSam AbdulNo ratings yet
- AppliedchemistrylabmaualDocument23 pagesAppliedchemistrylabmaualYashwanth KasthuriNo ratings yet
- Dorothy E. Johnson: Behavioral System ModelDocument15 pagesDorothy E. Johnson: Behavioral System Modelwickwax100% (1)
- Nuilding Acoustics Through Europe Volume 2Document572 pagesNuilding Acoustics Through Europe Volume 2salyNo ratings yet
- Three Dimensional GeometryDocument3 pagesThree Dimensional GeometryTaqi IsmailNo ratings yet
- Dissertation - Balancing Heritage and Contemporary ArchitectureDocument62 pagesDissertation - Balancing Heritage and Contemporary Architecturekavyagupta92100% (7)
- Motor Circuit Analysis For Energy, Reliability and Production Cost ImprovementsDocument4 pagesMotor Circuit Analysis For Energy, Reliability and Production Cost ImprovementsAmin Mustangin As-SalafyNo ratings yet
- IEE Checklist InstructionsDocument20 pagesIEE Checklist InstructionsBalaji_Rajaman_2280No ratings yet
- Logicalreasoning MockDocument11 pagesLogicalreasoning MockTarun GaurNo ratings yet
- ETABS Steel Frame Design: ETABS 20.3.0 License # 1844D8FY33V4ZNYDocument2 pagesETABS Steel Frame Design: ETABS 20.3.0 License # 1844D8FY33V4ZNYTravel DiariesNo ratings yet
- Caudal Duplication Syndrome-Report of A CaseDocument4 pagesCaudal Duplication Syndrome-Report of A Casekhumaira1982No ratings yet
- Metabolizam SeceraDocument52 pagesMetabolizam SeceraAnel RedzepiNo ratings yet



















































































































Download as docx, pdf, or txt
You might also like
- Inotropes and Vasoconstictor PackageDocument25 pagesInotropes and Vasoconstictor PackageYoussef MokdadNo ratings yet
- Final Examination Managerial EconomicsDocument2 pagesFinal Examination Managerial EconomicsMelinda Cariño BallonNo ratings yet
- NCM 107 Learning Packet On Related Learning Experience Rle Focus Unit: Care For High-Risk PregnancyDocument7 pagesNCM 107 Learning Packet On Related Learning Experience Rle Focus Unit: Care For High-Risk PregnancyMelinda Cariño BallonNo ratings yet
- Etruscan DictionaryDocument23 pagesEtruscan DictionaryHakki YazganNo ratings yet
- Angina PectorisDocument8 pagesAngina PectorisJoanne LagusadNo ratings yet
- Pulmonary ComplicationsDocument45 pagesPulmonary Complicationskyla arachelleNo ratings yet
- NCP Chest PainDocument2 pagesNCP Chest PainLinsae Troy50% (2)
- Activity 5Document4 pagesActivity 5AngieNo ratings yet
- Angina PectorisDocument4 pagesAngina PectorisJohiarra Madanglog TabigneNo ratings yet
- PericarditisDocument3 pagesPericarditisececasselNo ratings yet
- NCP Chest PainDocument2 pagesNCP Chest PainCG Patron BamboNo ratings yet
- Acute Coronary SyndromeDocument27 pagesAcute Coronary SyndromeSahr Anne Pilar B. ParreñoNo ratings yet
- Heart - CaDocument313 pagesHeart - Cafrenee aradanasNo ratings yet
- IM Cardiology Samplex All-In - LDocument35 pagesIM Cardiology Samplex All-In - LDeepbluexNo ratings yet
- Anesthetic Management of A Patient of Valvular Heart Disease Posted For Inguinal Hernioplasty A Case ReportDocument3 pagesAnesthetic Management of A Patient of Valvular Heart Disease Posted For Inguinal Hernioplasty A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Medip, IJAM-724 CDocument3 pagesMedip, IJAM-724 CKhalilSemlaliNo ratings yet
- Coronary Artery Disease Cvs 2 Es 1 1230806172121287 1 1Document30 pagesCoronary Artery Disease Cvs 2 Es 1 1230806172121287 1 1sara rababahNo ratings yet
- Abc Lec NotesDocument5 pagesAbc Lec NoteshanhananicasNo ratings yet
- Myocardial InfarctionDocument1 pageMyocardial InfarctionjljoioiuNo ratings yet
- (Antianginal Agents) Pharmacology Ass. Pabello Angelica S. BSN-2B 1946115Document9 pages(Antianginal Agents) Pharmacology Ass. Pabello Angelica S. BSN-2B 1946115Angelica PabelloNo ratings yet
- Angina PectorisDocument45 pagesAngina PectorisClarisse Biagtan CerameNo ratings yet
- ECG WorksheetDocument4 pagesECG WorksheetNikki GuisonNo ratings yet
- Concept Map For Anterior Myocardial Infarction: I. Introduction and ObjectivesDocument6 pagesConcept Map For Anterior Myocardial Infarction: I. Introduction and ObjectivesLouise GudmalinNo ratings yet
- Hypovolemic Shock: Dr. Sherwin BuluranDocument8 pagesHypovolemic Shock: Dr. Sherwin BuluranChristian UretaNo ratings yet
- 50 Emergency DrugsDocument70 pages50 Emergency DrugsderizNo ratings yet
- OxytocinDocument2 pagesOxytocinshefawNo ratings yet
- Short Cardic TabDocument4 pagesShort Cardic TabthackeryuktaNo ratings yet
- Cardio CH 27 NotesDocument8 pagesCardio CH 27 NotesMonica JubaneNo ratings yet
- Jam IsolaDocument11 pagesJam IsolaCAMOMILLE ROSE JAMISOLANo ratings yet
- Emmergency MedicineDocument48 pagesEmmergency MedicineSherein HagrasNo ratings yet
- Drug Study ORDocument3 pagesDrug Study ORIvan Jules P. PALMARESNo ratings yet
- DAY 6 SHOCK StudentsDocument38 pagesDAY 6 SHOCK StudentsTrisha UmaliNo ratings yet
- Cardiorespiratory Arrest (FS)Document55 pagesCardiorespiratory Arrest (FS)Ahmad AzharNo ratings yet
- Congestive Heart Failure and Pulmonary Edema: Nursing Diagnoses InterventionsDocument1 pageCongestive Heart Failure and Pulmonary Edema: Nursing Diagnoses InterventionsLovely CacapitNo ratings yet
- 15) Stable AnginaDocument3 pages15) Stable AnginaAris PaparisNo ratings yet
- Case Study With ECG Reading OcañaDocument3 pagesCase Study With ECG Reading OcañaNicole Chloe OcanaNo ratings yet
- Pericardial DiseasesDocument28 pagesPericardial DiseasesVrushali DNo ratings yet
- Pedia Cardio Lecture AidDocument5 pagesPedia Cardio Lecture AidStephanie Pearl AldaNo ratings yet
- Cardiac Exercise TableDocument16 pagesCardiac Exercise TablePreet KaurNo ratings yet
- 1.assignment On CPRDocument7 pages1.assignment On CPRsantosh kumarNo ratings yet
- Hypovolemic Shock Neurogenic ShockDocument40 pagesHypovolemic Shock Neurogenic ShockWemslaiNo ratings yet
- Haas 2008Document4 pagesHaas 2008Ana CortezNo ratings yet
- 401 ReviewerDocument30 pages401 ReviewerSheryl Anne GonzagaNo ratings yet
- CVS1 - K25 - Cardiac EmergencyDocument34 pagesCVS1 - K25 - Cardiac EmergencyAdmin neuro-usu.idNo ratings yet
- Hematologic Acute or Chronic Problems: ScenarioDocument36 pagesHematologic Acute or Chronic Problems: Scenariobhavana100% (1)
- Tatalaksana Sindroma Koroner Akut (Acute Coronary Syndrome)Document48 pagesTatalaksana Sindroma Koroner Akut (Acute Coronary Syndrome)Andrey ParhusipNo ratings yet
- AnesthesiaDocument8 pagesAnesthesiaYavani KulasinghamNo ratings yet
- Circulation AssessmentDocument8 pagesCirculation AssessmentalhassanmohamedNo ratings yet
- Journal Reading Acute Spinal Cord InjuryDocument14 pagesJournal Reading Acute Spinal Cord InjuryamandaNo ratings yet
- Cardiopulmonary ResuscitationDocument30 pagesCardiopulmonary ResuscitationAngel RituNo ratings yet
- Angina PectorisDocument19 pagesAngina PectorisRenas SalayNo ratings yet
- MYOCARDIAL INFARCTION EditedDocument27 pagesMYOCARDIAL INFARCTION Editedczars cajayonNo ratings yet
- Care of Clients With Physiologic and Psychosocial Alterations - Doc Version 1Document46 pagesCare of Clients With Physiologic and Psychosocial Alterations - Doc Version 1CLAIRE VillaviejaNo ratings yet
- Surgery Trauma - ShockDocument2 pagesSurgery Trauma - ShockyamaNo ratings yet
- MI SlidesDocument65 pagesMI SlidesJobelyn TunayNo ratings yet
- Acs - 12.01.2022Document41 pagesAcs - 12.01.2022SabariNo ratings yet
- Mi PresentationDocument65 pagesMi PresentationJobelyn TunayNo ratings yet
- Complications of Myocardial InfarctionDocument50 pagesComplications of Myocardial InfarctionAli Baker Algelane50% (2)
- Pericardial Effusion and Cardiac TamponadeDocument2 pagesPericardial Effusion and Cardiac TamponadeececasselNo ratings yet
- Cardiac Out Put NCPDocument3 pagesCardiac Out Put NCPTel EscorialNo ratings yet
- Concept Map MI 2Document1 pageConcept Map MI 2nicole barcenaNo ratings yet
- JurnalDocument4 pagesJurnalWaode Rifa AdhianiNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- 2021 - 2022 Tracheostomy Care ProcedureDocument69 pages2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNo ratings yet
- 2021 - 2022 Tracheostomy Care ProcedureDocument69 pages2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNo ratings yet
- Myocardial Infarction: - Mercy Grace DucusinDocument17 pagesMyocardial Infarction: - Mercy Grace DucusinMelinda Cariño BallonNo ratings yet
- Lecture 3: Sampling and Sample DistributionDocument30 pagesLecture 3: Sampling and Sample DistributionMelinda Cariño BallonNo ratings yet
- Urinary Interventions: By: Nursing Skills Laboratory GroupDocument57 pagesUrinary Interventions: By: Nursing Skills Laboratory GroupMelinda Cariño BallonNo ratings yet
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDocument3 pagesNursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceMelinda Cariño BallonNo ratings yet
- This Study Resource Was: Postpartum HemorrhageDocument2 pagesThis Study Resource Was: Postpartum HemorrhageMelinda Cariño BallonNo ratings yet
- Scope of Work (For 15 Working Days)Document2 pagesScope of Work (For 15 Working Days)Melinda Cariño BallonNo ratings yet
- KARDEXDocument2 pagesKARDEXMelinda Cariño BallonNo ratings yet
- NCM 107 Learning Packet On Related Learning Experience Rle Focus Unit: Care of NewbornDocument8 pagesNCM 107 Learning Packet On Related Learning Experience Rle Focus Unit: Care of NewbornMelinda Cariño BallonNo ratings yet
- Implications of Demographics of AgingDocument2 pagesImplications of Demographics of AgingMelinda Cariño BallonNo ratings yet
- Nurses' Notes: Patient Name: Age: Hospital No: Physician: Sex: Female Ward/Room: NicuDocument4 pagesNurses' Notes: Patient Name: Age: Hospital No: Physician: Sex: Female Ward/Room: NicuMelinda Cariño BallonNo ratings yet
- Drug Study-Ballon, Karlo C.Document5 pagesDrug Study-Ballon, Karlo C.Melinda Cariño BallonNo ratings yet
- NCM 109 LP RLE On HIGH RISK FOR PEDIATRIC CASE 1Document7 pagesNCM 109 LP RLE On HIGH RISK FOR PEDIATRIC CASE 1Melinda Cariño BallonNo ratings yet
- Journal Analysis-BALLON, Karlo CDocument4 pagesJournal Analysis-BALLON, Karlo CMelinda Cariño BallonNo ratings yet
- Autism: Assessment Diagnostic ManagementDocument1 pageAutism: Assessment Diagnostic ManagementMelinda Cariño BallonNo ratings yet
- Case Study Physiologic Changes in pregnancy-BALLON, KARLO C.Document3 pagesCase Study Physiologic Changes in pregnancy-BALLON, KARLO C.Melinda Cariño BallonNo ratings yet
- Sodium Bicarbonate Drug StudyDocument2 pagesSodium Bicarbonate Drug StudyMelinda Cariño BallonNo ratings yet
- This Study Resource Was Shared ViaDocument6 pagesThis Study Resource Was Shared ViaMelinda Cariño BallonNo ratings yet
- Journal Analysis-BALLON, Karlo CDocument4 pagesJournal Analysis-BALLON, Karlo CMelinda Cariño BallonNo ratings yet
- Reaction-paper-NURSE-INFORMATICS-ROLE - BALLON, KARLO C.Document2 pagesReaction-paper-NURSE-INFORMATICS-ROLE - BALLON, KARLO C.Melinda Cariño Ballon100% (1)
- DRUG-STUDY - BALLON, Karlo CDocument6 pagesDRUG-STUDY - BALLON, Karlo CMelinda Cariño BallonNo ratings yet
- Case Analaysis On infertility-BALLON-Karlo CDocument4 pagesCase Analaysis On infertility-BALLON-Karlo CMelinda Cariño BallonNo ratings yet
- Drug Study-Nifedipine-BALLON, Karlo C.Document2 pagesDrug Study-Nifedipine-BALLON, Karlo C.Melinda Cariño Ballon100% (1)
- Your Score: 100% (50/50) : CorrectDocument53 pagesYour Score: 100% (50/50) : CorrectMelinda Cariño BallonNo ratings yet
- M20 LatticeDocument30 pagesM20 LatticeKerwin Cley UgaleNo ratings yet
- Ignition Loss of Cured Reinforced Resins: Standard Test Method ForDocument3 pagesIgnition Loss of Cured Reinforced Resins: Standard Test Method ForElida SanchezNo ratings yet
- Wollo University: Kombolcha Institute of TechnologyDocument12 pagesWollo University: Kombolcha Institute of Technologymike workuNo ratings yet
- Lab 7 QUBE-Servo PD Control WorkbookDocument6 pagesLab 7 QUBE-Servo PD Control WorkbookLuis EnriquezNo ratings yet
- Hus3-C M8 Bolt For Brick WallDocument22 pagesHus3-C M8 Bolt For Brick WallANGEL MUÑOZNo ratings yet
- Stratified RocksDocument16 pagesStratified RocksJanuxie ParkNo ratings yet
- Unit Two. Dominant Theories Approaches: Positivism Rational Choice Theory MarxismDocument8 pagesUnit Two. Dominant Theories Approaches: Positivism Rational Choice Theory MarxismPaul RicoNo ratings yet
- Total Result 2594 Total Result 2583Document2,897 pagesTotal Result 2594 Total Result 2583anjali shilpa kajalNo ratings yet
- Are Urbanization, Industrialization and CO2 Emissions Cointegrated?Document30 pagesAre Urbanization, Industrialization and CO2 Emissions Cointegrated?doctshNo ratings yet
- Reimagine RTS Final ReportDocument88 pagesReimagine RTS Final ReportWXXI NewsNo ratings yet
- Urinary SystemDocument9 pagesUrinary SystemMary Joyce RamosNo ratings yet
- Real Analysis Problems - Cristian E. GutierrezDocument23 pagesReal Analysis Problems - Cristian E. GutierrezSanotestNo ratings yet
- Bending Stresses in BeamsDocument25 pagesBending Stresses in Beamsrajatapc12007No ratings yet
- Pathway - Skoliosis GROUPDocument12 pagesPathway - Skoliosis GROUPAnonymous NZTQVgjaNo ratings yet
- Fluid Mechanics PDFDocument48 pagesFluid Mechanics PDFrakib hasanNo ratings yet
- Our Own English High School, Sharjah Look Who'S Answering Quiz Club Group I (Grade 1) Question Bank - MAY 2019Document3 pagesOur Own English High School, Sharjah Look Who'S Answering Quiz Club Group I (Grade 1) Question Bank - MAY 2019Abimanyu ShenilNo ratings yet
- Comparison of The Ratios of Coca Cola and PepsiDocument6 pagesComparison of The Ratios of Coca Cola and PepsiassadullahNo ratings yet
- Research On Sustainable Development of Textile Industrial Clusters in The Process of GlobalizationDocument5 pagesResearch On Sustainable Development of Textile Industrial Clusters in The Process of GlobalizationSam AbdulNo ratings yet
- AppliedchemistrylabmaualDocument23 pagesAppliedchemistrylabmaualYashwanth KasthuriNo ratings yet
- Dorothy E. Johnson: Behavioral System ModelDocument15 pagesDorothy E. Johnson: Behavioral System Modelwickwax100% (1)
- Nuilding Acoustics Through Europe Volume 2Document572 pagesNuilding Acoustics Through Europe Volume 2salyNo ratings yet
- Three Dimensional GeometryDocument3 pagesThree Dimensional GeometryTaqi IsmailNo ratings yet
- Dissertation - Balancing Heritage and Contemporary ArchitectureDocument62 pagesDissertation - Balancing Heritage and Contemporary Architecturekavyagupta92100% (7)
- Motor Circuit Analysis For Energy, Reliability and Production Cost ImprovementsDocument4 pagesMotor Circuit Analysis For Energy, Reliability and Production Cost ImprovementsAmin Mustangin As-SalafyNo ratings yet
- IEE Checklist InstructionsDocument20 pagesIEE Checklist InstructionsBalaji_Rajaman_2280No ratings yet
- Logicalreasoning MockDocument11 pagesLogicalreasoning MockTarun GaurNo ratings yet
- ETABS Steel Frame Design: ETABS 20.3.0 License # 1844D8FY33V4ZNYDocument2 pagesETABS Steel Frame Design: ETABS 20.3.0 License # 1844D8FY33V4ZNYTravel DiariesNo ratings yet
- Caudal Duplication Syndrome-Report of A CaseDocument4 pagesCaudal Duplication Syndrome-Report of A Casekhumaira1982No ratings yet
- Metabolizam SeceraDocument52 pagesMetabolizam SeceraAnel RedzepiNo ratings yet