Download as pdf or txt
You might also like
- Emergency Nursing ExamDocument38 pagesEmergency Nursing Exammilayosores100% (5)
- HLTINF001 Student Assessment Task 1 - Questioning...Document10 pagesHLTINF001 Student Assessment Task 1 - Questioning...Muskan SohalNo ratings yet
- Drug Study - SalbutamolDocument2 pagesDrug Study - SalbutamolryanNo ratings yet
- Incompetent NCPDocument1 pageIncompetent NCPJohn Francis Velasco100% (6)
- Effect of A Novel Macrophage-Regulating Drug On Wound Healing in Patients With Diabetic Foot UlcersDocument13 pagesEffect of A Novel Macrophage-Regulating Drug On Wound Healing in Patients With Diabetic Foot Ulcers陳瑋毅No ratings yet
- Chen 2017Document10 pagesChen 2017Ranti AgustiniNo ratings yet
- SR Diabetic Foot UlcerDocument11 pagesSR Diabetic Foot UlcerDeka AdeNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleAsriyani HamidNo ratings yet
- Amputation Predictors in Diabetic Foot Ulcers Treated With Hyperbaric OxygenDocument4 pagesAmputation Predictors in Diabetic Foot Ulcers Treated With Hyperbaric OxygenRanti AgustiniNo ratings yet
- HHS Public Access: Update On Management of Diabetic Foot UlcersDocument19 pagesHHS Public Access: Update On Management of Diabetic Foot UlcersPUSKESMAS KECAMATAN KEPULAUAN SERIBU UTARANo ratings yet
- Acutepainmanagement: Nabil Moussa,, Orrett E. OgleDocument13 pagesAcutepainmanagement: Nabil Moussa,, Orrett E. OgleMahmoud AbouelsoudNo ratings yet
- Enteral1 PDFDocument10 pagesEnteral1 PDFCarlos Eduardo FerrazNo ratings yet
- Maggot Therapy For Treating Diabetic Foot Ulcers UDocument6 pagesMaggot Therapy For Treating Diabetic Foot Ulcers UBayu AdhityaNo ratings yet
- What Is The Best Pain Control After Major Hepato Pancreato Biliary SurgeryDocument15 pagesWhat Is The Best Pain Control After Major Hepato Pancreato Biliary Surgeryvalerio.messinaNo ratings yet
- Jowc 2020 29 Sup3 S13Document6 pagesJowc 2020 29 Sup3 S13LalaNo ratings yet
- NJS 25 14Document7 pagesNJS 25 14Rio RomaNo ratings yet
- A Comparative Study of Topical Phenytoin Vs Conventional Wound Care in Diabetic UlcerDocument6 pagesA Comparative Study of Topical Phenytoin Vs Conventional Wound Care in Diabetic UlcerIOSRjournalNo ratings yet
- Dor de Garganta BMJ EditorialDocument6 pagesDor de Garganta BMJ Editorialangela995No ratings yet
- Impact of Negative Pressure Wound Therapy in Complete Healing Rates Following Surgical Debridement in Heel and Ankle Regions in Diabetic Foot InfectionsDocument6 pagesImpact of Negative Pressure Wound Therapy in Complete Healing Rates Following Surgical Debridement in Heel and Ankle Regions in Diabetic Foot InfectionsZven BlackNo ratings yet
- The Routes of Administration For Acute Postoperative Pain MedicationDocument17 pagesThe Routes of Administration For Acute Postoperative Pain Medicationronald97hgNo ratings yet
- Internasional 2Document5 pagesInternasional 2Srimaya TampubolonNo ratings yet
- Injectableagentsversus Surgeryforrecurrent Temporomandibularjoint DislocationDocument7 pagesInjectableagentsversus Surgeryforrecurrent Temporomandibularjoint Dislocationmehak malhotraNo ratings yet
- Desmoid Type Tumor DOX JapanDocument8 pagesDesmoid Type Tumor DOX JapanAgung PriyonoNo ratings yet
- Greene & Manfredini 2023 - Overtreatment Successes - 230709 - 135204Document11 pagesGreene & Manfredini 2023 - Overtreatment Successes - 230709 - 135204Abigail HernándezNo ratings yet
- Overcoming Barriers To Patient Adherence: The Case For Developing Innovative Drug Delivery SystemsDocument23 pagesOvercoming Barriers To Patient Adherence: The Case For Developing Innovative Drug Delivery SystemsscribdNo ratings yet
- Wound 2021 0016Document21 pagesWound 2021 0016Ronel ResurricionNo ratings yet
- E001758 FullDocument24 pagesE001758 FullsarlecakestreakNo ratings yet
- 215768-Article Text-531860-1-10-20211010Document7 pages215768-Article Text-531860-1-10-20211010Rio RomaNo ratings yet
- Diabetic Foot Infection: Antibiotic Therapy and Good Practice RecommendationsDocument10 pagesDiabetic Foot Infection: Antibiotic Therapy and Good Practice RecommendationsjessicaNo ratings yet
- Malek Pour Alam Dari 2021Document5 pagesMalek Pour Alam Dari 2021Rio RomaNo ratings yet
- Opiod RotationDocument9 pagesOpiod RotationboboNo ratings yet
- BiocellulosaDocument4 pagesBiocellulosadesi mitraNo ratings yet
- Research Open Access: Dina Yehia Kassim, Hatem Elmoutaz Mahmoud, Dina Mahmoud Fakhry and Mariana Abdelsayed MansourDocument10 pagesResearch Open Access: Dina Yehia Kassim, Hatem Elmoutaz Mahmoud, Dina Mahmoud Fakhry and Mariana Abdelsayed MansourIda Ayu Apsari P NNo ratings yet
- Maggot Debridement Therapy For Diabetic Foot Ulcer: Experience From Maggot Treatment Centers Http://ajpp - InDocument4 pagesMaggot Debridement Therapy For Diabetic Foot Ulcer: Experience From Maggot Treatment Centers Http://ajpp - InOsmela PutriNo ratings yet
- Cba 2Document2 pagesCba 2Najib Al FatinNo ratings yet
- The Effect of A Mhealth Intervention On.7Document5 pagesThe Effect of A Mhealth Intervention On.7Aula reciNo ratings yet
- Wound Care Management in Indonesia Issues and Challenges in Diabetic Foot Ulceration PDFDocument5 pagesWound Care Management in Indonesia Issues and Challenges in Diabetic Foot Ulceration PDFlinda jurwitaNo ratings yet
- Hypertonic Dextrose (Prolotherapy)Document8 pagesHypertonic Dextrose (Prolotherapy)RensoBerlangaNo ratings yet
- Pathogenesis and Management of Fracture-Related InfectionDocument7 pagesPathogenesis and Management of Fracture-Related InfectionJeremi SetiawanNo ratings yet
- PR 2021 Cureus 13-1-E12870 1-9Document9 pagesPR 2021 Cureus 13-1-E12870 1-9aditya galih wicaksonoNo ratings yet
- 2022.abdoli AOVE Diabetic FootDocument7 pages2022.abdoli AOVE Diabetic Footv8w7g2xyjcNo ratings yet
- Outcomes of 207 Totally Extraperitoneal Hernia Repairs Using Self Fixation MeshDocument8 pagesOutcomes of 207 Totally Extraperitoneal Hernia Repairs Using Self Fixation Mesha kNo ratings yet
- Therapeutic Drug Monitoring of Biologics For Patients With Inflammatory Bowel Diseases: How, When, and For Whom?Document10 pagesTherapeutic Drug Monitoring of Biologics For Patients With Inflammatory Bowel Diseases: How, When, and For Whom?paula costa LeandroNo ratings yet
- Stratmann 2020 Oi 200419 1601302160.02426Document12 pagesStratmann 2020 Oi 200419 1601302160.02426Laís LimaNo ratings yet
- FX de CaderaDocument11 pagesFX de CaderaJuan Carlos Perez ParadaNo ratings yet
- 593 FullDocument3 pages593 FullEka Setyorini .A.No ratings yet
- Manejo Pte Diabetico IopDocument11 pagesManejo Pte Diabetico Iopheiddy MendozaNo ratings yet
- Preoperative Assessment and Perioperative Management in Oesophageal and Gastric SurgeryDocument16 pagesPreoperative Assessment and Perioperative Management in Oesophageal and Gastric SurgeryLuis FelipeNo ratings yet
- Opioid-Free Versus Opioid-Based Anesthesia in Pancreatic Surgery BMC Anest. 2022Document9 pagesOpioid-Free Versus Opioid-Based Anesthesia in Pancreatic Surgery BMC Anest. 2022valerio.messinaNo ratings yet
- Benefits and Risks of Dexamethasone in Noncardiac SurgeryDocument9 pagesBenefits and Risks of Dexamethasone in Noncardiac SurgeryHenry Gabriel HarderNo ratings yet
- Case Studies Evaluation Using Advanced Wound Dressings in The Local Management of Diabetic Foot Ulcers PDFDocument24 pagesCase Studies Evaluation Using Advanced Wound Dressings in The Local Management of Diabetic Foot Ulcers PDFKalbornozQuintulNo ratings yet
- FDG PET - CT-based Response AssessmentDocument17 pagesFDG PET - CT-based Response AssessmentHelen MejiaNo ratings yet
- A Prospective Observational Multi Centre Study On The Use of Negative Pressure Wound Therapy in Diabetic Foot UlcerDocument7 pagesA Prospective Observational Multi Centre Study On The Use of Negative Pressure Wound Therapy in Diabetic Foot UlcerHerald Scholarly Open AccessNo ratings yet
- LidocainaDocument7 pagesLidocainaDaniel Alejandro GrecoNo ratings yet
- Nyas 14440Document11 pagesNyas 14440Willian HolandaNo ratings yet
- Outcomes of Management of Recurrent Dupuytren Contracture: A Systematic Review and Meta-AnalysisDocument10 pagesOutcomes of Management of Recurrent Dupuytren Contracture: A Systematic Review and Meta-Analysissadaka.mohamedNo ratings yet
- Jco 19 02192Document11 pagesJco 19 02192giovanni nuñez nuñezNo ratings yet
- Iwj 12097Document6 pagesIwj 12097Asriyani HamidNo ratings yet
- PIIS0007091220305663Document13 pagesPIIS0007091220305663Ana Belén Artero CastañoNo ratings yet
- BJAEd - Analgesia For Caesarean SectionDocument7 pagesBJAEd - Analgesia For Caesarean SectionDragos IonixNo ratings yet
- Skube 2018Document5 pagesSkube 2018RafaelNo ratings yet
- PDF TestDocument15 pagesPDF TestJess BaerNo ratings yet
- Infusion Therapy: For Pain, Headache and Related ConditionsFrom EverandInfusion Therapy: For Pain, Headache and Related ConditionsAlaa Abd-ElsayedNo ratings yet
- Speech and Language Therapy For Aphasia Following Subacute StrokeDocument4 pagesSpeech and Language Therapy For Aphasia Following Subacute StrokeRanti AgustiniNo ratings yet
- Efficacy of Intensive Aphasia Therapy in Patients With Chronic Stroke: A Randomised Controlled TrialDocument7 pagesEfficacy of Intensive Aphasia Therapy in Patients With Chronic Stroke: A Randomised Controlled TrialRanti AgustiniNo ratings yet
- Chen 2017Document10 pagesChen 2017Ranti AgustiniNo ratings yet
- Articles: BackgroundDocument11 pagesArticles: BackgroundRanti AgustiniNo ratings yet
- THELANCET D 16 06318R1 As Accepted 01.11.2016Document59 pagesTHELANCET D 16 06318R1 As Accepted 01.11.2016Ranti AgustiniNo ratings yet
- CD000425Document315 pagesCD000425Ranti AgustiniNo ratings yet
- What Speech and Language Therapy Do Community Dwelling Stroke Survivors With Aphasia Receive in The UK?Document20 pagesWhat Speech and Language Therapy Do Community Dwelling Stroke Survivors With Aphasia Receive in The UK?Ranti AgustiniNo ratings yet
- Template JKG 2021Document5 pagesTemplate JKG 2021Ranti AgustiniNo ratings yet
- The Open Cardiovascular Medicine JournalDocument6 pagesThe Open Cardiovascular Medicine JournalRanti AgustiniNo ratings yet
- Amputation Predictors in Diabetic Foot Ulcers Treated With Hyperbaric OxygenDocument4 pagesAmputation Predictors in Diabetic Foot Ulcers Treated With Hyperbaric OxygenRanti AgustiniNo ratings yet
- Topical Oxygen Therapy Promotes The Healing of Chronic Diabetic Foot Ulcers: A Pilot StudyDocument7 pagesTopical Oxygen Therapy Promotes The Healing of Chronic Diabetic Foot Ulcers: A Pilot StudyRanti AgustiniNo ratings yet
- Ontario Health Technology Assessment SeriesDocument142 pagesOntario Health Technology Assessment SeriesRanti AgustiniNo ratings yet
- 2020 Article 4757Document6 pages2020 Article 4757Ranti AgustiniNo ratings yet
- Name: Ranti Agustini Class: Psik 3CDocument3 pagesName: Ranti Agustini Class: Psik 3CRanti AgustiniNo ratings yet
- Impact of Hyperbaric Oxygen On More Advanced Wagner Grades 3 and 4 Diabetic Foot Ulcers: Matching Therapy To Specific Wound ConditionsDocument11 pagesImpact of Hyperbaric Oxygen On More Advanced Wagner Grades 3 and 4 Diabetic Foot Ulcers: Matching Therapy To Specific Wound ConditionsRanti AgustiniNo ratings yet
- Taenia SoliumDocument44 pagesTaenia SoliumRanti AgustiniNo ratings yet
- Causes and Effects of Stress: Name:Ranti Agustini NIM: 21117098 Class: PSIK 3CDocument2 pagesCauses and Effects of Stress: Name:Ranti Agustini NIM: 21117098 Class: PSIK 3CRanti AgustiniNo ratings yet
- Relationship Between Flood and Infectious Diseases BackgroundDocument1 pageRelationship Between Flood and Infectious Diseases BackgroundRanti AgustiniNo ratings yet
- Relationship Between Flood and Infectious Diseases BackgroundDocument1 pageRelationship Between Flood and Infectious Diseases BackgroundRanti AgustiniNo ratings yet
- PSPD AnswerDocument4 pagesPSPD Answercinocag595No ratings yet
- Annexure-A Form No 2 UCO Bank Application For Commutation of Pension Subject To Medical Examination. (To Be Submitted in Duplicate) Part-IDocument7 pagesAnnexure-A Form No 2 UCO Bank Application For Commutation of Pension Subject To Medical Examination. (To Be Submitted in Duplicate) Part-Ipranav11No ratings yet
- Chanca Piedra: Kidney Stones BreakerDocument2 pagesChanca Piedra: Kidney Stones BreakerIfechukwu U. IbemeNo ratings yet
- Java Script 2Document50 pagesJava Script 2ashishkumar140806No ratings yet
- Fetal CirculationDocument4 pagesFetal CirculationNishaThakuriNo ratings yet
- Outpatient Programs - Adult Rehabilitation Island HealthDocument8 pagesOutpatient Programs - Adult Rehabilitation Island HealthCorey Jay ParkerNo ratings yet
- Sleep Medicine in Critical CareDocument335 pagesSleep Medicine in Critical CareDragutin PetrićNo ratings yet
- Heart Failure in The Last Year: Progress and Perspective: Journal ReadingDocument31 pagesHeart Failure in The Last Year: Progress and Perspective: Journal ReadingIkmah FauzanNo ratings yet
- CV AgtDocument6 pagesCV AgtHafzhy TravelNo ratings yet
- Brainstorming: Unit 1: Basic Classifications of Addictive SubstanceDocument9 pagesBrainstorming: Unit 1: Basic Classifications of Addictive SubstanceJamie MedallaNo ratings yet
- Injury Prevention, Safety, and First AidDocument20 pagesInjury Prevention, Safety, and First AidAprille Maye CayogNo ratings yet
- Health ChecklistDocument1 pageHealth ChecklistMelba BarcelNo ratings yet
- Lung Function TestingDocument217 pagesLung Function TestingMazurencoIana100% (2)
- Kidneys and Kidney DiseaseDocument32 pagesKidneys and Kidney DiseaseAbdullah Bin SaeedNo ratings yet
- Cues/Needs Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective Data: IndependentDocument2 pagesCues/Needs Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective Data: IndependentArabelle GONo ratings yet
- What Are The Core Elements of PCC A Narrative ReviewDocument12 pagesWhat Are The Core Elements of PCC A Narrative ReviewDario SanabriaNo ratings yet
- DR Shaukat Khan ResumeDocument4 pagesDR Shaukat Khan ResumeShaukat KhanNo ratings yet
- BK3 Greatest FearDocument4 pagesBK3 Greatest FearMaxine TaeyeonNo ratings yet
- PPT Case NephrolithiasisDocument45 pagesPPT Case NephrolithiasisRifka Anisa0% (1)
- Group 2 - Siloam Hospital - 2Document31 pagesGroup 2 - Siloam Hospital - 2Byu PALEMBANGNo ratings yet
- 1 of 1 - My Health SummaryDocument210 pages1 of 1 - My Health SummaryCandace DeihlNo ratings yet
- UTI Practicum Make-Up Assignment FINALDocument8 pagesUTI Practicum Make-Up Assignment FINALlmstar98No ratings yet
- Texila American University: Case Report FormatDocument7 pagesTexila American University: Case Report FormatShahzad AhmadNo ratings yet
- ASPAK Alkes IGDDocument2 pagesASPAK Alkes IGDAdra AdeNo ratings yet
- Subject Type of Exam Exam Date Number of Groups: Medical Chemistry Online. WRITTENDocument12 pagesSubject Type of Exam Exam Date Number of Groups: Medical Chemistry Online. WRITTENEhsan TariqNo ratings yet
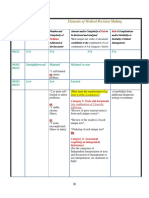
- 3-Level of MDMDocument3 pages3-Level of MDMmedical codingNo ratings yet