
Embolic Stroke of Undetermined Source: A Systematic Review and Clinical Update
Embolic Stroke of Undetermined Source: A Systematic Review and Clinical Update
You might also like
- Show: Bunheads By: Amy Sherman-Palladino Scene Type: Serio-Comic Character: BooDocument17 pagesShow: Bunheads By: Amy Sherman-Palladino Scene Type: Serio-Comic Character: BooChristina CannillaNo ratings yet
- Science Yearly Lesson Plan Form 2Document10 pagesScience Yearly Lesson Plan Form 2NorelyanaAli100% (2)
- 10 1001@jamaneurol 2019 0591Document7 pages10 1001@jamaneurol 2019 0591Suryati HusinNo ratings yet
- Bhat Et Al 2021 Embolic Stroke of Undetermined Source Approaches in Risk Stratification For CardioembolismDocument17 pagesBhat Et Al 2021 Embolic Stroke of Undetermined Source Approaches in Risk Stratification For CardioembolismSuryati HusinNo ratings yet
- Jamaneurology Topcuoglu 2017 Oi 170047Document8 pagesJamaneurology Topcuoglu 2017 Oi 170047LadycherryNo ratings yet
- 6 Antithrombotic Therapy in Patients With Infective EndocarditisDocument12 pages6 Antithrombotic Therapy in Patients With Infective Endocarditisabdeali hazariNo ratings yet
- Different Clinical Phenotypes of Embolic Stroke of Undetermined Source: A Subgroup Analysis of 86 PatientsDocument9 pagesDifferent Clinical Phenotypes of Embolic Stroke of Undetermined Source: A Subgroup Analysis of 86 PatientsSuryati HusinNo ratings yet
- Anticoagulacion Temprana Vs Tardia en ACV Con FADocument11 pagesAnticoagulacion Temprana Vs Tardia en ACV Con FACesar Mauricio Daza CajasNo ratings yet
- 525 FullDocument5 pages525 FullmluthfidunandNo ratings yet
- Rory Hachamovitch, MD, MSC Sean W. Hayes, MD John D. Friedman, MD Ishac Cohen, PHD Daniel S. Berman, MDDocument8 pagesRory Hachamovitch, MD, MSC Sean W. Hayes, MD John D. Friedman, MD Ishac Cohen, PHD Daniel S. Berman, MDFarah SukmanaNo ratings yet
- Update Managemant Unrupture Aneurysm 2018Document8 pagesUpdate Managemant Unrupture Aneurysm 2018Mikha ManurungNo ratings yet
- ICA'sDocument37 pagesICA'sVeronica TanNo ratings yet
- Kamiya Matsuoka2017Document5 pagesKamiya Matsuoka2017Jasper CubiasNo ratings yet
- Early Versus Later Anticoagulation For Stroke With Atrial FibrillationDocument11 pagesEarly Versus Later Anticoagulation For Stroke With Atrial Fibrillationguille.1492No ratings yet
- Trial of Endovascular Thrombectomy For Large Ischemic StrokesDocument13 pagesTrial of Endovascular Thrombectomy For Large Ischemic StrokesMABEL LUCERO OLARTE JURADONo ratings yet
- Sharma Et Al 2021 Frequency and Patterns of Brain Infarction in Patients With Embolic Stroke of Undetermined SourceDocument8 pagesSharma Et Al 2021 Frequency and Patterns of Brain Infarction in Patients With Embolic Stroke of Undetermined SourceSuryati HusinNo ratings yet
- BMJ 2023 077848.fullDocument12 pagesBMJ 2023 077848.fullfilhosvaldpNo ratings yet
- Acute DizzinessDocument14 pagesAcute DizzinesstsyrahmaniNo ratings yet
- PVC and Risk of CVDNHDocument13 pagesPVC and Risk of CVDNHDenny IntanNo ratings yet
- A Newelectrocardiographic Pattern Indicating Inferior Myocardial InfarctionDocument6 pagesA Newelectrocardiographic Pattern Indicating Inferior Myocardial InfarctionOswaldo OrtizNo ratings yet
- Cardiogenic Shock in Children 2024Document14 pagesCardiogenic Shock in Children 2024Pediatrician Suhail NaikNo ratings yet
- Symptomatic Non-Stenotic Carotid Disease: Current Challenges and Opportunities For Diagnosis and TreatmentDocument8 pagesSymptomatic Non-Stenotic Carotid Disease: Current Challenges and Opportunities For Diagnosis and Treatmentsnzbtk8df9No ratings yet
- Strokeaha 111 622175Document6 pagesStrokeaha 111 622175Ivan PradhanaNo ratings yet
- Comment: Vs 1 7% of 261 Patients With Atrial TachyarrhythmiasDocument2 pagesComment: Vs 1 7% of 261 Patients With Atrial TachyarrhythmiasDewina Dyani Rosari IINo ratings yet
- Acv Criptogenico Neurol Clin Pract-2016-Bartolini-271-6Document7 pagesAcv Criptogenico Neurol Clin Pract-2016-Bartolini-271-6FedericoNo ratings yet
- Apixaban Vs ASA en Ictus Embólico de Fuente IndeterminadaDocument12 pagesApixaban Vs ASA en Ictus Embólico de Fuente IndeterminadaOscar SantosNo ratings yet
- 1371 FullDocument9 pages1371 Fullyogithajeganathan5197No ratings yet
- Ejemplo1 Tabla1Document12 pagesEjemplo1 Tabla1Isabel MartNo ratings yet
- Smash-U: A Proposal For Etiologic Classification of Intracerebral HemorrhageDocument6 pagesSmash-U: A Proposal For Etiologic Classification of Intracerebral HemorrhageIulian EnacheNo ratings yet
- 1 s2.0 S0929664620302163 MainDocument14 pages1 s2.0 S0929664620302163 MainSuryati HusinNo ratings yet
- Risk Factors of Dysphagia in Patients With Ischemic Stroke - A Meta-Analysis and Systematic ReviewDocument14 pagesRisk Factors of Dysphagia in Patients With Ischemic Stroke - A Meta-Analysis and Systematic ReviewAlexandreNo ratings yet
- Review Articles: A Systematic Review On Internal Jugular Vein Thrombosis and Pulmonary EmbolismDocument5 pagesReview Articles: A Systematic Review On Internal Jugular Vein Thrombosis and Pulmonary EmbolismdevaNo ratings yet
- 01 STR 29 1 251Document6 pages01 STR 29 1 251RAFAEL BRITONo ratings yet
- Clinical Neurology and NeurosurgeryDocument6 pagesClinical Neurology and NeurosurgeryNurul Azmi Rosmala PutriNo ratings yet
- Open Questions in Acute Stroke Management and Stroke PreventionDocument2 pagesOpen Questions in Acute Stroke Management and Stroke PreventionMazin Al-TahirNo ratings yet
- AHA/ASA Scientific StatementDocument19 pagesAHA/ASA Scientific StatementMeidianie CamelliaNo ratings yet
- Capsulotomia y Riesgo de Nav en Desplazamiento de Epifisis de Cabeza Femoral Inestable, Metanalisis 2019Document6 pagesCapsulotomia y Riesgo de Nav en Desplazamiento de Epifisis de Cabeza Femoral Inestable, Metanalisis 2019Daniel Cancino CallirgosNo ratings yet
- WASID Trial 2005Document12 pagesWASID Trial 2005cristhian_carvaja_13No ratings yet
- J JCMG 2022 06 015Document12 pagesJ JCMG 2022 06 015Jhon Alexis M ArgoteNo ratings yet
- More Expansive Horizons - A Review of Endovascular Therapy For Patients With Low NIHSS ScoresDocument7 pagesMore Expansive Horizons - A Review of Endovascular Therapy For Patients With Low NIHSS ScoresVictor M TorresNo ratings yet
- CCMED Chief HRV AnalysisDocument2 pagesCCMED Chief HRV AnalysisdonsuniNo ratings yet
- Rivaroxavan en Fa ValvularDocument5 pagesRivaroxavan en Fa Valvularcarlos pardoNo ratings yet
- Anticoagulant in Atrial Fibrillation Patients With Prior IntracranialDocument7 pagesAnticoagulant in Atrial Fibrillation Patients With Prior IntracranialWilliam BarreraNo ratings yet
- Meta-Analysis of Fragmented QRS As An Electrocardiographic Predictor For Arrhythmic Events in Patients With Brugada SyndromeDocument7 pagesMeta-Analysis of Fragmented QRS As An Electrocardiographic Predictor For Arrhythmic Events in Patients With Brugada SyndromeAndonis AngelovNo ratings yet
- JRMS 17 396Document6 pagesJRMS 17 396fani rudiyantiNo ratings yet
- Cutting Ballon Combined With Drug Coated Balloon Angioplasty For The Treatment of In-Stent RestenosisDocument8 pagesCutting Ballon Combined With Drug Coated Balloon Angioplasty For The Treatment of In-Stent Restenosislia indria watiNo ratings yet
- Make Clipping Great Again: Microsurgery For Cerebral Aneurysms by Dual-Trained NeurosurgeonsDocument8 pagesMake Clipping Great Again: Microsurgery For Cerebral Aneurysms by Dual-Trained NeurosurgeonsJohnson SimatupangNo ratings yet
- Lumbar Spinal Stenosis: Syndrome, Diagnostics and Treatment: Nature Reviews Neurology August 2009Document13 pagesLumbar Spinal Stenosis: Syndrome, Diagnostics and Treatment: Nature Reviews Neurology August 2009Surya PangeranNo ratings yet
- Early Repolarization Pattern and Risk For Arrhythmia Death Meta AnalysisDocument6 pagesEarly Repolarization Pattern and Risk For Arrhythmia Death Meta Analysisfindingnemo667No ratings yet
- Continuous Determination of Optimal Cerebral Perfusion Pressure in Traumatic Brain InjuryDocument8 pagesContinuous Determination of Optimal Cerebral Perfusion Pressure in Traumatic Brain InjurydrdivyapukNo ratings yet
- Bateman2017Document6 pagesBateman2017Meris JugadorNo ratings yet
- Predictors of Outcome in AneurysmalDocument7 pagesPredictors of Outcome in AneurysmalNeni NirmalaNo ratings yet
- Seiffge 2018Document3 pagesSeiffge 2018barti koksNo ratings yet
- Cooper Et Al 2007 The Role of Endomyocardial Biopsy in The Management of Cardiovascular DiseaseDocument18 pagesCooper Et Al 2007 The Role of Endomyocardial Biopsy in The Management of Cardiovascular DiseaseEszter SzerencsiNo ratings yet
- Adult NCSE Power KN 2015Document5 pagesAdult NCSE Power KN 2015Hendra PermanaNo ratings yet
- Kwon Et Al 2020 Deep Learning Based Algorithm For Detecting Aortic Stenosis Using ElectrocardiographyDocument16 pagesKwon Et Al 2020 Deep Learning Based Algorithm For Detecting Aortic Stenosis Using Electrocardiography施展No ratings yet
- ToastDocument7 pagesToastallisonjramirezNo ratings yet
- Ankylosing SpondylitesDocument16 pagesAnkylosing SpondylitesJyotirmayeeNo ratings yet
- Clinical Neurology and NeurosurgeryDocument14 pagesClinical Neurology and NeurosurgeryabbbabbbNo ratings yet
- Jaha 119 013678Document18 pagesJaha 119 013678Bosman AriestaNo ratings yet
- Time Trends in Atrial Fibrillation-Associated Stroke and Premorbid AnticoagulationDocument7 pagesTime Trends in Atrial Fibrillation-Associated Stroke and Premorbid Anticoagulationmuhamad ibnu sinaNo ratings yet
- J LPM 2019 03 016 PDFDocument9 pagesJ LPM 2019 03 016 PDFDessytha NathaniaNo ratings yet
- A Modified Anatomical-Functional-Rope (Af-Rope) Score Improves Patient Selection For Patent Foramen Ovale ClosureDocument4 pagesA Modified Anatomical-Functional-Rope (Af-Rope) Score Improves Patient Selection For Patent Foramen Ovale ClosureDessytha NathaniaNo ratings yet
- Acute Rheumatic Fever Diagnosis and Management - Rhda Workshop March 2016 Brisbane - Final PDFDocument61 pagesAcute Rheumatic Fever Diagnosis and Management - Rhda Workshop March 2016 Brisbane - Final PDFDessytha NathaniaNo ratings yet
- JONESDocument61 pagesJONESDessytha NathaniaNo ratings yet
- Abdullah JavedDocument8 pagesAbdullah JavedTahir MahmoodNo ratings yet
- 1 Structural - FunctionalismDocument57 pages1 Structural - FunctionalismCinnamonNo ratings yet
- Hick's Law Lab 1Document6 pagesHick's Law Lab 1Merna SamieNo ratings yet
- 16.21.1814 EbookDocument442 pages16.21.1814 EbookSutadi Triputra100% (1)
- Im12a01f01 03enDocument95 pagesIm12a01f01 03enkjonasamNo ratings yet
- Webhunt Conor FoleyDocument3 pagesWebhunt Conor Foleyapi-367746310No ratings yet
- Challenges To IoT-Enabled Predictive Maintenance For Industry 4.0Document13 pagesChallenges To IoT-Enabled Predictive Maintenance For Industry 4.0BrunoNo ratings yet
- Selina Concise Physics Solutions Class 6 Chapter 1 MatterDocument22 pagesSelina Concise Physics Solutions Class 6 Chapter 1 MatterAltaf TalpurNo ratings yet
- RCA SystemLink3Document9 pagesRCA SystemLink3JerônimoNo ratings yet
- Lab. 12 NylonDocument4 pagesLab. 12 NyloncsnNo ratings yet
- Example The Inductance of A SolenoidDocument3 pagesExample The Inductance of A SolenoidMuhamad YusupNo ratings yet
- BlackBerry Wireless Headset HS 700 User Guide 1035096 0819052837 001 USDocument4 pagesBlackBerry Wireless Headset HS 700 User Guide 1035096 0819052837 001 USPopescu CristiNo ratings yet
- Experiment 1 FINALDocument12 pagesExperiment 1 FINALMaiSakurajimaNo ratings yet
- 02.1-WCDMA Basic Principle of Radio Propagation - 20051214Document20 pages02.1-WCDMA Basic Principle of Radio Propagation - 20051214kltowerNo ratings yet
- Happiness - Mark MansonDocument26 pagesHappiness - Mark MansonJake100% (3)
- Line Dance ModuleDocument34 pagesLine Dance ModuleMarie Antionette MondragonNo ratings yet
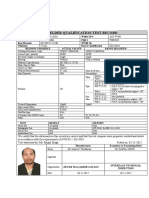
- Wqt-1-13-W-1-3g-Smaw-Alclad-Aws D1.1Document1 pageWqt-1-13-W-1-3g-Smaw-Alclad-Aws D1.1Rejoy babyNo ratings yet
- Infections PDFDocument29 pagesInfections PDFLoudry ElfaNo ratings yet
- NBRK0200 Installation Configuration ManualDocument32 pagesNBRK0200 Installation Configuration ManualGoran JovanovicNo ratings yet
- Anima Core BookDocument317 pagesAnima Core BookPeter HillaryNo ratings yet
- M45913-1 RevADocument4 pagesM45913-1 RevAMAI_QualityNo ratings yet
- Amniotic Fluid PDFDocument24 pagesAmniotic Fluid PDFJoshua Ty CayetanoNo ratings yet
- EW - European Whirl (Classic Trip)Document19 pagesEW - European Whirl (Classic Trip)Gabriele Di RivombrosaNo ratings yet
- Hotel Minimum ReqDocument28 pagesHotel Minimum ReqAnusha AshokNo ratings yet
- Text 1 (A & B)Document2 pagesText 1 (A & B)ifx leeNo ratings yet
- Poster PresentationDocument1 pagePoster PresentationPilla SatishNo ratings yet
- Measuring Your Carbon Footprint PowerPointDocument16 pagesMeasuring Your Carbon Footprint PowerPointpremquilonNo ratings yet
- Roblox Admins Free WorkingDocument483 pagesRoblox Admins Free WorkingCrazy SodaNo ratings yet





























































































Download as pdf or txt
You might also like
- Show: Bunheads By: Amy Sherman-Palladino Scene Type: Serio-Comic Character: BooDocument17 pagesShow: Bunheads By: Amy Sherman-Palladino Scene Type: Serio-Comic Character: BooChristina CannillaNo ratings yet
- Science Yearly Lesson Plan Form 2Document10 pagesScience Yearly Lesson Plan Form 2NorelyanaAli100% (2)
- 10 1001@jamaneurol 2019 0591Document7 pages10 1001@jamaneurol 2019 0591Suryati HusinNo ratings yet
- Bhat Et Al 2021 Embolic Stroke of Undetermined Source Approaches in Risk Stratification For CardioembolismDocument17 pagesBhat Et Al 2021 Embolic Stroke of Undetermined Source Approaches in Risk Stratification For CardioembolismSuryati HusinNo ratings yet
- Jamaneurology Topcuoglu 2017 Oi 170047Document8 pagesJamaneurology Topcuoglu 2017 Oi 170047LadycherryNo ratings yet
- 6 Antithrombotic Therapy in Patients With Infective EndocarditisDocument12 pages6 Antithrombotic Therapy in Patients With Infective Endocarditisabdeali hazariNo ratings yet
- Different Clinical Phenotypes of Embolic Stroke of Undetermined Source: A Subgroup Analysis of 86 PatientsDocument9 pagesDifferent Clinical Phenotypes of Embolic Stroke of Undetermined Source: A Subgroup Analysis of 86 PatientsSuryati HusinNo ratings yet
- Anticoagulacion Temprana Vs Tardia en ACV Con FADocument11 pagesAnticoagulacion Temprana Vs Tardia en ACV Con FACesar Mauricio Daza CajasNo ratings yet
- 525 FullDocument5 pages525 FullmluthfidunandNo ratings yet
- Rory Hachamovitch, MD, MSC Sean W. Hayes, MD John D. Friedman, MD Ishac Cohen, PHD Daniel S. Berman, MDDocument8 pagesRory Hachamovitch, MD, MSC Sean W. Hayes, MD John D. Friedman, MD Ishac Cohen, PHD Daniel S. Berman, MDFarah SukmanaNo ratings yet
- Update Managemant Unrupture Aneurysm 2018Document8 pagesUpdate Managemant Unrupture Aneurysm 2018Mikha ManurungNo ratings yet
- ICA'sDocument37 pagesICA'sVeronica TanNo ratings yet
- Kamiya Matsuoka2017Document5 pagesKamiya Matsuoka2017Jasper CubiasNo ratings yet
- Early Versus Later Anticoagulation For Stroke With Atrial FibrillationDocument11 pagesEarly Versus Later Anticoagulation For Stroke With Atrial Fibrillationguille.1492No ratings yet
- Trial of Endovascular Thrombectomy For Large Ischemic StrokesDocument13 pagesTrial of Endovascular Thrombectomy For Large Ischemic StrokesMABEL LUCERO OLARTE JURADONo ratings yet
- Sharma Et Al 2021 Frequency and Patterns of Brain Infarction in Patients With Embolic Stroke of Undetermined SourceDocument8 pagesSharma Et Al 2021 Frequency and Patterns of Brain Infarction in Patients With Embolic Stroke of Undetermined SourceSuryati HusinNo ratings yet
- BMJ 2023 077848.fullDocument12 pagesBMJ 2023 077848.fullfilhosvaldpNo ratings yet
- Acute DizzinessDocument14 pagesAcute DizzinesstsyrahmaniNo ratings yet
- PVC and Risk of CVDNHDocument13 pagesPVC and Risk of CVDNHDenny IntanNo ratings yet
- A Newelectrocardiographic Pattern Indicating Inferior Myocardial InfarctionDocument6 pagesA Newelectrocardiographic Pattern Indicating Inferior Myocardial InfarctionOswaldo OrtizNo ratings yet
- Cardiogenic Shock in Children 2024Document14 pagesCardiogenic Shock in Children 2024Pediatrician Suhail NaikNo ratings yet
- Symptomatic Non-Stenotic Carotid Disease: Current Challenges and Opportunities For Diagnosis and TreatmentDocument8 pagesSymptomatic Non-Stenotic Carotid Disease: Current Challenges and Opportunities For Diagnosis and Treatmentsnzbtk8df9No ratings yet
- Strokeaha 111 622175Document6 pagesStrokeaha 111 622175Ivan PradhanaNo ratings yet
- Comment: Vs 1 7% of 261 Patients With Atrial TachyarrhythmiasDocument2 pagesComment: Vs 1 7% of 261 Patients With Atrial TachyarrhythmiasDewina Dyani Rosari IINo ratings yet
- Acv Criptogenico Neurol Clin Pract-2016-Bartolini-271-6Document7 pagesAcv Criptogenico Neurol Clin Pract-2016-Bartolini-271-6FedericoNo ratings yet
- Apixaban Vs ASA en Ictus Embólico de Fuente IndeterminadaDocument12 pagesApixaban Vs ASA en Ictus Embólico de Fuente IndeterminadaOscar SantosNo ratings yet
- 1371 FullDocument9 pages1371 Fullyogithajeganathan5197No ratings yet
- Ejemplo1 Tabla1Document12 pagesEjemplo1 Tabla1Isabel MartNo ratings yet
- Smash-U: A Proposal For Etiologic Classification of Intracerebral HemorrhageDocument6 pagesSmash-U: A Proposal For Etiologic Classification of Intracerebral HemorrhageIulian EnacheNo ratings yet
- 1 s2.0 S0929664620302163 MainDocument14 pages1 s2.0 S0929664620302163 MainSuryati HusinNo ratings yet
- Risk Factors of Dysphagia in Patients With Ischemic Stroke - A Meta-Analysis and Systematic ReviewDocument14 pagesRisk Factors of Dysphagia in Patients With Ischemic Stroke - A Meta-Analysis and Systematic ReviewAlexandreNo ratings yet
- Review Articles: A Systematic Review On Internal Jugular Vein Thrombosis and Pulmonary EmbolismDocument5 pagesReview Articles: A Systematic Review On Internal Jugular Vein Thrombosis and Pulmonary EmbolismdevaNo ratings yet
- 01 STR 29 1 251Document6 pages01 STR 29 1 251RAFAEL BRITONo ratings yet
- Clinical Neurology and NeurosurgeryDocument6 pagesClinical Neurology and NeurosurgeryNurul Azmi Rosmala PutriNo ratings yet
- Open Questions in Acute Stroke Management and Stroke PreventionDocument2 pagesOpen Questions in Acute Stroke Management and Stroke PreventionMazin Al-TahirNo ratings yet
- AHA/ASA Scientific StatementDocument19 pagesAHA/ASA Scientific StatementMeidianie CamelliaNo ratings yet
- Capsulotomia y Riesgo de Nav en Desplazamiento de Epifisis de Cabeza Femoral Inestable, Metanalisis 2019Document6 pagesCapsulotomia y Riesgo de Nav en Desplazamiento de Epifisis de Cabeza Femoral Inestable, Metanalisis 2019Daniel Cancino CallirgosNo ratings yet
- WASID Trial 2005Document12 pagesWASID Trial 2005cristhian_carvaja_13No ratings yet
- J JCMG 2022 06 015Document12 pagesJ JCMG 2022 06 015Jhon Alexis M ArgoteNo ratings yet
- More Expansive Horizons - A Review of Endovascular Therapy For Patients With Low NIHSS ScoresDocument7 pagesMore Expansive Horizons - A Review of Endovascular Therapy For Patients With Low NIHSS ScoresVictor M TorresNo ratings yet
- CCMED Chief HRV AnalysisDocument2 pagesCCMED Chief HRV AnalysisdonsuniNo ratings yet
- Rivaroxavan en Fa ValvularDocument5 pagesRivaroxavan en Fa Valvularcarlos pardoNo ratings yet
- Anticoagulant in Atrial Fibrillation Patients With Prior IntracranialDocument7 pagesAnticoagulant in Atrial Fibrillation Patients With Prior IntracranialWilliam BarreraNo ratings yet
- Meta-Analysis of Fragmented QRS As An Electrocardiographic Predictor For Arrhythmic Events in Patients With Brugada SyndromeDocument7 pagesMeta-Analysis of Fragmented QRS As An Electrocardiographic Predictor For Arrhythmic Events in Patients With Brugada SyndromeAndonis AngelovNo ratings yet
- JRMS 17 396Document6 pagesJRMS 17 396fani rudiyantiNo ratings yet
- Cutting Ballon Combined With Drug Coated Balloon Angioplasty For The Treatment of In-Stent RestenosisDocument8 pagesCutting Ballon Combined With Drug Coated Balloon Angioplasty For The Treatment of In-Stent Restenosislia indria watiNo ratings yet
- Make Clipping Great Again: Microsurgery For Cerebral Aneurysms by Dual-Trained NeurosurgeonsDocument8 pagesMake Clipping Great Again: Microsurgery For Cerebral Aneurysms by Dual-Trained NeurosurgeonsJohnson SimatupangNo ratings yet
- Lumbar Spinal Stenosis: Syndrome, Diagnostics and Treatment: Nature Reviews Neurology August 2009Document13 pagesLumbar Spinal Stenosis: Syndrome, Diagnostics and Treatment: Nature Reviews Neurology August 2009Surya PangeranNo ratings yet
- Early Repolarization Pattern and Risk For Arrhythmia Death Meta AnalysisDocument6 pagesEarly Repolarization Pattern and Risk For Arrhythmia Death Meta Analysisfindingnemo667No ratings yet
- Continuous Determination of Optimal Cerebral Perfusion Pressure in Traumatic Brain InjuryDocument8 pagesContinuous Determination of Optimal Cerebral Perfusion Pressure in Traumatic Brain InjurydrdivyapukNo ratings yet
- Bateman2017Document6 pagesBateman2017Meris JugadorNo ratings yet
- Predictors of Outcome in AneurysmalDocument7 pagesPredictors of Outcome in AneurysmalNeni NirmalaNo ratings yet
- Seiffge 2018Document3 pagesSeiffge 2018barti koksNo ratings yet
- Cooper Et Al 2007 The Role of Endomyocardial Biopsy in The Management of Cardiovascular DiseaseDocument18 pagesCooper Et Al 2007 The Role of Endomyocardial Biopsy in The Management of Cardiovascular DiseaseEszter SzerencsiNo ratings yet
- Adult NCSE Power KN 2015Document5 pagesAdult NCSE Power KN 2015Hendra PermanaNo ratings yet
- Kwon Et Al 2020 Deep Learning Based Algorithm For Detecting Aortic Stenosis Using ElectrocardiographyDocument16 pagesKwon Et Al 2020 Deep Learning Based Algorithm For Detecting Aortic Stenosis Using Electrocardiography施展No ratings yet
- ToastDocument7 pagesToastallisonjramirezNo ratings yet
- Ankylosing SpondylitesDocument16 pagesAnkylosing SpondylitesJyotirmayeeNo ratings yet
- Clinical Neurology and NeurosurgeryDocument14 pagesClinical Neurology and NeurosurgeryabbbabbbNo ratings yet
- Jaha 119 013678Document18 pagesJaha 119 013678Bosman AriestaNo ratings yet
- Time Trends in Atrial Fibrillation-Associated Stroke and Premorbid AnticoagulationDocument7 pagesTime Trends in Atrial Fibrillation-Associated Stroke and Premorbid Anticoagulationmuhamad ibnu sinaNo ratings yet
- J LPM 2019 03 016 PDFDocument9 pagesJ LPM 2019 03 016 PDFDessytha NathaniaNo ratings yet
- A Modified Anatomical-Functional-Rope (Af-Rope) Score Improves Patient Selection For Patent Foramen Ovale ClosureDocument4 pagesA Modified Anatomical-Functional-Rope (Af-Rope) Score Improves Patient Selection For Patent Foramen Ovale ClosureDessytha NathaniaNo ratings yet
- Acute Rheumatic Fever Diagnosis and Management - Rhda Workshop March 2016 Brisbane - Final PDFDocument61 pagesAcute Rheumatic Fever Diagnosis and Management - Rhda Workshop March 2016 Brisbane - Final PDFDessytha NathaniaNo ratings yet
- JONESDocument61 pagesJONESDessytha NathaniaNo ratings yet
- Abdullah JavedDocument8 pagesAbdullah JavedTahir MahmoodNo ratings yet
- 1 Structural - FunctionalismDocument57 pages1 Structural - FunctionalismCinnamonNo ratings yet
- Hick's Law Lab 1Document6 pagesHick's Law Lab 1Merna SamieNo ratings yet
- 16.21.1814 EbookDocument442 pages16.21.1814 EbookSutadi Triputra100% (1)
- Im12a01f01 03enDocument95 pagesIm12a01f01 03enkjonasamNo ratings yet
- Webhunt Conor FoleyDocument3 pagesWebhunt Conor Foleyapi-367746310No ratings yet
- Challenges To IoT-Enabled Predictive Maintenance For Industry 4.0Document13 pagesChallenges To IoT-Enabled Predictive Maintenance For Industry 4.0BrunoNo ratings yet
- Selina Concise Physics Solutions Class 6 Chapter 1 MatterDocument22 pagesSelina Concise Physics Solutions Class 6 Chapter 1 MatterAltaf TalpurNo ratings yet
- RCA SystemLink3Document9 pagesRCA SystemLink3JerônimoNo ratings yet
- Lab. 12 NylonDocument4 pagesLab. 12 NyloncsnNo ratings yet
- Example The Inductance of A SolenoidDocument3 pagesExample The Inductance of A SolenoidMuhamad YusupNo ratings yet
- BlackBerry Wireless Headset HS 700 User Guide 1035096 0819052837 001 USDocument4 pagesBlackBerry Wireless Headset HS 700 User Guide 1035096 0819052837 001 USPopescu CristiNo ratings yet
- Experiment 1 FINALDocument12 pagesExperiment 1 FINALMaiSakurajimaNo ratings yet
- 02.1-WCDMA Basic Principle of Radio Propagation - 20051214Document20 pages02.1-WCDMA Basic Principle of Radio Propagation - 20051214kltowerNo ratings yet
- Happiness - Mark MansonDocument26 pagesHappiness - Mark MansonJake100% (3)
- Line Dance ModuleDocument34 pagesLine Dance ModuleMarie Antionette MondragonNo ratings yet
- Wqt-1-13-W-1-3g-Smaw-Alclad-Aws D1.1Document1 pageWqt-1-13-W-1-3g-Smaw-Alclad-Aws D1.1Rejoy babyNo ratings yet
- Infections PDFDocument29 pagesInfections PDFLoudry ElfaNo ratings yet
- NBRK0200 Installation Configuration ManualDocument32 pagesNBRK0200 Installation Configuration ManualGoran JovanovicNo ratings yet
- Anima Core BookDocument317 pagesAnima Core BookPeter HillaryNo ratings yet
- M45913-1 RevADocument4 pagesM45913-1 RevAMAI_QualityNo ratings yet
- Amniotic Fluid PDFDocument24 pagesAmniotic Fluid PDFJoshua Ty CayetanoNo ratings yet
- EW - European Whirl (Classic Trip)Document19 pagesEW - European Whirl (Classic Trip)Gabriele Di RivombrosaNo ratings yet
- Hotel Minimum ReqDocument28 pagesHotel Minimum ReqAnusha AshokNo ratings yet
- Text 1 (A & B)Document2 pagesText 1 (A & B)ifx leeNo ratings yet
- Poster PresentationDocument1 pagePoster PresentationPilla SatishNo ratings yet
- Measuring Your Carbon Footprint PowerPointDocument16 pagesMeasuring Your Carbon Footprint PowerPointpremquilonNo ratings yet
- Roblox Admins Free WorkingDocument483 pagesRoblox Admins Free WorkingCrazy SodaNo ratings yet