Download as pdf or txt
You might also like
- NCP Anxiety Related To Unconscious Conflict About Essential Goals and Values of Life Into Financial Instability Causing DistressDocument2 pagesNCP Anxiety Related To Unconscious Conflict About Essential Goals and Values of Life Into Financial Instability Causing DistressMa. Elaine Carla Tating33% (3)
- Nursing Care Plan Dysfunctional Uterine Bleeding (DUB)Document2 pagesNursing Care Plan Dysfunctional Uterine Bleeding (DUB)deric90% (10)
- NURSING CARE PLAN - Breast CancerDocument2 pagesNURSING CARE PLAN - Breast Cancerderic100% (3)
- NCP Self EsteemDocument4 pagesNCP Self Esteemeinghel_24100% (2)
- Nursing Care Plan PDFDocument6 pagesNursing Care Plan PDFEngely MercaderNo ratings yet
- 26 - LCCI L3 AC - Sep 2019 - ASE 20104 - MSDocument15 pages26 - LCCI L3 AC - Sep 2019 - ASE 20104 - MSKhin Zaw Htwe100% (6)
- CVL Consent PDFDocument5 pagesCVL Consent PDFGolam SarwarNo ratings yet
- SUMMATIVE TEST IN SCIENCE 6 (Fourth Quarter)Document3 pagesSUMMATIVE TEST IN SCIENCE 6 (Fourth Quarter)Cindy Mae Macamay100% (2)
- Nursing Care Plan: Objective: Admission DiagnosisDocument4 pagesNursing Care Plan: Objective: Admission DiagnosisJe ZalNo ratings yet
- Cues/Data Nursing Diagnosis Interference Planning Intervention Rationale EvaluationDocument3 pagesCues/Data Nursing Diagnosis Interference Planning Intervention Rationale EvaluationLouwella RamosNo ratings yet
- Palo Ayen Trisha MCN Lab Module 5 NCPDocument5 pagesPalo Ayen Trisha MCN Lab Module 5 NCPAyen PaloNo ratings yet
- Guarin NCPDocument4 pagesGuarin NCPMary Joy Anne LucasNo ratings yet
- Roldan NCP-G2CDocument4 pagesRoldan NCP-G2CCeegi Arville RoldanNo ratings yet
- Nursing Care Plan Endometrial CancerDocument2 pagesNursing Care Plan Endometrial Cancerderic88% (16)
- Nursing Care Plan Nursing Diagnosis Anxiety (Mild)Document4 pagesNursing Care Plan Nursing Diagnosis Anxiety (Mild)yvenette_kris871881% (27)
- NCP CervicalDocument4 pagesNCP CervicalZaira Kim93% (14)
- Disaster PTSDocument3 pagesDisaster PTSkarl de guzmanNo ratings yet
- Game Name LIFE THE GAME Stay SafeDocument9 pagesGame Name LIFE THE GAME Stay SafeJASTINE JOY PEREZNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanMel Izhra N. MargateNo ratings yet
- Using The Scenario About Human Sexuality Formulate A Nursing Care PlanDocument4 pagesUsing The Scenario About Human Sexuality Formulate A Nursing Care PlanSteven ConejosNo ratings yet
- Nursing Department: Embracing World Class Standards Care To Learn, Learn To CareDocument11 pagesNursing Department: Embracing World Class Standards Care To Learn, Learn To CareJoselyn M. LachicaNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanBlitz KriegNo ratings yet
- Recognize The Need For Eating and Drinking ProperlyDocument3 pagesRecognize The Need For Eating and Drinking ProperlyJacquelyn NombradoNo ratings yet
- NCP Active SeizureDocument4 pagesNCP Active SeizureAngelica CorpuzNo ratings yet
- Dementia NCPDocument3 pagesDementia NCPDonnalyn MillaresNo ratings yet
- UntitledDocument2 pagesUntitledKristil ChavezNo ratings yet
- FNCPDocument1 pageFNCPThunderNo ratings yet
- Sas 22-23Document15 pagesSas 22-23Jilkiah Mae Alfoja CampomanesNo ratings yet
- Nursing Care Plan Impaired CommunicationDocument3 pagesNursing Care Plan Impaired CommunicationRamiel ChristopherNo ratings yet
- Risk For Falls Related To Memory Deficits, Confusion, and Physical InstabilityDocument2 pagesRisk For Falls Related To Memory Deficits, Confusion, and Physical InstabilityJerreca DasasNo ratings yet
- Schizo NCPDocument18 pagesSchizo NCPRoscheen Berg TutorNo ratings yet
- LCUP Family Nursing Care Plan AsthmaDocument3 pagesLCUP Family Nursing Care Plan AsthmaKia MadineNo ratings yet
- NCPDocument1 pageNCPSherry Ann FayeNo ratings yet
- Babon, Christelle Anne - FNCPDocument2 pagesBabon, Christelle Anne - FNCPchristelleannebabon196No ratings yet
- NCP EamcDocument4 pagesNCP EamcsustiguerchristianpaulNo ratings yet
- IndependentDocument4 pagesIndependentTel EscorialNo ratings yet
- NCP - AnxietyDocument4 pagesNCP - AnxietyRoyce Vincent Tizon100% (1)
- Exam 3 JeopardyDocument4 pagesExam 3 JeopardyDiya AggarwalNo ratings yet
- Fear Related To Threat of DystociaDocument2 pagesFear Related To Threat of DystociaMark FernandezNo ratings yet
- Nursing Care Plan For Breast Cancer NCPDocument2 pagesNursing Care Plan For Breast Cancer NCPEsha MeharNo ratings yet
- ImprovingUnderstanding PatientExperience NM Set23 PEDRODocument23 pagesImprovingUnderstanding PatientExperience NM Set23 PEDROana.griloNo ratings yet
- Nursing Care Plan For Breast Cancer NCP PDFDocument2 pagesNursing Care Plan For Breast Cancer NCP PDFMaina BarmanNo ratings yet
- Nursing Care Plan For Breast Cancer NCP PDFDocument2 pagesNursing Care Plan For Breast Cancer NCP PDFMaina Barman100% (1)
- Nursing Care Plan For Breast Cancer NCPDocument2 pagesNursing Care Plan For Breast Cancer NCPMaina BarmanNo ratings yet
- Dissociative Spectrum Disorders in The Primary Care Setting: One Personal Copy May Be PrintedDocument5 pagesDissociative Spectrum Disorders in The Primary Care Setting: One Personal Copy May Be PrintedprematellieNo ratings yet
- Dienizs Labini BSN-3E Brain Cancer Activities: B. Glioblastoma MultiformeDocument11 pagesDienizs Labini BSN-3E Brain Cancer Activities: B. Glioblastoma MultiformeDienizs Labini TadenaNo ratings yet
- NCPDocument3 pagesNCPCharles Mallari Valdez100% (1)
- NCP - Patient For Electrocardiogram (ECG)Document1 pageNCP - Patient For Electrocardiogram (ECG)SelwynVillamorPatenteNo ratings yet
- NCP ManaoagDocument3 pagesNCP ManaoagAkira Poscablo PiranteNo ratings yet
- FNCPDocument2 pagesFNCPJaylove CastilloNo ratings yet
- NCP AshraDocument4 pagesNCP AshraSherry RodriguezNo ratings yet
- Activity 2 Nursing Care Plan Making: College of Health Sciences Department of NursingDocument3 pagesActivity 2 Nursing Care Plan Making: College of Health Sciences Department of NursingReeka Izabel Dela PeñaNo ratings yet
- NCP Blurred VisionDocument3 pagesNCP Blurred Visionناديه المعمريNo ratings yet
- NCP JoverDocument3 pagesNCP JoverJOVEMEA LIRAYNo ratings yet
- Workbook & Summary - The Gift Of Fear - Based On The Book By Gavin De BeckerFrom EverandWorkbook & Summary - The Gift Of Fear - Based On The Book By Gavin De BeckerNo ratings yet
- Be Safe - Growing Safety Awareness for Accident Prevention in Dangerous Occupations: Safety Through Mindfulness, #1From EverandBe Safe - Growing Safety Awareness for Accident Prevention in Dangerous Occupations: Safety Through Mindfulness, #1No ratings yet
- Ancestral Shadows: Unraveling the Hidden Impact of Inherited Family Trauma and the Path to Recovery: Generational Healing, #1From EverandAncestral Shadows: Unraveling the Hidden Impact of Inherited Family Trauma and the Path to Recovery: Generational Healing, #1No ratings yet
- Recovery From Childhood Trauma: Become a happier and healthier version of yourself as you begin to understand the key concepts of childhood trauma, its causes, its effects and its healing process.From EverandRecovery From Childhood Trauma: Become a happier and healthier version of yourself as you begin to understand the key concepts of childhood trauma, its causes, its effects and its healing process.No ratings yet
- Daring To Be Great ForeverDocument2 pagesDaring To Be Great ForeverRhoda Mae CocjinNo ratings yet
- Course Info Sheet - NST001Document7 pagesCourse Info Sheet - NST001Ching DialomaNo ratings yet
- Prezentare AGS en +romDocument34 pagesPrezentare AGS en +romGina Daniela BorcanNo ratings yet
- HR Practices NTPCDocument16 pagesHR Practices NTPCRuchika SinhaNo ratings yet
- ExamenesDocument4 pagesExamenesZareli Lazo AriasNo ratings yet
- Swot Analysis 123Document15 pagesSwot Analysis 123Roif SamsulNo ratings yet
- HUC Program Grading SchemeDocument1 pageHUC Program Grading SchemeThanis RaoNo ratings yet
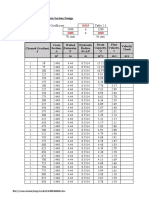
- Box Culvert / U-Drain Section Design: File:///conversion/tmp/scratch/488560866Document9 pagesBox Culvert / U-Drain Section Design: File:///conversion/tmp/scratch/488560866azwanNo ratings yet
- SUBWAY EditedDocument13 pagesSUBWAY Editedsonaxiv697No ratings yet
- ELLNA iMPLEMENTER FINALDocument22 pagesELLNA iMPLEMENTER FINALGina HerraduraNo ratings yet
- Inbound 5129053772572461691Document17 pagesInbound 5129053772572461691LaksndNo ratings yet
- 8 Fall of The Ottoman EmpireDocument10 pages8 Fall of The Ottoman Empireapi-303147801No ratings yet
- Classroom Accommodations For Students With Learning Difficulties and DisabilitiesDocument2 pagesClassroom Accommodations For Students With Learning Difficulties and Disabilitiesapi-359063455No ratings yet
- Data Structures Algorithms in Python 1St Edition John Canning Full ChapterDocument67 pagesData Structures Algorithms in Python 1St Edition John Canning Full Chapterchester.gallegos491100% (6)
- Siemens - General Fire Detection System PlanningDocument98 pagesSiemens - General Fire Detection System PlanningSimon BolivarNo ratings yet
- Reading Section Worksheet XIDocument5 pagesReading Section Worksheet XIgaurav20199No ratings yet
- Air Conditioning System: Click The Volvo-Logo in The Lower Right Corner To Return To This Menu Main MenuDocument22 pagesAir Conditioning System: Click The Volvo-Logo in The Lower Right Corner To Return To This Menu Main MenuLeopoldo Del Campo100% (1)
- 7480H - Catalog - Mobile - Fuel - Filtration - Filtors Racor PDFDocument98 pages7480H - Catalog - Mobile - Fuel - Filtration - Filtors Racor PDFFrank Felipe Cruz ChavezNo ratings yet
- Identifying Errors 2Document4 pagesIdentifying Errors 2Renz Daniel Fetalvero DemaisipNo ratings yet
- Breast CA SeminarDocument60 pagesBreast CA SeminarAliyi MuktarNo ratings yet
- CT Secondary InjectionDocument2 pagesCT Secondary InjectionHumayun AhsanNo ratings yet
- 2178 Reference AciDocument3 pages2178 Reference AciAnn GordonNo ratings yet
- Chapter 4 Manual Assembly LinesDocument49 pagesChapter 4 Manual Assembly LinesRohit WadhwaniNo ratings yet
- 4.3 Introduction To Database ManagementDocument14 pages4.3 Introduction To Database ManagementppghoshinNo ratings yet
- Load Cell Input ModuleDocument3 pagesLoad Cell Input Moduleabo omrNo ratings yet
- To Biochemistry: Murang'a University of TechnologyDocument6 pagesTo Biochemistry: Murang'a University of TechnologyJoseph NyabugaNo ratings yet
- Marketing Advanced HW 3 A5-7, A9-12Document3 pagesMarketing Advanced HW 3 A5-7, A9-12ruf62ny5No ratings yet