Download as pdf or txt
You might also like
- Wpa PaperDocument12 pagesWpa Paperkhairul ezwan100% (1)
- Advance Baking CompilationDocument44 pagesAdvance Baking CompilationCherry Brutas100% (1)
- For Hino: Tics Pump Electrical Part Resistance Value ListDocument35 pagesFor Hino: Tics Pump Electrical Part Resistance Value Listfersky90% (10)
- 141 Jazz Guitar LicksDocument114 pages141 Jazz Guitar LicksINTJason100% (5)
- Automated Nucleated Red Blood Cell Count Using The Mindray BC - 6800 Hematology AnalyzerDocument6 pagesAutomated Nucleated Red Blood Cell Count Using The Mindray BC - 6800 Hematology AnalyzerAngelNo ratings yet
- Evaluation of The Abbott CELL-DYN 4000 HematologyDocument10 pagesEvaluation of The Abbott CELL-DYN 4000 Hematologypasamuco473No ratings yet
- Evaluation of The Performance of Sysmex XN-3100 Automated Hematology Analyzer Regarding The Sysmex XE-2100 and Microscopic ExaminationDocument9 pagesEvaluation of The Performance of Sysmex XN-3100 Automated Hematology Analyzer Regarding The Sysmex XE-2100 and Microscopic ExaminationbalkisNo ratings yet
- User Verification of Abbott Alinity HQ HematologyDocument11 pagesUser Verification of Abbott Alinity HQ HematologyYetzh HayatiNo ratings yet
- Clinical Biochemistry: E. Schapkaitz, S. RaburabuDocument7 pagesClinical Biochemistry: E. Schapkaitz, S. RaburabuMunawwar SaukaniNo ratings yet
- Alta Mimi 2012Document8 pagesAlta Mimi 2012Erika SantiagoNo ratings yet
- Pandey 2020Document5 pagesPandey 2020my accountNo ratings yet
- Int J Lab Hematology - 2022 - Marinov - Validation of A Single Tube 3 Colour Immature Red Blood Cell Screening Assay ForDocument7 pagesInt J Lab Hematology - 2022 - Marinov - Validation of A Single Tube 3 Colour Immature Red Blood Cell Screening Assay ForMaria SousaNo ratings yet
- Evaluation and Comparison of The New Mindray BC-6200 Hematology Analyzer With ADVIA 2120iDocument8 pagesEvaluation and Comparison of The New Mindray BC-6200 Hematology Analyzer With ADVIA 2120iGABRIELA HERRERANo ratings yet
- MicremiCRP Nomura Eval 2014IJLH12312Document9 pagesMicremiCRP Nomura Eval 2014IJLH12312Shan AhmadNo ratings yet
- Letter To The Editor: Comparison Between Automated and Microscopic Analysis in Body Fluids CytologyDocument3 pagesLetter To The Editor: Comparison Between Automated and Microscopic Analysis in Body Fluids CytologybalkisNo ratings yet
- XN 3000 VS BeckmanDocument8 pagesXN 3000 VS BeckmanZied FehriNo ratings yet
- eJHaem - 2022 - Linko Parvinen - HemoScreen Hematology Analyzer Compared To Sysmex XN For Complete Blood Count White BloodDocument9 pageseJHaem - 2022 - Linko Parvinen - HemoScreen Hematology Analyzer Compared To Sysmex XN For Complete Blood Count White Bloodrince noveliaNo ratings yet
- An Artificial Intelligence-Assisted Diagnostic PlaDocument11 pagesAn Artificial Intelligence-Assisted Diagnostic Plahanrong912No ratings yet
- Lmy 030Document7 pagesLmy 030Tuan NguyenNo ratings yet
- Comparison of ABX PENTRA 120 Retic, Sysmex R-2000, Flow Cytometry, and Manual CountsDocument10 pagesComparison of ABX PENTRA 120 Retic, Sysmex R-2000, Flow Cytometry, and Manual CountsdayanaNo ratings yet
- Jurnal Alin Poct Dipstk UrineDocument9 pagesJurnal Alin Poct Dipstk Urineherlina armarianiNo ratings yet
- Performance Evaluation of Abbott CELL-DYN Ruby For Routine UseDocument8 pagesPerformance Evaluation of Abbott CELL-DYN Ruby For Routine UseSethLunaNo ratings yet
- Poredjenje Mindray BC-5180 Vs Sysmex XN-1000Document6 pagesPoredjenje Mindray BC-5180 Vs Sysmex XN-1000Miroslav TomovicNo ratings yet
- Sysmex XN WPC ChannelDocument3 pagesSysmex XN WPC ChannelZied FehriNo ratings yet
- Red Blood Cell Agglutination For Blood Typing Within Passive Microfluidic BiochipsDocument13 pagesRed Blood Cell Agglutination For Blood Typing Within Passive Microfluidic BiochipsCatia CorreaNo ratings yet
- Body Fluid Cell Counts by Automated MethodsDocument11 pagesBody Fluid Cell Counts by Automated MethodsntnquynhproNo ratings yet
- Advanced MAPSS™ Technology of Alinity HQDocument7 pagesAdvanced MAPSS™ Technology of Alinity HQYetzh HayatiNo ratings yet
- TCVDocument8 pagesTCVChatchai KreepalaNo ratings yet
- Performance of CellaVision DM96 in Leukocyte ClassificationDocument5 pagesPerformance of CellaVision DM96 in Leukocyte ClassificationarielNo ratings yet
- Bruegel 2015Document15 pagesBruegel 2015my accountNo ratings yet
- Tampil Jurnal Dr. Hafni FixDocument28 pagesTampil Jurnal Dr. Hafni FixCenyiqanita NurqanitaNo ratings yet
- 2017 Clin Lab Sci Doing and Zhang A Methodical Approach To Interpreting The RBC Parameters of The CBCDocument13 pages2017 Clin Lab Sci Doing and Zhang A Methodical Approach To Interpreting The RBC Parameters of The CBCJonathan MilhomensNo ratings yet
- Dacosta 2015Document36 pagesDacosta 2015JE SimianNo ratings yet
- (14374331 - Clinical Chemistry and Laboratory Medicine (CCLM) ) Analytical Evaluation of Four Faecal Immunochemistry Tests For HaemoglobinDocument6 pages(14374331 - Clinical Chemistry and Laboratory Medicine (CCLM) ) Analytical Evaluation of Four Faecal Immunochemistry Tests For HaemoglobinguschinNo ratings yet
- New QuantitiesDocument6 pagesNew Quantities20100117 Bùi Thùy VyNo ratings yet
- NRBCDocument5 pagesNRBCGaurav AggarwalNo ratings yet
- Ok 2Document7 pagesOk 2cydolusNo ratings yet
- Six of Eight Hemoglobin A1c Point-of-Care Instruments Do Not Meet The General Accepted Analytical Performance CriteriaDocument9 pagesSix of Eight Hemoglobin A1c Point-of-Care Instruments Do Not Meet The General Accepted Analytical Performance CriteriaSaloustros GiannisNo ratings yet
- 173 FullDocument13 pages173 FullYaser MNo ratings yet
- Jcla 22392Document8 pagesJcla 22392Ajish joNo ratings yet
- Verification and Quality Control of Routine Hematology AnalyzersDocument10 pagesVerification and Quality Control of Routine Hematology AnalyzersRafat ElshemiNo ratings yet
- Ijlh 12503Document11 pagesIjlh 12503MUCHLISOH ZULAEHANo ratings yet
- Int J Lab Hematology - 2016 - Vis - Verification and Quality Control of Routine Hematology AnalyzersDocument10 pagesInt J Lab Hematology - 2016 - Vis - Verification and Quality Control of Routine Hematology AnalyzersHerbanu PramonoNo ratings yet
- European Journal of Biomedical AND Pharmaceutical SciencesDocument5 pagesEuropean Journal of Biomedical AND Pharmaceutical SciencesGaurav AggarwalNo ratings yet
- Ijpo 3 (2) 351-353Document3 pagesIjpo 3 (2) 351-353anggaririnNo ratings yet
- HematologiaDocument8 pagesHematologiaRafael RibeiroNo ratings yet
- The Clinical Relevance of Nucleated Red Blood Cell CountsDocument5 pagesThe Clinical Relevance of Nucleated Red Blood Cell CountspaconscribdNo ratings yet
- Lectura Complementaria. Método de Referencia para El Recuento de PlaquetasDocument5 pagesLectura Complementaria. Método de Referencia para El Recuento de PlaquetasFlor GianoNo ratings yet
- Ajcpath128 0585Document5 pagesAjcpath128 0585adhialepNo ratings yet
- Novel Automated Hematology Parameters in Clinical Pediatric PracticeDocument9 pagesNovel Automated Hematology Parameters in Clinical Pediatric PracticerahulNo ratings yet
- 11 Feb Denise PHD Final With Corrections For PrintingDocument272 pages11 Feb Denise PHD Final With Corrections For PrintingAbeer AbdullahNo ratings yet
- Int J Lab Hematology - 2016 - Vis - Verification and Quality Control of Routine Hematology AnalyzersDocument10 pagesInt J Lab Hematology - 2016 - Vis - Verification and Quality Control of Routine Hematology AnalyzersletphuongNo ratings yet
- Guidance For Storing Blood Samples in Laboratories Performingcomplete Blood Count With DifferentialDocument6 pagesGuidance For Storing Blood Samples in Laboratories Performingcomplete Blood Count With Differentialimran ahmed siddiquiNo ratings yet
- Sensitive Albuminuria Analysis Using Dye-Binding Based Test StripsDocument24 pagesSensitive Albuminuria Analysis Using Dye-Binding Based Test StripsВалерия БедоеваNo ratings yet
- JurnalDocument6 pagesJurnalAnonymous bYYJdvXhlNNo ratings yet
- Evaluation of The Effect of Temperature and Time of Incubation On Complete Blood Count (CBC) TestsDocument4 pagesEvaluation of The Effect of Temperature and Time of Incubation On Complete Blood Count (CBC) TestsYaser MNo ratings yet
- Tracking Arteriovenous Fistula Maturation: A Novel Approach: Research Article - Advances in CKD 2019Document6 pagesTracking Arteriovenous Fistula Maturation: A Novel Approach: Research Article - Advances in CKD 2019Anonymous ATdLPZNo ratings yet
- Laboratory Hematology CriteriaDocument7 pagesLaboratory Hematology CriteriaRosNo ratings yet
- Hedley 2010Document12 pagesHedley 2010my accountNo ratings yet
- TRF 14043Document10 pagesTRF 14043Ahmad ANo ratings yet
- بيروان دكتورDocument9 pagesبيروان دكتورمني احمد قدحNo ratings yet
- QFPCRDocument21 pagesQFPCRPhạm Quốc ToảnNo ratings yet
- Laboratory Hematology PracticeFrom EverandLaboratory Hematology PracticeKandice Kottke-MarchantRating: 5 out of 5 stars5/5 (1)
- Cytogenetic Laboratory Management: Chromosomal, FISH and Microarray-Based Best Practices and ProceduresFrom EverandCytogenetic Laboratory Management: Chromosomal, FISH and Microarray-Based Best Practices and ProceduresNo ratings yet
- UtamaDocument14 pagesUtamaCenyiqanita NurqanitaNo ratings yet
- SodapdfDocument33 pagesSodapdfCenyiqanita NurqanitaNo ratings yet
- R-R-Ofd07193: Nfier) .988Document2 pagesR-R-Ofd07193: Nfier) .988Cenyiqanita NurqanitaNo ratings yet
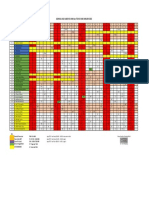
- Jadwal Insentif Bulanan 21 Juli - 20 AGUSTUS 2022Document2 pagesJadwal Insentif Bulanan 21 Juli - 20 AGUSTUS 2022Cenyiqanita NurqanitaNo ratings yet
- Tampil Jurnal Dr. Hafni FixDocument28 pagesTampil Jurnal Dr. Hafni FixCenyiqanita NurqanitaNo ratings yet
- ParameterDocument1 pageParameterCenyiqanita NurqanitaNo ratings yet
- Jadwal Fix Share Januari 2022Document1 pageJadwal Fix Share Januari 2022Cenyiqanita NurqanitaNo ratings yet
- Hepatic Insulin Clearance Is Increased in Patients With High Hba1C Type 2 Diabetes: A Preliminary ReportDocument8 pagesHepatic Insulin Clearance Is Increased in Patients With High Hba1C Type 2 Diabetes: A Preliminary ReportCenyiqanita NurqanitaNo ratings yet
- Matrix-Assisted Laser DesorptionIonization Time-OfDocument8 pagesMatrix-Assisted Laser DesorptionIonization Time-OfCenyiqanita NurqanitaNo ratings yet
- Quality Indicators in A Hematology Laboratory-A Retrospective AnalysisDocument6 pagesQuality Indicators in A Hematology Laboratory-A Retrospective AnalysisCenyiqanita NurqanitaNo ratings yet
- CDC Diagnostic TestingDocument19 pagesCDC Diagnostic TestingCenyiqanita NurqanitaNo ratings yet
- Three Years' Experience of Quality Monitoring Program On Pre-Analytical Errors in ChinaDocument7 pagesThree Years' Experience of Quality Monitoring Program On Pre-Analytical Errors in ChinaCenyiqanita NurqanitaNo ratings yet
- Urine AnalysisDocument69 pagesUrine Analysisvinay0717100% (3)
- Kuliah 1Document114 pagesKuliah 1Cenyiqanita NurqanitaNo ratings yet
- FBL1000 Pro Data SheetDocument2 pagesFBL1000 Pro Data SheetNovi unionNo ratings yet
- hw4 SolDocument3 pageshw4 SoladvifulNo ratings yet
- Spe 199993 MSDocument28 pagesSpe 199993 MSHussam AgabNo ratings yet
- Hambardzumyan InfDocument102 pagesHambardzumyan InfAnush AsrianNo ratings yet
- Dangase Group - Research FinalDocument59 pagesDangase Group - Research FinalGlenda PapelleroNo ratings yet
- Telephone EnglishDocument5 pagesTelephone EnglishZaw WinOoNo ratings yet
- Block 3 Welcome LetterDocument2 pagesBlock 3 Welcome LetterRobNo ratings yet
- MA 231 MATHEMATICS III 2006 Question PaperDocument3 pagesMA 231 MATHEMATICS III 2006 Question Paperyasin muhamedNo ratings yet
- Lesson Plan Ds 8603Document7 pagesLesson Plan Ds 8603sramalingam288953No ratings yet
- SPWLA Log IntegrationDocument14 pagesSPWLA Log IntegrationpahlawankemalemanNo ratings yet
- Petrochemical Standards (PDFDrive)Document68 pagesPetrochemical Standards (PDFDrive)fatimahNo ratings yet
- Philippines RegionsDocument5 pagesPhilippines RegionsKristine MercadoNo ratings yet
- Introductory Entomology: Third Semester Lamjung CampusDocument206 pagesIntroductory Entomology: Third Semester Lamjung Campusnishan khatriNo ratings yet
- Purpose - Device - Ravana - OSHODocument2 pagesPurpose - Device - Ravana - OSHOChitter SinghNo ratings yet
- IMMI Grant NotificationDocument4 pagesIMMI Grant NotificationAngeline GarciaNo ratings yet
- Bend TestDocument38 pagesBend TestAzan Safril100% (1)
- Articulo-Watson Crick PDFDocument2 pagesArticulo-Watson Crick PDFAjedrez ItineranteNo ratings yet
- Filtration For HPLC Sample Preparation DistributorDocument24 pagesFiltration For HPLC Sample Preparation DistributorTuyết NgânNo ratings yet
- Geofirma Geotextile Datasheet 2020Document1 pageGeofirma Geotextile Datasheet 2020Chandima AtapattuNo ratings yet
- TOT Water For Pharmaceutical Use - Part 1Document132 pagesTOT Water For Pharmaceutical Use - Part 1Delly AnakAfternoonyesterdays0% (1)
- Plagiarism Prevention Software: TurnitinDocument24 pagesPlagiarism Prevention Software: TurnitinJoshua QuayeNo ratings yet
- Reviewer in Pa 108Document14 pagesReviewer in Pa 108Madelyn OrfinadaNo ratings yet
- 2021 Nqesh Mock Test Set BDocument36 pages2021 Nqesh Mock Test Set Brandolf traigo100% (3)
- Chapter 4 - Braking System 4.1 Brake LinesDocument14 pagesChapter 4 - Braking System 4.1 Brake LinesEmanuel VidalNo ratings yet
- EN Quick Reference Guide Fabian HFOi-V4.0Document30 pagesEN Quick Reference Guide Fabian HFOi-V4.0Tanzimul IslamNo ratings yet
- Problem SetDocument12 pagesProblem SetJohn Lade Tan NacionalNo ratings yet