Download as pdf or txt
You might also like
- Working Together in Clinical SupervisionDocument28 pagesWorking Together in Clinical SupervisionCharleneKronstedt100% (1)
- Glutathione Parkinsons DiseaseDocument4 pagesGlutathione Parkinsons Diseaseimm100% (3)
- A Randomized Placebo-Controlled Pilot Study of N-Acetylcysteine in Youth With Autism Spectrum DisorderDocument9 pagesA Randomized Placebo-Controlled Pilot Study of N-Acetylcysteine in Youth With Autism Spectrum DisorderdudihadinegoroNo ratings yet
- Caffeine As A Pharmacological ToolDocument5 pagesCaffeine As A Pharmacological ToolNala Dwi HartatiNo ratings yet
- Neuroprotective Effects Of The Pparβ/Δ Antagonist Gsk0660 In In Vitro And In Vivo Parkinson'S Disease ModelsDocument22 pagesNeuroprotective Effects Of The Pparβ/Δ Antagonist Gsk0660 In In Vitro And In Vivo Parkinson'S Disease ModelsAmyNo ratings yet
- Oral Ambroxol Increases Brain Glucocerebrosidase Activity in A Nonhuman PrimateDocument3 pagesOral Ambroxol Increases Brain Glucocerebrosidase Activity in A Nonhuman PrimateTia MutiaraNo ratings yet
- Glucocorticoid Current N FutureDocument15 pagesGlucocorticoid Current N FutureAriani SetyaningsihNo ratings yet
- Cells 09 00376 PDFDocument19 pagesCells 09 00376 PDFMikel MillerNo ratings yet
- Latar Belakang Kayu ManisDocument11 pagesLatar Belakang Kayu ManisMuhammad YarhamNo ratings yet
- 66 68 PBDocument89 pages66 68 PBAyesha FatimaNo ratings yet
- The Effect of An Inhaled Corticosteroid On Glucose Control in Type 2 DiabetesDocument7 pagesThe Effect of An Inhaled Corticosteroid On Glucose Control in Type 2 DiabetesAshraf Uddin AhmedNo ratings yet
- Trial KetogenicDietAndFastingDietAsNDocument9 pagesTrial KetogenicDietAndFastingDietAsNFrancois MerNo ratings yet
- Manejo de La Sepsis 2Document5 pagesManejo de La Sepsis 2Rachmi Pratiwi Febrita PartiNo ratings yet
- Chemotherapy For Tuberculous Meningitis: Peter R. Donald, M.DDocument3 pagesChemotherapy For Tuberculous Meningitis: Peter R. Donald, M.DDirga Rasyidin LNo ratings yet
- Probiotics For Parkinson's Disease: Molecular SciencesDocument26 pagesProbiotics For Parkinson's Disease: Molecular SciencesFanny CruzNo ratings yet
- NEJMoa 1114287Document10 pagesNEJMoa 1114287yulibudhyNo ratings yet
- Cytoplasmic p21 Induced by p65 Prevents Doxorubicin-Induced Cell Death in Pancreatic Carcinoma Cell LineDocument10 pagesCytoplasmic p21 Induced by p65 Prevents Doxorubicin-Induced Cell Death in Pancreatic Carcinoma Cell LineTarmidi MidziNo ratings yet
- Apremilast Improves Psoriasis With A Side Order of Weight LossDocument9 pagesApremilast Improves Psoriasis With A Side Order of Weight LossgopalNo ratings yet
- Intranasal Glutathione Cognitive Vitality For ResearchersDocument9 pagesIntranasal Glutathione Cognitive Vitality For ResearchersMarrauNo ratings yet
- The Anticonvulsant Effects of Ketogenic Diet On EpDocument5 pagesThe Anticonvulsant Effects of Ketogenic Diet On EpDianaNo ratings yet
- Perspective Is Therapeutic Plasma Exchange A Viable Option For TreatingDocument11 pagesPerspective Is Therapeutic Plasma Exchange A Viable Option For TreatingRaul Rios RitterNo ratings yet
- An Open Label Study Evaluating The Safety and Efficacy of Budesonide in Patients With Iga Nephropathy at High Risk of ProgressionDocument11 pagesAn Open Label Study Evaluating The Safety and Efficacy of Budesonide in Patients With Iga Nephropathy at High Risk of ProgressionMukesh DassaniNo ratings yet
- Review Article: Pharmacogenomics of Drug Response in Type 2 Diabetes: Toward The Definition of Tailored Therapies?Document11 pagesReview Article: Pharmacogenomics of Drug Response in Type 2 Diabetes: Toward The Definition of Tailored Therapies?James CowellNo ratings yet
- Cadeddu Et Al J Med Case Reports 2015Document6 pagesCadeddu Et Al J Med Case Reports 2015Sheila UlinaNo ratings yet
- Pharmacokinetic-Pharmacodynamic Crisis in The Elderly: Ehab S. Eldesoky, MD, PHDDocument11 pagesPharmacokinetic-Pharmacodynamic Crisis in The Elderly: Ehab S. Eldesoky, MD, PHDMonica LucaciuNo ratings yet
- FRGS2023 LatestDocument12 pagesFRGS2023 Latests221598No ratings yet
- Articulo 20 DietaDocument19 pagesArticulo 20 DietaCecilia DavilaNo ratings yet
- Adipose Tissue As A Target For Second-Generation (Atypical) AntipsychoticsDocument14 pagesAdipose Tissue As A Target For Second-Generation (Atypical) AntipsychoticsAgustin NunezNo ratings yet
- Keto Diet & AlzheimerDocument10 pagesKeto Diet & AlzheimerAksil IfrenNo ratings yet
- Ijms 19 00122Document10 pagesIjms 19 00122roxanaNo ratings yet
- E003290 FullDocument9 pagesE003290 FullANGELA CAMILA JARA LUZURIAGANo ratings yet
- Edr 05 155Document8 pagesEdr 05 155Noor NoorNo ratings yet
- Obesity, Antioxidants and Negative SymptomDocument6 pagesObesity, Antioxidants and Negative SymptomsiralkNo ratings yet
- RepeatDocument3 pagesRepeatntnquynhproNo ratings yet
- Sunday O. Oyedemi - Godswill Nwaogu - Chika I. Chukwuma - Olaoluwa T. Adeyemi - Motlalepula G. Matsabisa - Shasank S. Swain - Olayinka A. AiyegoroDocument16 pagesSunday O. Oyedemi - Godswill Nwaogu - Chika I. Chukwuma - Olaoluwa T. Adeyemi - Motlalepula G. Matsabisa - Shasank S. Swain - Olayinka A. AiyegoroGiovanni OliveiraNo ratings yet
- Green Tea and Quercetin Sensitize PC-3 Xenograft Prostate Tumors To Docetaxel ChemotherapyDocument11 pagesGreen Tea and Quercetin Sensitize PC-3 Xenograft Prostate Tumors To Docetaxel ChemotherapykgoffscsuNo ratings yet
- Molecules: Neuroprotective E Neurological DiseasesDocument16 pagesMolecules: Neuroprotective E Neurological DiseasesPsicoterapia InfantilNo ratings yet
- Pro-Apoptotic Effect of Rice Bran Inositol Hexaphosphate (IP) On HT-29 Colorectal Cancer CellsDocument14 pagesPro-Apoptotic Effect of Rice Bran Inositol Hexaphosphate (IP) On HT-29 Colorectal Cancer Cellsastuti susantiNo ratings yet
- Parkinson's Disease Mitochondrial Molecular Pathology Inflammation Statins and Therapeutic Neuroprotective Nutrition Nutr Clin Pract 2010Document20 pagesParkinson's Disease Mitochondrial Molecular Pathology Inflammation Statins and Therapeutic Neuroprotective Nutrition Nutr Clin Pract 2010Sandra Garnés RancurelloNo ratings yet
- Dietiker Mecobalamin PDFDocument6 pagesDietiker Mecobalamin PDFTaufikk Haldi (Taufik)No ratings yet
- A Randomized, Double-Blind, PlacebocontrolledDocument14 pagesA Randomized, Double-Blind, PlacebocontrolledPrabanandaAdistanaNo ratings yet
- Biomedicines 11 01133Document14 pagesBiomedicines 11 01133y1ann1sNo ratings yet
- Kolberg 2015Document11 pagesKolberg 2015kotzaNo ratings yet
- Glutathione Precursor N-Acetyl-cysteine Modulates EEG Synchronization in Schizophrenia PatientsDocument9 pagesGlutathione Precursor N-Acetyl-cysteine Modulates EEG Synchronization in Schizophrenia PatientsArturoNo ratings yet
- Anti-Inflammatory and Anti-Amyloidogenic Effects oDocument13 pagesAnti-Inflammatory and Anti-Amyloidogenic Effects oDhivya kothandanNo ratings yet
- Essential Update For SNDocument11 pagesEssential Update For SNshanksNo ratings yet
- A Deeper Dive Into Lipid Alterations in CKDDocument2 pagesA Deeper Dive Into Lipid Alterations in CKDAli TalalNo ratings yet
- Cytotoxics or Biologics in The Treatment of Sjogren's Syndrome Biological AgentsDocument10 pagesCytotoxics or Biologics in The Treatment of Sjogren's Syndrome Biological AgentsPablo Isaias Jaramillo FrancoNo ratings yet
- Editorial The Role of Oxidative Stress in The Development of Diabetes Mellitus and Its ComplicationsDocument4 pagesEditorial The Role of Oxidative Stress in The Development of Diabetes Mellitus and Its Complicationsipd limabersaudaraNo ratings yet
- 49-1456198085 2 PDFDocument7 pages49-1456198085 2 PDFSipkhotunWindayaniNo ratings yet
- Therapeutic Drug Monitoring of Carbamazepine A 20-YearDocument9 pagesTherapeutic Drug Monitoring of Carbamazepine A 20-YearEla chawNo ratings yet
- Approach To Patient With Glucocorticoid Induced Adrenal InsufficiencyDocument11 pagesApproach To Patient With Glucocorticoid Induced Adrenal InsufficiencyBHUENDOCRINE SRNo ratings yet
- 2 Glucosa y Neuronas - Journal of Neurochemistry - 2020 - Gherardelli - Andrographolide Restores Glucose Uptake in Rat Hippocampal NeuronsDocument12 pages2 Glucosa y Neuronas - Journal of Neurochemistry - 2020 - Gherardelli - Andrographolide Restores Glucose Uptake in Rat Hippocampal NeuronsFerNo ratings yet
- Ketogenic Diets and Alzheimers DiseaseDocument9 pagesKetogenic Diets and Alzheimers DiseaseCaro GonzalezAFNo ratings yet
- JMC2010,53,5502 Gossypol-APADocument9 pagesJMC2010,53,5502 Gossypol-APAVincent GeruszNo ratings yet
- Caripirazine Rats SchizophreniaDocument39 pagesCaripirazine Rats SchizophreniaEsraa SaeedNo ratings yet
- Ijms 23 02673Document12 pagesIjms 23 02673Yaumil ChoiriNo ratings yet
- The Ketogenic Diet As A Non Pharmacological Treatment For HIV Associated Neurocognitive Disorder A Descriptive AnalysisDocument5 pagesThe Ketogenic Diet As A Non Pharmacological Treatment For HIV Associated Neurocognitive Disorder A Descriptive AnalysisPaul HartingNo ratings yet
- Base Pra Revisao 2Document11 pagesBase Pra Revisao 2Helena CysneirosNo ratings yet
- The Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianFrom EverandThe Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianNo ratings yet
- Next Generation Kinase Inhibitors: Moving Beyond the ATP Binding/Catalytic SitesFrom EverandNext Generation Kinase Inhibitors: Moving Beyond the ATP Binding/Catalytic SitesNo ratings yet
- Mind Hacks @team LiB - by Tom Stafford, Matt Webb PDFDocument1,578 pagesMind Hacks @team LiB - by Tom Stafford, Matt Webb PDFXade EulorNo ratings yet
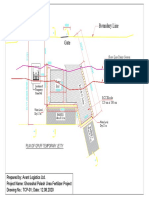
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- Basic Aviation Medicine: DR Firman Rachman Masjhur SPKP 17 November 2014Document43 pagesBasic Aviation Medicine: DR Firman Rachman Masjhur SPKP 17 November 2014sunarniNo ratings yet
- RusDocument42 pagesRusОльга КалмыковаNo ratings yet
- Chapter 6 MORTAR (Compatibility Mode) PDFDocument14 pagesChapter 6 MORTAR (Compatibility Mode) PDFBerhanu Mengstu AlemayohNo ratings yet
- Action Research On Students Misbehavior in ClassDocument4 pagesAction Research On Students Misbehavior in ClassAnalyn Girasol86% (7)
- Conceptual Design For Leachate Treatment Plant (LTP)Document19 pagesConceptual Design For Leachate Treatment Plant (LTP)Akyas M100% (1)
- Annex 1 - List of DelegatesDocument9 pagesAnnex 1 - List of DelegatesaseancocoaclubNo ratings yet
- Therapeutic Drug MonitoringDocument43 pagesTherapeutic Drug MonitoringMohammad AdibNo ratings yet
- Chapter 3 - Structure of The Nervous SystemDocument8 pagesChapter 3 - Structure of The Nervous Systemmanilyn dacoNo ratings yet
- The Nature of DreamsDocument2 pagesThe Nature of DreamsWesternLNo ratings yet
- 16HP Operators ManualDocument40 pages16HP Operators ManualPaul ArguinNo ratings yet
- Feel The Difference Owner'S Handbook: FordrangerDocument156 pagesFeel The Difference Owner'S Handbook: FordrangerGammy ZhammyNo ratings yet
- FYP-I Report-Hybrid Electric VehicleDocument35 pagesFYP-I Report-Hybrid Electric VehicleM UsamaNo ratings yet
- Farmakologi Dan Toksikologi 2022Document25 pagesFarmakologi Dan Toksikologi 2022Ghost TsushimaNo ratings yet
- 2020 JAADCR Araoye-Aguh CCCA Response To Topical MetforminDocument3 pages2020 JAADCR Araoye-Aguh CCCA Response To Topical MetforminKumar SukhdeoNo ratings yet
- Effect of Mulch On Soil TemperatureDocument11 pagesEffect of Mulch On Soil TemperatureEzeugo NelsonNo ratings yet
- Swale (Landform) - WikipediaDocument2 pagesSwale (Landform) - WikipediaMohamedNo ratings yet
- R410A Aqua Tempo Super Series Air Cooled Scroll Chiller Technical ManualDocument172 pagesR410A Aqua Tempo Super Series Air Cooled Scroll Chiller Technical ManualJuan Imas Del PuertoNo ratings yet
- Package Dimension (Qcc8C) : WWW - Datasheet.Co - KR WWW - Datasheet.Co - KRDocument3 pagesPackage Dimension (Qcc8C) : WWW - Datasheet.Co - KR WWW - Datasheet.Co - KRindustronicaNo ratings yet
- A9810029 enDocument3 pagesA9810029 enAnonymous nIcSGEwNo ratings yet
- Visual Encyclopedia of Chemical Engineering Rotational MoldingDocument6 pagesVisual Encyclopedia of Chemical Engineering Rotational MoldingVanNo ratings yet
- Zagreb-Miler Qualitative Tests Presentation PDFDocument36 pagesZagreb-Miler Qualitative Tests Presentation PDFFernando CruzNo ratings yet
- CH 6 Model 13 Financial Statements Scenario AnalysisDocument12 pagesCH 6 Model 13 Financial Statements Scenario AnalysisrealitNo ratings yet
- Issuance of Insanity 2Document278 pagesIssuance of Insanity 2Jonatha B SantosNo ratings yet
- Springfield Building Department Inspectional Services Notice of ViolationsDocument6 pagesSpringfield Building Department Inspectional Services Notice of ViolationsThe Republican/MassLive.comNo ratings yet
- Unit 2.2 Landforms and Landscape Processes Weathering and RiversDocument12 pagesUnit 2.2 Landforms and Landscape Processes Weathering and RiversifeNo ratings yet
- Work Life Balance QuestionnaireDocument4 pagesWork Life Balance QuestionnaireJonathan Britto75% (4)
- Escritura AutoguardadoDocument7 pagesEscritura AutoguardadoEren JaegerNo ratings yet