Download as pdf or txt
You might also like
- Pedsql Module CardioDocument31 pagesPedsql Module CardioRatna100% (1)
- Hyperthyroidism CaseDocument52 pagesHyperthyroidism CaseEncee Mian100% (2)
- NAVA HypoventilationDocument3 pagesNAVA HypoventilationFabian Esteban SubiabreNo ratings yet
- Sarnat 1976Document10 pagesSarnat 1976João Paulo RaposoNo ratings yet
- Neonatal Seizures: Incidence, Etiologies, Clinical Features and EEG Findings in The Neonatal Intensive Care UnitDocument5 pagesNeonatal Seizures: Incidence, Etiologies, Clinical Features and EEG Findings in The Neonatal Intensive Care UnitDoraemon BiruNo ratings yet
- Manejo Post Reanimacion AsfixiaDocument6 pagesManejo Post Reanimacion AsfixialauracamilacaceresdNo ratings yet
- ContentServer 2Document5 pagesContentServer 2Ni Wayan Ana PsNo ratings yet
- CorrespndenceDocument1 pageCorrespndenceTajul TajNo ratings yet
- Newborn With Meningoencephalitis Proteus MirabilisDocument5 pagesNewborn With Meningoencephalitis Proteus MirabilisRestu TriwulandaniNo ratings yet
- Convulsion NeonataleDocument15 pagesConvulsion NeonataleBookie BonishelliNo ratings yet
- Post Asphyxia Mangement NewDocument21 pagesPost Asphyxia Mangement NewAb Imo Pectore EvanNo ratings yet
- Avances en Convulsiones NeonatalesDocument10 pagesAvances en Convulsiones NeonatalesMarysol UlloaNo ratings yet
- NCC Case StudyDocument4 pagesNCC Case StudyMasego MekgoeNo ratings yet
- Early Life Serum Neurofilament Dynamics Predict Neurodevelopmental Outcome of Preterm InfantsDocument8 pagesEarly Life Serum Neurofilament Dynamics Predict Neurodevelopmental Outcome of Preterm InfantsKatharina GoeralNo ratings yet
- Prognostic Markers of Neonatal Outcomes in Full Term Neonates Suffering From Perinatal Asphyxia 2167 0897 1000193Document5 pagesPrognostic Markers of Neonatal Outcomes in Full Term Neonates Suffering From Perinatal Asphyxia 2167 0897 1000193Claudia BrînzaNo ratings yet
- Compromiso Cardìaco en Hiperglicinemia No CetosicaDocument4 pagesCompromiso Cardìaco en Hiperglicinemia No CetosicaDanny Bolaño MartinezNo ratings yet
- Late-Onset Rasmussen's Encephalitis and Long-Term Remission: Clinical CommentaryDocument4 pagesLate-Onset Rasmussen's Encephalitis and Long-Term Remission: Clinical CommentarySana ShafeeqNo ratings yet
- Vol-2 Issue-1 Approach To Respiratory Distress in The Newborn 19Document13 pagesVol-2 Issue-1 Approach To Respiratory Distress in The Newborn 19salamredNo ratings yet
- Medicine: Sudden Seizure During Cesarean SectionDocument2 pagesMedicine: Sudden Seizure During Cesarean SectionDavid RefuncionNo ratings yet
- Hipo Glice MiaDocument7 pagesHipo Glice MiaRosita Aguirre FloresNo ratings yet
- Congenital Nephrotic Syndrome: A Cases Report: Case Report Open AccessDocument4 pagesCongenital Nephrotic Syndrome: A Cases Report: Case Report Open AccessAzaliRiccoNo ratings yet
- Nefritis U Henoh Šenlajnovoj Purpuri Kod Dece: Iskustva U Prognozi I TerapijiDocument5 pagesNefritis U Henoh Šenlajnovoj Purpuri Kod Dece: Iskustva U Prognozi I TerapijiDewi PrasetiaNo ratings yet
- Hart. Neonatal Seizures p2Document8 pagesHart. Neonatal Seizures p2Ibai ArregiNo ratings yet
- ACNS Guideline Continuous Electroencephalography Monitoring in NeonatesDocument7 pagesACNS Guideline Continuous Electroencephalography Monitoring in NeonatesShanaHNo ratings yet
- NIH Public Access: Update On PPHN: Mechanisms and TreatmentDocument24 pagesNIH Public Access: Update On PPHN: Mechanisms and TreatmentathayafebNo ratings yet
- Diaphragmatic Paralysis Associated With Neonatal Brachial Plexus PalsyDocument3 pagesDiaphragmatic Paralysis Associated With Neonatal Brachial Plexus PalsyDennyNo ratings yet
- Perinatal/Neonatal Case PresentationDocument5 pagesPerinatal/Neonatal Case PresentationAnkit sharmaNo ratings yet
- Ogs 63 293Document12 pagesOgs 63 293DavidNo ratings yet
- Management and Investigation of Neonatal Encephalopathy: 2017 UpdateDocument13 pagesManagement and Investigation of Neonatal Encephalopathy: 2017 Updatenuge putriNo ratings yet
- E349 FullDocument6 pagesE349 FullrakeNo ratings yet
- Kim 2014Document5 pagesKim 2014Huệ MinhNo ratings yet
- A Severe Asphyxiated Newborn: A Case ReportDocument13 pagesA Severe Asphyxiated Newborn: A Case ReportEeeeeeeeeNo ratings yet
- E527 FullDocument5 pagesE527 FullrakeNo ratings yet
- Penatalaksanaan Anestesi Pada Shaken Baby Syndrome Anesthesia Management For Shaken Baby SyndromeDocument9 pagesPenatalaksanaan Anestesi Pada Shaken Baby Syndrome Anesthesia Management For Shaken Baby SyndromeDesta FransiscaNo ratings yet
- Pediatric Neuroanesthesia: Neuroimaging Clinics OfnorthamericaDocument9 pagesPediatric Neuroanesthesia: Neuroimaging Clinics OfnorthamericaMerlin MuktialiNo ratings yet
- A Case of Successful Management of Guillainbarre Syndrome in PregnancyDocument3 pagesA Case of Successful Management of Guillainbarre Syndrome in PregnancyTias DiahNo ratings yet
- Pakistan SedasiDocument3 pagesPakistan SedasiAnonymous 8Jlc7aTs90No ratings yet
- Seizures in Pregnancy: Epilepsy, Eclampsia, and Stroke: Laura A. Hart, MD, and Baha M. Sibai, MDDocument18 pagesSeizures in Pregnancy: Epilepsy, Eclampsia, and Stroke: Laura A. Hart, MD, and Baha M. Sibai, MDFannyZamoraGranielNo ratings yet
- A-Acta Paediatr 2010 Apr 99 (4) 497-501Document5 pagesA-Acta Paediatr 2010 Apr 99 (4) 497-501Antonio MartinezNo ratings yet
- Allergic Enterocolitis Presenting As Recurrent Necrotizing Enterocolitis in Preterm NeonatesDocument3 pagesAllergic Enterocolitis Presenting As Recurrent Necrotizing Enterocolitis in Preterm NeonatesJuwita PratiwiNo ratings yet
- 1 s2.0 S1389945717302496 Main PDFDocument3 pages1 s2.0 S1389945717302496 Main PDFvalentinaNo ratings yet
- Periodic Breathing and Apnea in Preterm InfantsDocument4 pagesPeriodic Breathing and Apnea in Preterm InfantsIvan VeriswanNo ratings yet
- Early-Onset Sepsis :clinical and Laboratory ChallengeDocument34 pagesEarly-Onset Sepsis :clinical and Laboratory ChallengelordofthewebNo ratings yet
- Seizure: Nick Kane, Lesley Grocott, Ros Kandler, Sarah Lawrence, Catherine PangDocument6 pagesSeizure: Nick Kane, Lesley Grocott, Ros Kandler, Sarah Lawrence, Catherine PangRenard ChristianNo ratings yet
- Devries2009 Evolving Understanding ofDocument10 pagesDevries2009 Evolving Understanding ofModou NianeNo ratings yet
- Untitled 4Document1 pageUntitled 4Giga HasabiNo ratings yet
- 631-Article Text-2378-1-10-20180830Document6 pages631-Article Text-2378-1-10-20180830azizhamoudNo ratings yet
- ACNS Neonatal EEG GuidelinesDocument40 pagesACNS Neonatal EEG Guidelinesseemee23820No ratings yet
- 10 1111@j 1440-1754 1995 tb00793 X PDFDocument4 pages10 1111@j 1440-1754 1995 tb00793 X PDFNdamale NicholasNo ratings yet
- A Review of Normal Values of Infant Sleep PolysomnographyDocument6 pagesA Review of Normal Values of Infant Sleep PolysomnographyGil CLNo ratings yet
- Atypical SspeDocument2 pagesAtypical Sspenisa_neyshaaljufriNo ratings yet
- Finer, (1981) - Hypoxic-Ischemic Encephalopathy in Term Neonates Perinatal Factors and Outcome. The Journal of PediatricsDocument6 pagesFiner, (1981) - Hypoxic-Ischemic Encephalopathy in Term Neonates Perinatal Factors and Outcome. The Journal of PediatricsKatherine FernandezNo ratings yet
- Ref 7Document12 pagesRef 7Tiago BaraNo ratings yet
- Post Asphyxia MangementDocument17 pagesPost Asphyxia MangementTania MahalNo ratings yet
- Postpartum Eclampsia PDFDocument2 pagesPostpartum Eclampsia PDFMo Fadra0% (1)
- Fped 2019 00453Document7 pagesFped 2019 00453rifqiNo ratings yet
- Seminars in Fetal & Neonatal Medicine: Chakrapani Vasudevan, Malcolm LeveneDocument7 pagesSeminars in Fetal & Neonatal Medicine: Chakrapani Vasudevan, Malcolm LeveneAngelica AponteNo ratings yet
- Encefalopatia Neonatal PDFDocument13 pagesEncefalopatia Neonatal PDFVanessa RomeroNo ratings yet
- Rolul (A) EEG SI NIRS in Diagnosticul, Managmentul Si Prognosticul Convulsiilor NeonataleDocument10 pagesRolul (A) EEG SI NIRS in Diagnosticul, Managmentul Si Prognosticul Convulsiilor Neonataleandreea sfirnaciucNo ratings yet
- Anesthetic Management of A Parturient With Active Tuberculous MeningitisDocument3 pagesAnesthetic Management of A Parturient With Active Tuberculous Meningitishendri hidayatNo ratings yet
- Fetal ElectrocardiogramDocument5 pagesFetal ElectrocardiogrammariakjaimesNo ratings yet
- Echography and Doppler of the BrainFrom EverandEchography and Doppler of the BrainChiara RobbaNo ratings yet
- Fistula Kista Duktus Tiroglosus: Laporan KasusDocument6 pagesFistula Kista Duktus Tiroglosus: Laporan KasusRatnaNo ratings yet
- Dengue TropMed New Sept'12Document62 pagesDengue TropMed New Sept'12RatnaNo ratings yet
- Sepsis 2013Document42 pagesSepsis 2013RatnaNo ratings yet
- Nutricia Global Virtual Conference: Impacting Health in The New Norm With Specialized NutritionDocument9 pagesNutricia Global Virtual Conference: Impacting Health in The New Norm With Specialized NutritionRatnaNo ratings yet
- The Association of Antiepileptic Drugs With Vitamin D Status in Childhood Epilepsy December 2019 1576325924 5710734Document4 pagesThe Association of Antiepileptic Drugs With Vitamin D Status in Childhood Epilepsy December 2019 1576325924 5710734RatnaNo ratings yet
- Growth FalteringDocument56 pagesGrowth FalteringRatnaNo ratings yet
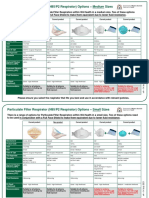
- COVID19 N95 and P2 Respirator OptionsDocument2 pagesCOVID19 N95 and P2 Respirator OptionsRatnaNo ratings yet
- 3887-Article Text-17080-1-2-20191014Document10 pages3887-Article Text-17080-1-2-20191014RatnaNo ratings yet
- Growing PainDocument7 pagesGrowing PainRatnaNo ratings yet
- Approach To Liver Function Tests in Children: Mahmood HaghighatDocument4 pagesApproach To Liver Function Tests in Children: Mahmood HaghighatRatnaNo ratings yet
- A Study of Vitamin - D Status in Epileptic Children in Age Group of 2-15 YearsDocument5 pagesA Study of Vitamin - D Status in Epileptic Children in Age Group of 2-15 YearsRatnaNo ratings yet
- Vit D and Risk FactorDocument6 pagesVit D and Risk FactorRatnaNo ratings yet
- Study of Vitamin D Levels in Epileptic Children in Age Group of 2-16 YearsDocument2 pagesStudy of Vitamin D Levels in Epileptic Children in Age Group of 2-16 YearsRatnaNo ratings yet
- Pain Monitoring ChartDocument2 pagesPain Monitoring ChartAmith VijayanNo ratings yet
- SRH 72 JamDocument3 pagesSRH 72 JamRinaldi sani NasutionNo ratings yet
- NSTPDocument3 pagesNSTPKRISTINE RIO BACSALNo ratings yet
- Extravasation of Contrast MediaDocument19 pagesExtravasation of Contrast Mediazainab sawanNo ratings yet
- Drug Induced ParkinsonismDocument9 pagesDrug Induced ParkinsonismarifbudipraNo ratings yet
- Antibiotik Bijak Pada COVID-19 (Ronald Irwanto)Document52 pagesAntibiotik Bijak Pada COVID-19 (Ronald Irwanto)Sitti marhamahNo ratings yet
- Dr. Rishank Kishore Resident: ENT & Head-Neck SurgeryDocument19 pagesDr. Rishank Kishore Resident: ENT & Head-Neck SurgeryMayur IngaleNo ratings yet
- 2020 AGEAGEING Deprescribing in Older People Approaching en of Life Development and Validation of STOPPFrail Version 2Document7 pages2020 AGEAGEING Deprescribing in Older People Approaching en of Life Development and Validation of STOPPFrail Version 2erika avelina rodriguez jaureguiNo ratings yet
- Swim Class Final Exam: Mary Donahue Welcomes You To Her Home PageDocument9 pagesSwim Class Final Exam: Mary Donahue Welcomes You To Her Home PageArk KnightNo ratings yet
- 1 Q&A Usmle Step 1Document72 pages1 Q&A Usmle Step 1Villia DamayantieNo ratings yet
- Intl Journal of Cancer - 2024 - Stier - International Anal Neoplasia Society S Consensus Guidelines For Anal CancerDocument9 pagesIntl Journal of Cancer - 2024 - Stier - International Anal Neoplasia Society S Consensus Guidelines For Anal CancercarolinaNo ratings yet
- HTP Heat Related IllnessDocument7 pagesHTP Heat Related IllnessNhadzmae Asmadul IsnainNo ratings yet
- CDU Care Plan. UTIDocument7 pagesCDU Care Plan. UTImutiso mutieNo ratings yet
- Obstructed LaborDocument41 pagesObstructed LaborHenok Y KebedeNo ratings yet
- Epidemiology Principles and Methods Prof Bhisma MurtiDocument32 pagesEpidemiology Principles and Methods Prof Bhisma Murtievy_silviania8873100% (1)
- Ortholecture 1Document102 pagesOrtholecture 1Sam Raven AndresNo ratings yet
- Bakteriološki Nalaz U Uretri Muškaraca Sa I Bez Negonoroičnog UretritisaDocument4 pagesBakteriološki Nalaz U Uretri Muškaraca Sa I Bez Negonoroičnog UretritisaNemanjaDragosavacNo ratings yet
- Malaria in PregnancyDocument17 pagesMalaria in PregnancyMwanja MosesNo ratings yet
- Bronchial AsthmaDocument21 pagesBronchial AsthmashaitabliganNo ratings yet
- Case Study Final AsthmaDocument6 pagesCase Study Final AsthmaRichelle Sandriel C. de CastroNo ratings yet
- Path GitDocument18 pagesPath Gitvnair112No ratings yet
- Centre For Clinical Interventions - Mood Management Course - Anxiety Cognitive Behavioural TherapyDocument3 pagesCentre For Clinical Interventions - Mood Management Course - Anxiety Cognitive Behavioural TherapyNatami TokieNo ratings yet
- Conjunctivitis Hordeolum ChalazionDocument52 pagesConjunctivitis Hordeolum ChalazionPatricia May CruzNo ratings yet
- World IBD Day Infographic 2019 PDFDocument1 pageWorld IBD Day Infographic 2019 PDFVasoRafaelaVakouftsiNo ratings yet
- Proceso Marc F. Udarbe: Representative CaseDocument6 pagesProceso Marc F. Udarbe: Representative CaseAlvin Germo PasuquinNo ratings yet
- Radiology Case Report - Splenic AbscessDocument6 pagesRadiology Case Report - Splenic AbscessAbeebNo ratings yet
- Pleural TapingDocument6 pagesPleural TapingLiza KameliaNo ratings yet
- Silvadene (Silver Sulfadiazine)Document1 pageSilvadene (Silver Sulfadiazine)ENo ratings yet
- Clubfoot - TalipesDocument6 pagesClubfoot - Talipess12321261112No ratings yet