Download as docx, pdf, or txt
You might also like
- Iso 15213-1-2023Document28 pagesIso 15213-1-2023JOSEPH100% (7)
- Health Declaration FormDocument3 pagesHealth Declaration FormMaja Aira BumatayNo ratings yet
- Pre-Employment Physical FormDocument1 pagePre-Employment Physical FormKarthik SNo ratings yet
- UST NSTP Medical Examination Report FormDocument1 pageUST NSTP Medical Examination Report FormFrancisQueNo ratings yet
- Application Form - Campus HiringDocument5 pagesApplication Form - Campus HiringDhanu T ANo ratings yet
- Antenatal FormDocument1 pageAntenatal Formtami_web2No ratings yet
- PHA Individual Health Profile & Assessment Form As of Oct.09, 2017Document8 pagesPHA Individual Health Profile & Assessment Form As of Oct.09, 2017Eden VblagasyNo ratings yet
- Plant Design For Slurry HandlingDocument6 pagesPlant Design For Slurry HandlingJose BustosNo ratings yet
- Metatonin & Pineal GlandDocument107 pagesMetatonin & Pineal GlandSoman100% (2)
- 70 Ebook Photography Download FreeDocument3 pages70 Ebook Photography Download Free-roger Ron Taylor-100% (3)
- Computer Project 1: Assignment 1.1Document10 pagesComputer Project 1: Assignment 1.1Nelu TurcanuNo ratings yet
- Staff Health Form: Demographic ProfileDocument3 pagesStaff Health Form: Demographic ProfileAaron Jay MondayaNo ratings yet
- New Employee Medical QuestionnaireDocument2 pagesNew Employee Medical QuestionnaireRichard R M ThodéNo ratings yet
- Pre Employment QuestionnaireDocument1 pagePre Employment Questionnaireamira.rezk1490No ratings yet
- New Employee Health QuestionnaireDocument3 pagesNew Employee Health Questionnaireb596739No ratings yet
- Pe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)Document6 pagesPe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)MoyeonieNo ratings yet
- SA04 Medical Examination Report PDFDocument4 pagesSA04 Medical Examination Report PDFSOU FEI Ang0% (1)
- LTP On Student Medical Records - Apsa Circular 8 SignedDocument3 pagesLTP On Student Medical Records - Apsa Circular 8 SignedrorororNo ratings yet
- Physical Form 2018Document2 pagesPhysical Form 2018api-247134277No ratings yet
- Pre Employment Health AssessmentDocument7 pagesPre Employment Health AssessmentMP13No ratings yet
- NEW PE FORM Bangayan Vhynee SDocument4 pagesNEW PE FORM Bangayan Vhynee SVhynee BangayanNo ratings yet
- Page 3 6 MHR PRESCREEN QUESTIONNAIREDocument5 pagesPage 3 6 MHR PRESCREEN QUESTIONNAIREMark Joel AguilaNo ratings yet
- Minor Life QDocument1 pageMinor Life QSharath_Chandh_5634No ratings yet
- Student Medical RecordDocument3 pagesStudent Medical Recordhamsa RasbiehNo ratings yet
- Child's Health Form - PDFDocument4 pagesChild's Health Form - PDFAaron Jay MondayaNo ratings yet
- Golden+Yogi+Health+Assessment+Form Doc-2Document9 pagesGolden+Yogi+Health+Assessment+Form Doc-2ohasfwaNo ratings yet
- Dengue Case ReportDocument5 pagesDengue Case Reportvicky gNo ratings yet
- Medical Form FillableDocument4 pagesMedical Form Fillablefrancislouisa4No ratings yet
- Medical Form1Document1 pageMedical Form1Saket PrasadNo ratings yet
- Full Med QuestionnaireDocument3 pagesFull Med QuestionnaireGordana ManasievaNo ratings yet
- Annex D Quick Health Assessment Form - MR VaccineDocument1 pageAnnex D Quick Health Assessment Form - MR VaccinePaluan RhuNo ratings yet
- Annex D Quick Health Assessment Form - MR VaccineDocument1 pageAnnex D Quick Health Assessment Form - MR VaccineMaria Kathrina CyraNo ratings yet
- HealthHistory Immunizations Form p2 SWTDocument1 pageHealthHistory Immunizations Form p2 SWT6jtgd5g272No ratings yet
- Application Form - Campus HiringDocument5 pagesApplication Form - Campus Hiringpawan khattarNo ratings yet
- Assessment Tool For G and DDocument1 pageAssessment Tool For G and DCarl Joshua ValerianoNo ratings yet
- Fitness Assessment Questionnaire PDFDocument4 pagesFitness Assessment Questionnaire PDFKatrina Pillagara0% (1)
- Comprehensive Adult Health HistoryDocument7 pagesComprehensive Adult Health HistoryKhirsna PasajolNo ratings yet
- Medical Questionnaire Sept 06Document2 pagesMedical Questionnaire Sept 06Rein Potential Applicant100% (1)
- LLC Health FormDocument2 pagesLLC Health Formcesar maguigadNo ratings yet
- Nfhs Student Health RecordDocument2 pagesNfhs Student Health Recordestudillojesusimo64No ratings yet
- Medical FormDocument2 pagesMedical FormHoney AliNo ratings yet
- Chaitanya Godavari Grameena Bank:: Head Office:: Guntur Medical Examination ReportDocument2 pagesChaitanya Godavari Grameena Bank:: Head Office:: Guntur Medical Examination ReportbajibabuNo ratings yet
- New Patient Application UpdatedDocument5 pagesNew Patient Application UpdatedAbdu AryaNo ratings yet
- Personal Health History: Complete Incomplete Don't Know Females Only LMP (Last Menstrual Period)Document3 pagesPersonal Health History: Complete Incomplete Don't Know Females Only LMP (Last Menstrual Period)ERICKA GRACE DA SILVANo ratings yet
- 2020 Flu Vaccination Consent FormDocument1 page2020 Flu Vaccination Consent FormJoan LeeNo ratings yet
- Med History & PE GuideDocument7 pagesMed History & PE GuideStephanie GaerlanNo ratings yet
- Student Health RecordDocument2 pagesStudent Health Recordnadhityasari28No ratings yet
- Medical Health Record 2 LONGDocument2 pagesMedical Health Record 2 LONGipanagclaire8No ratings yet
- Brendahs Medical FormDocument2 pagesBrendahs Medical FormBaluku GeofreyNo ratings yet
- Free Annual Medical ReportDocument2 pagesFree Annual Medical ReportPravin Nikhade0% (1)
- Meeting 1-General Assessment (Repaired)Document3 pagesMeeting 1-General Assessment (Repaired)Indah Yulinda PramestyNo ratings yet
- Research Proposal PresentationDocument19 pagesResearch Proposal Presentationapi-542965039No ratings yet
- Pre Medical Evaluatiom Form PFT 1 PDFDocument2 pagesPre Medical Evaluatiom Form PFT 1 PDFAIEN WENDELEIH Q. CAPINPIN100% (2)
- Medical FormsDocument5 pagesMedical FormsolandiolettyNo ratings yet
- Medical History FormDocument2 pagesMedical History FormUtkarsh LakraNo ratings yet
- Patient Registration FormDocument5 pagesPatient Registration FormCari WithrowNo ratings yet
- School Health FormDocument1 pageSchool Health Formremely marcosNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration Formlouis alvarezNo ratings yet
- Nurse HistoryDocument3 pagesNurse HistoryHAROLD ANGELESNo ratings yet
- Occupational Health Assessment Questionnaire Version 2 February 2010Document3 pagesOccupational Health Assessment Questionnaire Version 2 February 2010Cherry Mañibo100% (1)
- Uhs Form 4 Pe Form With Philhealth Number and PWD For 2024Document4 pagesUhs Form 4 Pe Form With Philhealth Number and PWD For 2024plmbsbio1No ratings yet
- BwergnwoienbDocument3 pagesBwergnwoienbpobayed154No ratings yet
- Physician's Report Form: Part A (Completed by The Applicant) 1. 2. 3Document4 pagesPhysician's Report Form: Part A (Completed by The Applicant) 1. 2. 3Arturo MBNo ratings yet
- A Simple Guide To Sexually Transmitted Infections, Diagnosis, Treatment And Related ConditionsFrom EverandA Simple Guide To Sexually Transmitted Infections, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (3)
- Class Program: Nena A. TedlosDocument6 pagesClass Program: Nena A. TedlosAaron Jay MondayaNo ratings yet
- Wali June 13Document5 pagesWali June 13Aaron Jay MondayaNo ratings yet
- Staff Health Form: Demographic ProfileDocument3 pagesStaff Health Form: Demographic ProfileAaron Jay MondayaNo ratings yet
- Child's Health Form - PDFDocument4 pagesChild's Health Form - PDFAaron Jay MondayaNo ratings yet
- Organize Before You Start WritingDocument6 pagesOrganize Before You Start WritingAaron Jay MondayaNo ratings yet
- How To Start (And Complete) A Research PaperDocument4 pagesHow To Start (And Complete) A Research PaperAaron Jay MondayaNo ratings yet
- Rodriguez, A. G. & Mckay, S. (2010) - Professional Development For Experienced Teachers Working WithDocument4 pagesRodriguez, A. G. & Mckay, S. (2010) - Professional Development For Experienced Teachers Working WithAaron Jay MondayaNo ratings yet
- Endovac BrochureDocument8 pagesEndovac BrochureGeorge MK100% (1)
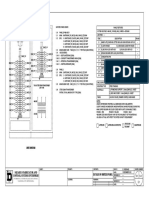
- Panel Features: Square-D Fabricator and Control Systems EnterpriseDocument1 pagePanel Features: Square-D Fabricator and Control Systems EnterpriseCallista CollectionsNo ratings yet
- Test Report CMI, 200 Amp 35kV Class "Tuf-Ex-Well II" Bushing WellDocument8 pagesTest Report CMI, 200 Amp 35kV Class "Tuf-Ex-Well II" Bushing WellCristobal BohorquezNo ratings yet
- Pizzi 1993Document8 pagesPizzi 1993jgNo ratings yet
- PPP-Eclipse-E05 Module 05 IDUsDocument11 pagesPPP-Eclipse-E05 Module 05 IDUsJervy SegarraNo ratings yet
- Kezelesi Utmutato Q3 RF 2010 AngolDocument12 pagesKezelesi Utmutato Q3 RF 2010 AngolClaudiu AdamNo ratings yet
- Scapula Setting AnaIsabel AlmeidaDocument1 pageScapula Setting AnaIsabel AlmeidaPeter ZachNo ratings yet
- The Occidental Man in Search of Human ValuesDocument11 pagesThe Occidental Man in Search of Human ValuesBen Ritche LayosNo ratings yet
- High Protein Foods List PDFDocument3 pagesHigh Protein Foods List PDFAnonymous P1FbQoqsHJ100% (1)
- Euca FBB - Jiangxi MillDocument1 pageEuca FBB - Jiangxi MillBill King0% (1)
- Metasploit FrameworkDocument1 pageMetasploit FrameworkPAUL VINCENT FAJARDONo ratings yet
- En The New Polo 1.0 TSI, Petrol Engine 85 KW Seven-Speed Dual-Clutch Gearbox (DS PDFDocument1 pageEn The New Polo 1.0 TSI, Petrol Engine 85 KW Seven-Speed Dual-Clutch Gearbox (DS PDFrobbertmdNo ratings yet
- Lab ManualDocument41 pagesLab Manualprojectapply2023No ratings yet
- Analisis Potensi Dan Tingkat Pemanfaatan Sumberdaya Ikan Di Perairan Kabupaten Bangka SelatanDocument12 pagesAnalisis Potensi Dan Tingkat Pemanfaatan Sumberdaya Ikan Di Perairan Kabupaten Bangka SelatanShope IkmaNo ratings yet
- Music Therapy When Death Is Imminent - A Phenomenological InquiryDocument32 pagesMusic Therapy When Death Is Imminent - A Phenomenological InquiryJuan Luis Köstner MartinoNo ratings yet
- ME Engines: Electronic Headway of Two-Stroke DieselsDocument4 pagesME Engines: Electronic Headway of Two-Stroke DieselsSalwan ShubhamNo ratings yet
- Assignment 3: Task #1 Has (10 Parts) That Corresponds To CLO # 2 For A Total of 30 PointsDocument2 pagesAssignment 3: Task #1 Has (10 Parts) That Corresponds To CLO # 2 For A Total of 30 PointsWaqas AliNo ratings yet
- Cryolite JM File 2011Document5 pagesCryolite JM File 2011mutemuNo ratings yet
- MotiliumDocument5 pagesMotiliumAkram KhanNo ratings yet
- Daftar Harga 2021 (Abjad)Document9 pagesDaftar Harga 2021 (Abjad)Arahmaniansyah HenkzNo ratings yet
- Suzuki vs125 ManualDocument22 pagesSuzuki vs125 ManualHaram JadahNo ratings yet
- Bas920 DatasheetDocument5 pagesBas920 Datasheetd_macuraNo ratings yet
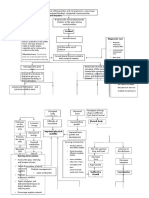
- Pathway - Skoliosis GROUPDocument12 pagesPathway - Skoliosis GROUPAnonymous NZTQVgjaNo ratings yet
- Tulip CRP TurbiDocument1 pageTulip CRP Turbirahul kumarNo ratings yet
- Plag - ReportDocument6 pagesPlag - ReportMehedi HasanNo ratings yet