
Malignant Transformation of Oral Submucous Fibrosis in Taiwan: A Nationwide Population-Based Retrospective Cohort Study
Malignant Transformation of Oral Submucous Fibrosis in Taiwan: A Nationwide Population-Based Retrospective Cohort Study
You might also like
- Issue Trees - The Definitive Guide (+in-Depth Examples) - Crafting CasesDocument147 pagesIssue Trees - The Definitive Guide (+in-Depth Examples) - Crafting CasesShubham Shah100% (1)
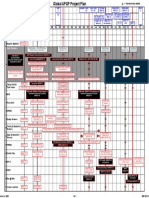
- GM 1927 01 Project PlanDocument1 pageGM 1927 01 Project Planmark100% (2)
- BMC Cancer: Prognostic Factors Associated With The Survival of Oral and Pharyngeal Carcinoma in TaiwanDocument11 pagesBMC Cancer: Prognostic Factors Associated With The Survival of Oral and Pharyngeal Carcinoma in TaiwanLinaena MericyNo ratings yet
- Medoralv16 I4 p473Document5 pagesMedoralv16 I4 p473AbhinavNo ratings yet
- Oral SCC SurvivalDocument8 pagesOral SCC Survivalmichaeljt_md6463No ratings yet
- Clinico-Pathological Study of Oral CancersDocument4 pagesClinico-Pathological Study of Oral CancersIOSRjournalNo ratings yet
- Factors Associated With Delay in The Diagnosis of Oral CancerDocument6 pagesFactors Associated With Delay in The Diagnosis of Oral CancerAshu TyagiNo ratings yet
- Effect of Periodontitis and Scaling and Root Planing On Risk of Pharyngeal Cancer: A Nested Case-Control StudyDocument12 pagesEffect of Periodontitis and Scaling and Root Planing On Risk of Pharyngeal Cancer: A Nested Case-Control StudyDr.Niveditha SNo ratings yet
- 2020 Increased Risk of Developing Dental Diseases in Patients With Primary Sjögren's SyndromeDocument13 pages2020 Increased Risk of Developing Dental Diseases in Patients With Primary Sjögren's SyndromemrsilNo ratings yet
- Autofluorescence 1Document18 pagesAutofluorescence 1Agache AnamariaNo ratings yet
- Introduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"Document11 pagesIntroduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"jesus ulises estrada cantuNo ratings yet
- Research 08Document18 pagesResearch 08Nandini SeetharamanNo ratings yet
- Brouns 2013Document18 pagesBrouns 2013s7ybkjhb44No ratings yet
- Risk Factors of Oral Cancer-A Hospital Based Case Control StudyDocument6 pagesRisk Factors of Oral Cancer-A Hospital Based Case Control StudyDevica DR PutriNo ratings yet
- Pharmaceutical Sciences: Analysis of Oral Submucous Fibrosis With and Without Associated Oral Squamous Cell CarcinomaDocument5 pagesPharmaceutical Sciences: Analysis of Oral Submucous Fibrosis With and Without Associated Oral Squamous Cell CarcinomaiajpsNo ratings yet
- Significantly Higher Frequencies of Hematinic Deficiencies and Hyperhomocysteinemia in Oral Precancer PatientsDocument9 pagesSignificantly Higher Frequencies of Hematinic Deficiencies and Hyperhomocysteinemia in Oral Precancer PatientsayondaNo ratings yet
- Lingen Et Al-2011-Oral DiseasesDocument16 pagesLingen Et Al-2011-Oral DiseasesSAMUEL ESCARESNo ratings yet
- Hed 44 1481Document11 pagesHed 44 1481dayllyn iglesiasNo ratings yet
- JHeadNeckPhysiciansSurg4129-194289 052348Document6 pagesJHeadNeckPhysiciansSurg4129-194289 052348Javeria MNo ratings yet
- Riginal Research: Journal of Advanced Medical and Dental Sciences ResearchDocument3 pagesRiginal Research: Journal of Advanced Medical and Dental Sciences Researchshivam sethiNo ratings yet
- Self-Induced Vomiting and Dental Erosion - A Clinical Study: Researcharticle Open AccessDocument7 pagesSelf-Induced Vomiting and Dental Erosion - A Clinical Study: Researcharticle Open AccessIonutz VargaNo ratings yet
- Hed 26006Document17 pagesHed 26006MARITZA GARCIA JIMENEZNo ratings yet
- Yuh 2014Document10 pagesYuh 2014Celyne DavoglioNo ratings yet
- Oral Cancer Literature ReviewDocument5 pagesOral Cancer Literature Reviewjsmyxkvkg100% (1)
- Zhou 2008Document5 pagesZhou 2008DIVYABOSENo ratings yet
- Hiv 1 PDFDocument13 pagesHiv 1 PDFmaridaNo ratings yet
- Anaerobic BacteriaDocument9 pagesAnaerobic BacteriaKali corgiNo ratings yet
- Bassin 2006Document8 pagesBassin 2006emirsolehloveNo ratings yet
- Public Health 309Document5 pagesPublic Health 309Blue TechNo ratings yet
- J Ajog 2009 10 892Document8 pagesJ Ajog 2009 10 892mapecorelli2626No ratings yet
- Medoral 29 E135Document10 pagesMedoral 29 E135Maria CorenaNo ratings yet
- 2019 Article 47029Document7 pages2019 Article 47029ccasta12No ratings yet
- Chemotherapy-Associated Oral Sequelae in Patients With Cancers Outside The Head and Neck RegionDocument10 pagesChemotherapy-Associated Oral Sequelae in Patients With Cancers Outside The Head and Neck RegionNndaydnaNo ratings yet
- Global Burden of Severe Periodontitis in 1990-2010: A Systematic Review and Meta-RegressionDocument10 pagesGlobal Burden of Severe Periodontitis in 1990-2010: A Systematic Review and Meta-RegressionRaul CamargoNo ratings yet
- Assessment of Haematological Parameter and Liver Enzyme Among Hepatitis B Infected Blood DonorsDocument9 pagesAssessment of Haematological Parameter and Liver Enzyme Among Hepatitis B Infected Blood DonorsKIU PUBLICATION AND EXTENSIONNo ratings yet
- 1 s2.0 S0923753419374125 MainDocument7 pages1 s2.0 S0923753419374125 MainGabriela MonteiroNo ratings yet
- Pjms 29 1112Document4 pagesPjms 29 1112Diana IancuNo ratings yet
- Oral Diseases - 2020 - Zhang - Using Next Generation Sequencing To Detect Oral Microbiome Change Following PeriodontalDocument17 pagesOral Diseases - 2020 - Zhang - Using Next Generation Sequencing To Detect Oral Microbiome Change Following PeriodontalmmputraNo ratings yet
- Estudi de Lesiones Katarzyna PDFDocument8 pagesEstudi de Lesiones Katarzyna PDFpaolaNo ratings yet
- Oral CancerDocument6 pagesOral CancerGhege GuntaranNo ratings yet
- Dental Utilization and Expenditures by Children With AutismDocument5 pagesDental Utilization and Expenditures by Children With AutismPoli BMNo ratings yet
- Jurnal THTDocument6 pagesJurnal THTFeby Arin BindaNo ratings yet
- Critical Reviews in Oral Biology & MedicineDocument8 pagesCritical Reviews in Oral Biology & MedicineBimalKrishnaNo ratings yet
- 1 s2.0 S1368837520304838 MainDocument6 pages1 s2.0 S1368837520304838 MainMariuxi GómezNo ratings yet
- Eke 2012Document8 pagesEke 2012Goja AdrianNo ratings yet
- Thematic Abstract Review: Systemic Factors Affecting Implant Survival?Document3 pagesThematic Abstract Review: Systemic Factors Affecting Implant Survival?Natalia Camila Rodríguez LatorreNo ratings yet
- Frequency of Patients Presenting With Recurrent Aphthous Stomatitis: A Pilot StudyDocument4 pagesFrequency of Patients Presenting With Recurrent Aphthous Stomatitis: A Pilot StudyAden DhenNo ratings yet
- 1957-63 2.19 Wan Maria Nabillah GhaniDocument7 pages1957-63 2.19 Wan Maria Nabillah GhaniNursyafiq Ali ShibramulisiNo ratings yet
- Pinto 2020Document14 pagesPinto 2020s7ybkjhb44No ratings yet
- Lee 2019Document10 pagesLee 2019shehla khanNo ratings yet
- Mikroba KankerDocument12 pagesMikroba KankerSilpi HamidiyahNo ratings yet
- 10.1007@s00405 020 06036 1Document10 pages10.1007@s00405 020 06036 1yusra ghayoorNo ratings yet
- Association Between Periodontal Health andDocument7 pagesAssociation Between Periodontal Health andTran DuongNo ratings yet
- 6IJAERS 1020202 Clinical PDFDocument7 pages6IJAERS 1020202 Clinical PDFIJAERS JOURNALNo ratings yet
- Journal Pone 0091059Document5 pagesJournal Pone 0091059AgusBhaktiNo ratings yet
- Clinical Evaluation of Halitosis Patients in KoreaDocument6 pagesClinical Evaluation of Halitosis Patients in KoreaBilly TrầnNo ratings yet
- Risk Factors For Ocular Surface Squamous Neoplasia in Kenya: A Case - Control StudyDocument9 pagesRisk Factors For Ocular Surface Squamous Neoplasia in Kenya: A Case - Control StudyGino VitteriNo ratings yet
- Economic and Survival Burden of Dysphagia Among Inpatients in The United StatesDocument7 pagesEconomic and Survival Burden of Dysphagia Among Inpatients in The United StatesClaudia Lorena MedinaNo ratings yet
- Shanaz FinalDocument7 pagesShanaz FinalDimaz ImanNo ratings yet
- Archive of SID: Oral Cancer Knowledge Among Patients Referred To Mashhad Dental School, IranDocument6 pagesArchive of SID: Oral Cancer Knowledge Among Patients Referred To Mashhad Dental School, Iranhajer hNo ratings yet
- Prevalence and Associated Factors of Blepharoptosis in Korean Adult Population: The Korea National Health and Nutrition Examination Survey 2008-2011Document7 pagesPrevalence and Associated Factors of Blepharoptosis in Korean Adult Population: The Korea National Health and Nutrition Examination Survey 2008-2011AndrewNo ratings yet
- Diagnostic Problems in Tumors of Head and Neck: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Head and Neck: Selected TopicsRating: 5 out of 5 stars5/5 (1)
- Pindborg 1984Document7 pagesPindborg 1984DIVYABOSENo ratings yet
- Pindborg 1967Document6 pagesPindborg 1967DIVYABOSENo ratings yet
- Chaturvedi 2017Document25 pagesChaturvedi 2017DIVYABOSENo ratings yet
- Better Grade of Tumor Differentiation of Oral Squamous Cell Carcinoma Arising in Background of Oral Submucous FibrosisDocument5 pagesBetter Grade of Tumor Differentiation of Oral Squamous Cell Carcinoma Arising in Background of Oral Submucous FibrosisDIVYABOSENo ratings yet
- Ehlers Danlos SyndromeDocument18 pagesEhlers Danlos SyndromeDIVYABOSENo ratings yet
- Unusual Encroachers in OKCDocument3 pagesUnusual Encroachers in OKCDIVYABOSENo ratings yet
- The Pathogenesis of Systemic Sclerosis: FurtherDocument31 pagesThe Pathogenesis of Systemic Sclerosis: FurtherDIVYABOSENo ratings yet
- Zhou 2008Document5 pagesZhou 2008DIVYABOSENo ratings yet
- Periodontal Ehlers-DanlosDocument7 pagesPeriodontal Ehlers-DanlosDIVYABOSENo ratings yet
- American Board of Forensic Odontology (ABFO) Body Identification Information & GuidelinesDocument12 pagesAmerican Board of Forensic Odontology (ABFO) Body Identification Information & GuidelinesDIVYABOSENo ratings yet
- Permanent Mandibular II MolarDocument24 pagesPermanent Mandibular II MolarDIVYABOSENo ratings yet
- Statement of Claim Form PDFDocument3 pagesStatement of Claim Form PDFWalla MahmoudNo ratings yet
- 3VA22255HL420AA0 Datasheet enDocument7 pages3VA22255HL420AA0 Datasheet enBensonNo ratings yet
- Declaration of Conformity For Restriction of Hazardous Substances (Rohs)Document1 pageDeclaration of Conformity For Restriction of Hazardous Substances (Rohs)Yogesh KatyarmalNo ratings yet
- Milling MachinesDocument39 pagesMilling MachinesSahil Sheth0% (1)
- Ch6-Mechanical PropertiesDocument39 pagesCh6-Mechanical PropertiesSaif AlbaddawiNo ratings yet
- Final ProjectDocument6 pagesFinal ProjectAmmar HussainNo ratings yet
- Fixturlaser Documenter User ManualDocument58 pagesFixturlaser Documenter User ManualMicroficheNo ratings yet
- PreloadDocument21 pagesPreloadjainshani2No ratings yet
- Internship 2021Document25 pagesInternship 2021PRAGYA CHANSORIYANo ratings yet
- Xu and Zhang (2009) (ASCE) GT.1943-5606 - Dam BreachDocument14 pagesXu and Zhang (2009) (ASCE) GT.1943-5606 - Dam BreachCharumitra YadavNo ratings yet
- Rw15 ManualDocument314 pagesRw15 ManualpedrogerardohjNo ratings yet
- Profile of Dr. APJ Abdul KalamDocument3 pagesProfile of Dr. APJ Abdul KalammukeshNo ratings yet
- Chapter 24 Notes (Student)Document11 pagesChapter 24 Notes (Student)Regina LinNo ratings yet
- SEAS RSRC 57bfe799620e0Document4 pagesSEAS RSRC 57bfe799620e0WunNaNo ratings yet
- Backtracking - Set 2 (Rat in A Maze) - GeeksforGeeksDocument7 pagesBacktracking - Set 2 (Rat in A Maze) - GeeksforGeeksAtul GargNo ratings yet
- Bundle Bundle Js LICENSEDocument11 pagesBundle Bundle Js LICENSE333surimaNo ratings yet
- ABB Unit Trip EMAX PR112-PD PDFDocument27 pagesABB Unit Trip EMAX PR112-PD PDFPedro MartinsNo ratings yet
- Brown Eaod8 PPT 08Document40 pagesBrown Eaod8 PPT 08qq2pmmj4gpNo ratings yet
- TBG Catalog Vol 6Document64 pagesTBG Catalog Vol 6GeorgeNo ratings yet
- Air Equipment Compressors Compressor 250 300CFM D XAS 125DD Operation ManualDocument34 pagesAir Equipment Compressors Compressor 250 300CFM D XAS 125DD Operation ManualFloyd MG100% (1)
- SPE 127422 Cement-Sheath Wellbore Integrity For CO Injection and Storage WellsDocument11 pagesSPE 127422 Cement-Sheath Wellbore Integrity For CO Injection and Storage Wellsadvantage025No ratings yet
- Chapter 5: Children'S Fiction: Lesson 1: Worlds and VoicesDocument5 pagesChapter 5: Children'S Fiction: Lesson 1: Worlds and VoicesRaquel LimboNo ratings yet
- Mechanics of Materials 9th Edition Hibbeler Solutions ManualDocument35 pagesMechanics of Materials 9th Edition Hibbeler Solutions Manualronbowmantdd2bh100% (29)
- Universiti Pendidikan Sultan Idris Mid-Term Test SEMESTER 1 SESSION 2020/2021Document3 pagesUniversiti Pendidikan Sultan Idris Mid-Term Test SEMESTER 1 SESSION 2020/2021rusnah chungNo ratings yet
- Case Study - Box-JenkinsDocument10 pagesCase Study - Box-JenkinsVedant MishraNo ratings yet
- Computer Graphics - Chapter 3 (1) - 2Document35 pagesComputer Graphics - Chapter 3 (1) - 2Sương TrầnNo ratings yet
- Genetic Mutation LAB SHEET REVISEDDocument2 pagesGenetic Mutation LAB SHEET REVISEDyusufoyololaNo ratings yet
- Gujarat Technological UniversityDocument2 pagesGujarat Technological Universityvasava dipakNo ratings yet


































































































Download as pdf or txt
You might also like
- Issue Trees - The Definitive Guide (+in-Depth Examples) - Crafting CasesDocument147 pagesIssue Trees - The Definitive Guide (+in-Depth Examples) - Crafting CasesShubham Shah100% (1)
- GM 1927 01 Project PlanDocument1 pageGM 1927 01 Project Planmark100% (2)
- BMC Cancer: Prognostic Factors Associated With The Survival of Oral and Pharyngeal Carcinoma in TaiwanDocument11 pagesBMC Cancer: Prognostic Factors Associated With The Survival of Oral and Pharyngeal Carcinoma in TaiwanLinaena MericyNo ratings yet
- Medoralv16 I4 p473Document5 pagesMedoralv16 I4 p473AbhinavNo ratings yet
- Oral SCC SurvivalDocument8 pagesOral SCC Survivalmichaeljt_md6463No ratings yet
- Clinico-Pathological Study of Oral CancersDocument4 pagesClinico-Pathological Study of Oral CancersIOSRjournalNo ratings yet
- Factors Associated With Delay in The Diagnosis of Oral CancerDocument6 pagesFactors Associated With Delay in The Diagnosis of Oral CancerAshu TyagiNo ratings yet
- Effect of Periodontitis and Scaling and Root Planing On Risk of Pharyngeal Cancer: A Nested Case-Control StudyDocument12 pagesEffect of Periodontitis and Scaling and Root Planing On Risk of Pharyngeal Cancer: A Nested Case-Control StudyDr.Niveditha SNo ratings yet
- 2020 Increased Risk of Developing Dental Diseases in Patients With Primary Sjögren's SyndromeDocument13 pages2020 Increased Risk of Developing Dental Diseases in Patients With Primary Sjögren's SyndromemrsilNo ratings yet
- Autofluorescence 1Document18 pagesAutofluorescence 1Agache AnamariaNo ratings yet
- Introduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"Document11 pagesIntroduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"jesus ulises estrada cantuNo ratings yet
- Research 08Document18 pagesResearch 08Nandini SeetharamanNo ratings yet
- Brouns 2013Document18 pagesBrouns 2013s7ybkjhb44No ratings yet
- Risk Factors of Oral Cancer-A Hospital Based Case Control StudyDocument6 pagesRisk Factors of Oral Cancer-A Hospital Based Case Control StudyDevica DR PutriNo ratings yet
- Pharmaceutical Sciences: Analysis of Oral Submucous Fibrosis With and Without Associated Oral Squamous Cell CarcinomaDocument5 pagesPharmaceutical Sciences: Analysis of Oral Submucous Fibrosis With and Without Associated Oral Squamous Cell CarcinomaiajpsNo ratings yet
- Significantly Higher Frequencies of Hematinic Deficiencies and Hyperhomocysteinemia in Oral Precancer PatientsDocument9 pagesSignificantly Higher Frequencies of Hematinic Deficiencies and Hyperhomocysteinemia in Oral Precancer PatientsayondaNo ratings yet
- Lingen Et Al-2011-Oral DiseasesDocument16 pagesLingen Et Al-2011-Oral DiseasesSAMUEL ESCARESNo ratings yet
- Hed 44 1481Document11 pagesHed 44 1481dayllyn iglesiasNo ratings yet
- JHeadNeckPhysiciansSurg4129-194289 052348Document6 pagesJHeadNeckPhysiciansSurg4129-194289 052348Javeria MNo ratings yet
- Riginal Research: Journal of Advanced Medical and Dental Sciences ResearchDocument3 pagesRiginal Research: Journal of Advanced Medical and Dental Sciences Researchshivam sethiNo ratings yet
- Self-Induced Vomiting and Dental Erosion - A Clinical Study: Researcharticle Open AccessDocument7 pagesSelf-Induced Vomiting and Dental Erosion - A Clinical Study: Researcharticle Open AccessIonutz VargaNo ratings yet
- Hed 26006Document17 pagesHed 26006MARITZA GARCIA JIMENEZNo ratings yet
- Yuh 2014Document10 pagesYuh 2014Celyne DavoglioNo ratings yet
- Oral Cancer Literature ReviewDocument5 pagesOral Cancer Literature Reviewjsmyxkvkg100% (1)
- Zhou 2008Document5 pagesZhou 2008DIVYABOSENo ratings yet
- Hiv 1 PDFDocument13 pagesHiv 1 PDFmaridaNo ratings yet
- Anaerobic BacteriaDocument9 pagesAnaerobic BacteriaKali corgiNo ratings yet
- Bassin 2006Document8 pagesBassin 2006emirsolehloveNo ratings yet
- Public Health 309Document5 pagesPublic Health 309Blue TechNo ratings yet
- J Ajog 2009 10 892Document8 pagesJ Ajog 2009 10 892mapecorelli2626No ratings yet
- Medoral 29 E135Document10 pagesMedoral 29 E135Maria CorenaNo ratings yet
- 2019 Article 47029Document7 pages2019 Article 47029ccasta12No ratings yet
- Chemotherapy-Associated Oral Sequelae in Patients With Cancers Outside The Head and Neck RegionDocument10 pagesChemotherapy-Associated Oral Sequelae in Patients With Cancers Outside The Head and Neck RegionNndaydnaNo ratings yet
- Global Burden of Severe Periodontitis in 1990-2010: A Systematic Review and Meta-RegressionDocument10 pagesGlobal Burden of Severe Periodontitis in 1990-2010: A Systematic Review and Meta-RegressionRaul CamargoNo ratings yet
- Assessment of Haematological Parameter and Liver Enzyme Among Hepatitis B Infected Blood DonorsDocument9 pagesAssessment of Haematological Parameter and Liver Enzyme Among Hepatitis B Infected Blood DonorsKIU PUBLICATION AND EXTENSIONNo ratings yet
- 1 s2.0 S0923753419374125 MainDocument7 pages1 s2.0 S0923753419374125 MainGabriela MonteiroNo ratings yet
- Pjms 29 1112Document4 pagesPjms 29 1112Diana IancuNo ratings yet
- Oral Diseases - 2020 - Zhang - Using Next Generation Sequencing To Detect Oral Microbiome Change Following PeriodontalDocument17 pagesOral Diseases - 2020 - Zhang - Using Next Generation Sequencing To Detect Oral Microbiome Change Following PeriodontalmmputraNo ratings yet
- Estudi de Lesiones Katarzyna PDFDocument8 pagesEstudi de Lesiones Katarzyna PDFpaolaNo ratings yet
- Oral CancerDocument6 pagesOral CancerGhege GuntaranNo ratings yet
- Dental Utilization and Expenditures by Children With AutismDocument5 pagesDental Utilization and Expenditures by Children With AutismPoli BMNo ratings yet
- Jurnal THTDocument6 pagesJurnal THTFeby Arin BindaNo ratings yet
- Critical Reviews in Oral Biology & MedicineDocument8 pagesCritical Reviews in Oral Biology & MedicineBimalKrishnaNo ratings yet
- 1 s2.0 S1368837520304838 MainDocument6 pages1 s2.0 S1368837520304838 MainMariuxi GómezNo ratings yet
- Eke 2012Document8 pagesEke 2012Goja AdrianNo ratings yet
- Thematic Abstract Review: Systemic Factors Affecting Implant Survival?Document3 pagesThematic Abstract Review: Systemic Factors Affecting Implant Survival?Natalia Camila Rodríguez LatorreNo ratings yet
- Frequency of Patients Presenting With Recurrent Aphthous Stomatitis: A Pilot StudyDocument4 pagesFrequency of Patients Presenting With Recurrent Aphthous Stomatitis: A Pilot StudyAden DhenNo ratings yet
- 1957-63 2.19 Wan Maria Nabillah GhaniDocument7 pages1957-63 2.19 Wan Maria Nabillah GhaniNursyafiq Ali ShibramulisiNo ratings yet
- Pinto 2020Document14 pagesPinto 2020s7ybkjhb44No ratings yet
- Lee 2019Document10 pagesLee 2019shehla khanNo ratings yet
- Mikroba KankerDocument12 pagesMikroba KankerSilpi HamidiyahNo ratings yet
- 10.1007@s00405 020 06036 1Document10 pages10.1007@s00405 020 06036 1yusra ghayoorNo ratings yet
- Association Between Periodontal Health andDocument7 pagesAssociation Between Periodontal Health andTran DuongNo ratings yet
- 6IJAERS 1020202 Clinical PDFDocument7 pages6IJAERS 1020202 Clinical PDFIJAERS JOURNALNo ratings yet
- Journal Pone 0091059Document5 pagesJournal Pone 0091059AgusBhaktiNo ratings yet
- Clinical Evaluation of Halitosis Patients in KoreaDocument6 pagesClinical Evaluation of Halitosis Patients in KoreaBilly TrầnNo ratings yet
- Risk Factors For Ocular Surface Squamous Neoplasia in Kenya: A Case - Control StudyDocument9 pagesRisk Factors For Ocular Surface Squamous Neoplasia in Kenya: A Case - Control StudyGino VitteriNo ratings yet
- Economic and Survival Burden of Dysphagia Among Inpatients in The United StatesDocument7 pagesEconomic and Survival Burden of Dysphagia Among Inpatients in The United StatesClaudia Lorena MedinaNo ratings yet
- Shanaz FinalDocument7 pagesShanaz FinalDimaz ImanNo ratings yet
- Archive of SID: Oral Cancer Knowledge Among Patients Referred To Mashhad Dental School, IranDocument6 pagesArchive of SID: Oral Cancer Knowledge Among Patients Referred To Mashhad Dental School, Iranhajer hNo ratings yet
- Prevalence and Associated Factors of Blepharoptosis in Korean Adult Population: The Korea National Health and Nutrition Examination Survey 2008-2011Document7 pagesPrevalence and Associated Factors of Blepharoptosis in Korean Adult Population: The Korea National Health and Nutrition Examination Survey 2008-2011AndrewNo ratings yet
- Diagnostic Problems in Tumors of Head and Neck: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Head and Neck: Selected TopicsRating: 5 out of 5 stars5/5 (1)
- Pindborg 1984Document7 pagesPindborg 1984DIVYABOSENo ratings yet
- Pindborg 1967Document6 pagesPindborg 1967DIVYABOSENo ratings yet
- Chaturvedi 2017Document25 pagesChaturvedi 2017DIVYABOSENo ratings yet
- Better Grade of Tumor Differentiation of Oral Squamous Cell Carcinoma Arising in Background of Oral Submucous FibrosisDocument5 pagesBetter Grade of Tumor Differentiation of Oral Squamous Cell Carcinoma Arising in Background of Oral Submucous FibrosisDIVYABOSENo ratings yet
- Ehlers Danlos SyndromeDocument18 pagesEhlers Danlos SyndromeDIVYABOSENo ratings yet
- Unusual Encroachers in OKCDocument3 pagesUnusual Encroachers in OKCDIVYABOSENo ratings yet
- The Pathogenesis of Systemic Sclerosis: FurtherDocument31 pagesThe Pathogenesis of Systemic Sclerosis: FurtherDIVYABOSENo ratings yet
- Zhou 2008Document5 pagesZhou 2008DIVYABOSENo ratings yet
- Periodontal Ehlers-DanlosDocument7 pagesPeriodontal Ehlers-DanlosDIVYABOSENo ratings yet
- American Board of Forensic Odontology (ABFO) Body Identification Information & GuidelinesDocument12 pagesAmerican Board of Forensic Odontology (ABFO) Body Identification Information & GuidelinesDIVYABOSENo ratings yet
- Permanent Mandibular II MolarDocument24 pagesPermanent Mandibular II MolarDIVYABOSENo ratings yet
- Statement of Claim Form PDFDocument3 pagesStatement of Claim Form PDFWalla MahmoudNo ratings yet
- 3VA22255HL420AA0 Datasheet enDocument7 pages3VA22255HL420AA0 Datasheet enBensonNo ratings yet
- Declaration of Conformity For Restriction of Hazardous Substances (Rohs)Document1 pageDeclaration of Conformity For Restriction of Hazardous Substances (Rohs)Yogesh KatyarmalNo ratings yet
- Milling MachinesDocument39 pagesMilling MachinesSahil Sheth0% (1)
- Ch6-Mechanical PropertiesDocument39 pagesCh6-Mechanical PropertiesSaif AlbaddawiNo ratings yet
- Final ProjectDocument6 pagesFinal ProjectAmmar HussainNo ratings yet
- Fixturlaser Documenter User ManualDocument58 pagesFixturlaser Documenter User ManualMicroficheNo ratings yet
- PreloadDocument21 pagesPreloadjainshani2No ratings yet
- Internship 2021Document25 pagesInternship 2021PRAGYA CHANSORIYANo ratings yet
- Xu and Zhang (2009) (ASCE) GT.1943-5606 - Dam BreachDocument14 pagesXu and Zhang (2009) (ASCE) GT.1943-5606 - Dam BreachCharumitra YadavNo ratings yet
- Rw15 ManualDocument314 pagesRw15 ManualpedrogerardohjNo ratings yet
- Profile of Dr. APJ Abdul KalamDocument3 pagesProfile of Dr. APJ Abdul KalammukeshNo ratings yet
- Chapter 24 Notes (Student)Document11 pagesChapter 24 Notes (Student)Regina LinNo ratings yet
- SEAS RSRC 57bfe799620e0Document4 pagesSEAS RSRC 57bfe799620e0WunNaNo ratings yet
- Backtracking - Set 2 (Rat in A Maze) - GeeksforGeeksDocument7 pagesBacktracking - Set 2 (Rat in A Maze) - GeeksforGeeksAtul GargNo ratings yet
- Bundle Bundle Js LICENSEDocument11 pagesBundle Bundle Js LICENSE333surimaNo ratings yet
- ABB Unit Trip EMAX PR112-PD PDFDocument27 pagesABB Unit Trip EMAX PR112-PD PDFPedro MartinsNo ratings yet
- Brown Eaod8 PPT 08Document40 pagesBrown Eaod8 PPT 08qq2pmmj4gpNo ratings yet
- TBG Catalog Vol 6Document64 pagesTBG Catalog Vol 6GeorgeNo ratings yet
- Air Equipment Compressors Compressor 250 300CFM D XAS 125DD Operation ManualDocument34 pagesAir Equipment Compressors Compressor 250 300CFM D XAS 125DD Operation ManualFloyd MG100% (1)
- SPE 127422 Cement-Sheath Wellbore Integrity For CO Injection and Storage WellsDocument11 pagesSPE 127422 Cement-Sheath Wellbore Integrity For CO Injection and Storage Wellsadvantage025No ratings yet
- Chapter 5: Children'S Fiction: Lesson 1: Worlds and VoicesDocument5 pagesChapter 5: Children'S Fiction: Lesson 1: Worlds and VoicesRaquel LimboNo ratings yet
- Mechanics of Materials 9th Edition Hibbeler Solutions ManualDocument35 pagesMechanics of Materials 9th Edition Hibbeler Solutions Manualronbowmantdd2bh100% (29)
- Universiti Pendidikan Sultan Idris Mid-Term Test SEMESTER 1 SESSION 2020/2021Document3 pagesUniversiti Pendidikan Sultan Idris Mid-Term Test SEMESTER 1 SESSION 2020/2021rusnah chungNo ratings yet
- Case Study - Box-JenkinsDocument10 pagesCase Study - Box-JenkinsVedant MishraNo ratings yet
- Computer Graphics - Chapter 3 (1) - 2Document35 pagesComputer Graphics - Chapter 3 (1) - 2Sương TrầnNo ratings yet
- Genetic Mutation LAB SHEET REVISEDDocument2 pagesGenetic Mutation LAB SHEET REVISEDyusufoyololaNo ratings yet
- Gujarat Technological UniversityDocument2 pagesGujarat Technological Universityvasava dipakNo ratings yet