Download as docx, pdf, or txt
You might also like
- Nursing Diagnosis of Prostate CancerDocument3 pagesNursing Diagnosis of Prostate CancerSyafiqAzizi100% (1)
- Sample Birthing PlanDocument2 pagesSample Birthing PlanChuohNo ratings yet
- Case Scenario: Prostate CancerDocument5 pagesCase Scenario: Prostate Cancer24 PAULINO ALDRIN MUJARNo ratings yet
- Urinary Incontinence Nursing ManagementDocument3 pagesUrinary Incontinence Nursing ManagementRnspeakcomNo ratings yet
- Qi Project PaperDocument8 pagesQi Project Paperapi-380333919No ratings yet
- Nursing Care Plan (NCP) For A Patient With Acute Renal FailureDocument3 pagesNursing Care Plan (NCP) For A Patient With Acute Renal FailureKian HerreraNo ratings yet
- Group-5 NCM-107 NCPDocument4 pagesGroup-5 NCM-107 NCPbulok netflakes100% (1)
- Deficient Knowledge Related To Urinary Tract Infection: "Di Ako Aware About Sa UTI"as Verbalized by The ClientDocument2 pagesDeficient Knowledge Related To Urinary Tract Infection: "Di Ako Aware About Sa UTI"as Verbalized by The ClientSeanmarie CabralesNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Goals Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Goals Intervention Rationale EvaluationLeizel ApolonioNo ratings yet
- NCP Metro San JoseDocument8 pagesNCP Metro San JosePrincess NavarroNo ratings yet
- NCPDocument2 pagesNCPbulok netflakesNo ratings yet
- Assessment Diagnosis Scientific Explanatation Planning Interventions Rationale EvaluationDocument2 pagesAssessment Diagnosis Scientific Explanatation Planning Interventions Rationale EvaluationLatrell GelacioNo ratings yet
- F. NCP ProperDocument4 pagesF. NCP ProperAle SandraNo ratings yet
- NCP BPHDocument1 pageNCP BPHyasiraNo ratings yet
- Maraming Tubig at Kakain NG Prutas para Makadumi Ako."Document2 pagesMaraming Tubig at Kakain NG Prutas para Makadumi Ako."Cayla Mae CarlosNo ratings yet
- Prostatic CancerDocument3 pagesProstatic CancerShakour El seifyNo ratings yet
- Institute of Nursing and Allied Health Education: Cabanatuan City, Nueva Ecija, Philippines 3100Document14 pagesInstitute of Nursing and Allied Health Education: Cabanatuan City, Nueva Ecija, Philippines 3100Potato BananaNo ratings yet
- Combine Bladder Irrigation Post Mortem Special MouthDocument88 pagesCombine Bladder Irrigation Post Mortem Special MouthJannen CasasNo ratings yet
- Closed Bladder Irrigation - Prodecure ManualDocument12 pagesClosed Bladder Irrigation - Prodecure ManualJannen CasasNo ratings yet
- NCP - Mod9Document3 pagesNCP - Mod9designericlelynsoronioNo ratings yet
- Nursing InterventionDocument3 pagesNursing InterventionElaine Marie SeraficaNo ratings yet
- Surgical NCP DRUG STUDY PATHOPHYSIOLOGYDocument38 pagesSurgical NCP DRUG STUDY PATHOPHYSIOLOGYBrandy Jaffar100% (1)
- Nursing Care Plan 1Document2 pagesNursing Care Plan 1Denise GabatoNo ratings yet
- Assignment in NCM 106 LectureDocument6 pagesAssignment in NCM 106 LectureJeanessa Delantar QuilisadioNo ratings yet
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- Gonzaga Rlems - NCPDocument3 pagesGonzaga Rlems - NCPShaynne Wencille A. GONZAGANo ratings yet
- NCP PediatricDocument5 pagesNCP PediatricSL Hanna NebridaNo ratings yet
- Prioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument5 pagesPrioritization of Problems Rank Problem Identified: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesTom CuencaNo ratings yet
- That Will Affect The Choice of Teaching Strategy or ApproachDocument2 pagesThat Will Affect The Choice of Teaching Strategy or ApproachDagmawit GirmaNo ratings yet
- Enema-Check-List RationaleDocument5 pagesEnema-Check-List Rationaleamal abdulrahmanNo ratings yet
- Alteration of The Starling Forces Which Control Transfer of Fluid From The Vascular Compartment To Surrounding Tissue SpacesDocument3 pagesAlteration of The Starling Forces Which Control Transfer of Fluid From The Vascular Compartment To Surrounding Tissue SpacesNicole cuencosNo ratings yet
- N039-N040 Rejano Nursing Care PlanDocument3 pagesN039-N040 Rejano Nursing Care PlanBianca Marithè RejanoNo ratings yet
- NCP Urinary RetentionDocument3 pagesNCP Urinary RetentionKingJayson Pacman06No ratings yet
- Pedia NCPDocument6 pagesPedia NCPZel MartinezNo ratings yet
- NCP Deficient Fluid VolumeDocument3 pagesNCP Deficient Fluid VolumeDoneva Lyn MedinaNo ratings yet
- Diarrhea Nursing Care PlanDocument2 pagesDiarrhea Nursing Care PlanKrizha Angela NicolasNo ratings yet
- Impaired Urinary EliminationDocument2 pagesImpaired Urinary EliminationMatty-b AskalaniNo ratings yet
- For Printing Jan23Document3 pagesFor Printing Jan23Jhoan OllanoNo ratings yet
- NCP For UTIDocument3 pagesNCP For UTIlachrymoseai100% (4)
- NCP Acabo Hypokalemia 1Document2 pagesNCP Acabo Hypokalemia 1Doneva Lyn MedinaNo ratings yet
- DiarrheaDocument3 pagesDiarrheaBert GasalNo ratings yet
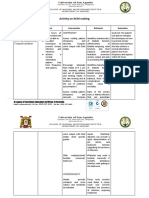
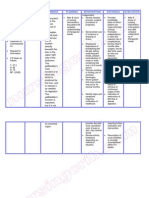
- Activity On NCM MakingDocument4 pagesActivity On NCM MakingJollan Marie BuenvenidaNo ratings yet
- Geriatric Nursing: Ma - Alicia Grace S. Kaimo, RN, ManDocument17 pagesGeriatric Nursing: Ma - Alicia Grace S. Kaimo, RN, ManYongNo ratings yet
- NCP CSDocument9 pagesNCP CSFreida Marie PiczonNo ratings yet
- Urinary Catherization: St. Paul University Dumaguete College of Nursing Dumaguete City First Semester, 2021-2022Document9 pagesUrinary Catherization: St. Paul University Dumaguete College of Nursing Dumaguete City First Semester, 2021-2022Franz goNo ratings yet
- Nursing Care PlansDocument4 pagesNursing Care PlansanreilegardeNo ratings yet
- Nursing Care PlansDocument4 pagesNursing Care Planswerismy daddyNo ratings yet
- NCPDocument6 pagesNCPJoni Lyn Ba-as BayengNo ratings yet
- NCP - Impaired Urinary EliminationDocument3 pagesNCP - Impaired Urinary EliminationFretzgine Lou ManuelNo ratings yet
- Related Learning Experience Fundamentals in Nursing 4 RotationDocument3 pagesRelated Learning Experience Fundamentals in Nursing 4 RotationMark Eliezer CulasingNo ratings yet
- Nursing Diagnoses Adult HealthDocument8 pagesNursing Diagnoses Adult HealthyormahdNo ratings yet
- Nursing Care Plan: RationaleDocument5 pagesNursing Care Plan: Rationalerona-chanNo ratings yet
- Risk For Fluid VolumeDocument1 pageRisk For Fluid VolumeMariella BadongenNo ratings yet
- Nursing Care Plan Cholecystectomy Gall Bladder RemovalDocument2 pagesNursing Care Plan Cholecystectomy Gall Bladder Removalderic100% (16)
- CAUTI Bundle of Care PDFDocument3 pagesCAUTI Bundle of Care PDFArvie PavinoNo ratings yet
- Nursing-Care-Plan - AgeDocument7 pagesNursing-Care-Plan - AgePanda JocyNo ratings yet
- Rules and Directions for the Employment of Injections in Various DiseasesFrom EverandRules and Directions for the Employment of Injections in Various DiseasesNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- Gastric Sleeve Diet: Step By Step Guide For Planning What to Do and Eat Before and After Your SurgeryFrom EverandGastric Sleeve Diet: Step By Step Guide For Planning What to Do and Eat Before and After Your SurgeryNo ratings yet
- Encopresis, (Fecal Incontinence) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEncopresis, (Fecal Incontinence) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Assessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentDocument7 pagesAssessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentQueenie Silva100% (1)
- Community Health Nursing: Family Assessment Guide FormDocument6 pagesCommunity Health Nursing: Family Assessment Guide FormQueenie SilvaNo ratings yet
- Feliciano, Troy Ivan Silva, Queenie Rose V. BSN 3-C: Rationale: To Track The Changes of Client's ConditionDocument4 pagesFeliciano, Troy Ivan Silva, Queenie Rose V. BSN 3-C: Rationale: To Track The Changes of Client's ConditionQueenie SilvaNo ratings yet
- Subjective Data: Short Term Independent: College of NursingDocument8 pagesSubjective Data: Short Term Independent: College of NursingQueenie SilvaNo ratings yet
- Drug Study - Osteomyelitis - Dalangin Delos Santos Pajarillo RigatDocument6 pagesDrug Study - Osteomyelitis - Dalangin Delos Santos Pajarillo RigatQueenie SilvaNo ratings yet
- Alzheimers FinalsDocument82 pagesAlzheimers FinalsQueenie SilvaNo ratings yet
- Effective Nursing Leadership and Management: How To Be An Effective Nursing LeaderDocument60 pagesEffective Nursing Leadership and Management: How To Be An Effective Nursing LeaderQueenie SilvaNo ratings yet
- Historical Development of TheoriesDocument5 pagesHistorical Development of TheoriesMichael100% (3)
- In Patient Satisfaction Survey-How Does It Help Our Health Care Delivery System (The Patient, The Health Care Giver and The Organization) ?Document10 pagesIn Patient Satisfaction Survey-How Does It Help Our Health Care Delivery System (The Patient, The Health Care Giver and The Organization) ?Pallavi PalluNo ratings yet
- Febuxostat Mylan Epar Public Assessment Report - enDocument28 pagesFebuxostat Mylan Epar Public Assessment Report - entomas.palominosNo ratings yet
- CPHRM Legal and Regulatory Version 2Document147 pagesCPHRM Legal and Regulatory Version 2Hosam GomaaNo ratings yet
- NEJM ResponseDocument2 pagesNEJM Responseamit545No ratings yet
- Past, Present, and Future of Antibacterial Economics: Increasing Bacterial Resistance, Limited Antibiotic Pipeline, and Societal ImplicationsDocument14 pagesPast, Present, and Future of Antibacterial Economics: Increasing Bacterial Resistance, Limited Antibiotic Pipeline, and Societal ImplicationsLeonardo SimonciniNo ratings yet
- Elevator Utilization and Emergency ProceduresDocument3 pagesElevator Utilization and Emergency ProceduresBudi YunantoNo ratings yet
- Narrative Report. Ate DaleDocument2 pagesNarrative Report. Ate DaleKryza Dale Bunado Batican89% (9)
- Analysis of Fortis HealthcareDocument40 pagesAnalysis of Fortis HealthcareAniket KhorgadeNo ratings yet
- Neurologist Deborah Boland, D.O., MSPT, Named "Physician of The Year"Document3 pagesNeurologist Deborah Boland, D.O., MSPT, Named "Physician of The Year"PR.comNo ratings yet
- CMHNDocument48 pagesCMHNvikaNo ratings yet
- Chapter 11 Power Point (1) - 5 PDFDocument25 pagesChapter 11 Power Point (1) - 5 PDFMuhammad NaveedNo ratings yet
- Câu Hỏi Ôn Tập: (Các lớp Cao đẳng Dược)Document12 pagesCâu Hỏi Ôn Tập: (Các lớp Cao đẳng Dược)Di ThiênNo ratings yet
- ICM Essential Competencies For Basic Midwifery Practice 2010, Revised 2013 PDFDocument19 pagesICM Essential Competencies For Basic Midwifery Practice 2010, Revised 2013 PDFKuurniiaa PraweestiiNo ratings yet
- Infra Red vs. Sitz BathDocument7 pagesInfra Red vs. Sitz BathMikeNo ratings yet
- First Step To Achieve Your Objective - GomezDocument8 pagesFirst Step To Achieve Your Objective - GomezNicole Ivy GorimoNo ratings yet
- Daftar Pustaka ManajemenDocument2 pagesDaftar Pustaka ManajemenAnip WungkulNo ratings yet
- Health Care Delivery System in IndiaDocument63 pagesHealth Care Delivery System in IndiaamsabavanNo ratings yet
- SLT Ca Ts TC ExDocument1 pageSLT Ca Ts TC ExMahmoud AtefNo ratings yet
- Leadership and ManagementDocument70 pagesLeadership and ManagementElaisa Mae Delos Santos100% (3)
- Effectiveness of Varmam and Thokkanam THDocument5 pagesEffectiveness of Varmam and Thokkanam THTam gdzie nauka spotyka się z magiąNo ratings yet
- Sample Complaints LettersDocument4 pagesSample Complaints LettersZdenka PetroskyNo ratings yet
- My Visa Cover Letter 1Document5 pagesMy Visa Cover Letter 1Tehami JawedNo ratings yet
- Guidelines For Management of Under-Five Children Brought in Dead (BID) To Ministry of Health FacilitiesDocument68 pagesGuidelines For Management of Under-Five Children Brought in Dead (BID) To Ministry of Health FacilitiesNORFARIZA BINTI MOHAMAD YUSOF (PKDMANJUNG)No ratings yet
- My Goals EssayyDocument2 pagesMy Goals Essayyapi-532076052No ratings yet
- Moderna CEO Stephane Bancel Says Coronavirus Vaccine Price Will Be LowDocument3 pagesModerna CEO Stephane Bancel Says Coronavirus Vaccine Price Will Be Lowtp4oyk fdtaz4100% (1)
- PDF Midwifery Final Test 1Document7 pagesPDF Midwifery Final Test 1DianeNo ratings yet
- Oamjms 7 482 PDFDocument13 pagesOamjms 7 482 PDFfaishal azharNo ratings yet