Download as pdf or txt
You might also like
- PDF The Ophthalmic Assistant A Text For Allied and Associated Ophthalmic Personnel 10Th Ed 10Th Edition Harold A Stein Ebook Full ChapterDocument54 pagesPDF The Ophthalmic Assistant A Text For Allied and Associated Ophthalmic Personnel 10Th Ed 10Th Edition Harold A Stein Ebook Full Chaptermichael.routzahn408100% (2)
- Denas ManualDocument78 pagesDenas Manualgetdenas100% (14)
- The Wills Eye Manual, 5th Ed.-2008 (Masternikos)Document2 pagesThe Wills Eye Manual, 5th Ed.-2008 (Masternikos)Ioana Vev0% (1)
- Olav Istre (Eds.) - Minimally Invasive Gynecological Surgery-Springer-Verlag Berlin Heidelberg (2015)Document201 pagesOlav Istre (Eds.) - Minimally Invasive Gynecological Surgery-Springer-Verlag Berlin Heidelberg (2015)ravikanth100% (1)
- CT ProtocolsDocument263 pagesCT ProtocolsMihir Katlariwala100% (3)
- Ewquickguide 2 EdDocument188 pagesEwquickguide 2 EdStanley Wu TaiNo ratings yet
- Evarrest MonographDocument24 pagesEvarrest MonographbasakerpolatNo ratings yet
- Addressing The Gaps: The Philippines As An Emerging Health Tourism DestinationDocument9 pagesAddressing The Gaps: The Philippines As An Emerging Health Tourism DestinationN.a. M. TandayagNo ratings yet
- Laparoscopic Liver ResectionDocument111 pagesLaparoscopic Liver ResectionTeodora-Valeria Tolan100% (1)
- 5 Axillary and Epitrochlear Lymph Node Dissection For MelanomaDocument11 pages5 Axillary and Epitrochlear Lymph Node Dissection For MelanomajuanrangoneNo ratings yet
- MelanomaDocument53 pagesMelanomaJaime Montenegro CnNo ratings yet
- Chang-Ming Huang, Chao-Hui Zheng (Eds.) - Laparoscopic Gastrectomy For Gastric Cancer - Surgical Technique and Lymphadenectomy-Springer Netherlands (2015)Document357 pagesChang-Ming Huang, Chao-Hui Zheng (Eds.) - Laparoscopic Gastrectomy For Gastric Cancer - Surgical Technique and Lymphadenectomy-Springer Netherlands (2015)Jaldo Freire100% (1)
- Aricol Cancer PancreaticDocument10 pagesAricol Cancer PancreaticBuliga ClaudiaNo ratings yet
- Vascular and Interventional Radiology Principles and Practice 2002Document497 pagesVascular and Interventional Radiology Principles and Practice 2002Felipe Negrao100% (1)
- Chest Drain GuidelineDocument42 pagesChest Drain GuidelineBảo TrungNo ratings yet
- W2018 MinorSurgeryManualDocument99 pagesW2018 MinorSurgeryManualLaetitia RobyNo ratings yet
- Stine Helene Falsig Pedersen (Editor) - Reviews of Physiology, Biochemistry and Pharmacology. 177-Springer (2021)Document155 pagesStine Helene Falsig Pedersen (Editor) - Reviews of Physiology, Biochemistry and Pharmacology. 177-Springer (2021)shuvvro dhaNo ratings yet
- Metastases Detection in Lymph Nodes Using Transfer Learning: Michel KokDocument41 pagesMetastases Detection in Lymph Nodes Using Transfer Learning: Michel KokShahid Akram MohammadNo ratings yet
- Seminars in Cell & Developmental Biology: Shan Liao, P.Y. Von Der WeidDocument7 pagesSeminars in Cell & Developmental Biology: Shan Liao, P.Y. Von Der WeidItzelArteagaNo ratings yet
- 1 5053054235202027721Document175 pages1 5053054235202027721andifa aziz satriawanNo ratings yet
- ''Sangrado Perioperatorio Severo GuiaDocument113 pages''Sangrado Perioperatorio Severo GuiaHECTOR ESTRADANo ratings yet
- Anaesthesia For Cataract SurgeryDocument19 pagesAnaesthesia For Cataract SurgeryRido Banar EkaputraNo ratings yet
- Ebook Complications During and After Cataract Surgery From Phacoemulsification Over Secondary Iol Implantation To Dropped Nucleus Ulrich Spandau Gabor B Scharioth Online PDF All ChapterDocument70 pagesEbook Complications During and After Cataract Surgery From Phacoemulsification Over Secondary Iol Implantation To Dropped Nucleus Ulrich Spandau Gabor B Scharioth Online PDF All Chapterkirk.chappell316100% (11)
- Article in Press: Acquired C1-Inhibitor Deficiency and Lymphoproliferative Disorders: A Tight RelationshipDocument10 pagesArticle in Press: Acquired C1-Inhibitor Deficiency and Lymphoproliferative Disorders: A Tight Relationshipapi-239502672No ratings yet
- Ultrasonography Upper-Extremity 082228Document119 pagesUltrasonography Upper-Extremity 082228Pamela Cielo BalboaNo ratings yet
- Edwards Critical Care Quick Guide To Cardiopulmonary Care PDFDocument188 pagesEdwards Critical Care Quick Guide To Cardiopulmonary Care PDFanonNo ratings yet
- Quick Guide To Cardiopulmonary CareDocument188 pagesQuick Guide To Cardiopulmonary CareAlex ApsokardosNo ratings yet
- Bellmunt Montoya2012Document11 pagesBellmunt Montoya2012vic alNo ratings yet
- Medial Collateral Ligament in The Multiligament Knee InjuryDocument12 pagesMedial Collateral Ligament in The Multiligament Knee InjuryMariana V. RendónNo ratings yet
- Atlas of Full Breast Ultrasonography 1st Edition PDFDocument392 pagesAtlas of Full Breast Ultrasonography 1st Edition PDFlllorelllei100% (2)
- 2735 Pediatric Cataract Manual - CompressedDocument66 pages2735 Pediatric Cataract Manual - CompressedKevin RamsahaiNo ratings yet
- Paraboschi2020 2Document8 pagesParaboschi2020 2nugra raturandangNo ratings yet
- ESVS Thoracic Ds PDFDocument49 pagesESVS Thoracic Ds PDFFredy CarolNo ratings yet
- Spectrometrie de MasaDocument13 pagesSpectrometrie de MasaLara LarukNo ratings yet
- Progress in Retinal and Eye ResearchDocument35 pagesProgress in Retinal and Eye ResearchYegor KharkovNo ratings yet
- Current Developments in Glaucoma Surgery and MigsDocument327 pagesCurrent Developments in Glaucoma Surgery and MigsFelipe AlarconNo ratings yet
- Manual For EndosDocument19 pagesManual For EndosVarsha MalikNo ratings yet
- Clay 2013Document9 pagesClay 2013Corina Scerbatiuc-CondurNo ratings yet
- Textbook Atlas of Neurotologic and Lateral Skull Base Surgery 1St Edition John S Oghalai Ebook All Chapter PDFDocument53 pagesTextbook Atlas of Neurotologic and Lateral Skull Base Surgery 1St Edition John S Oghalai Ebook All Chapter PDFdiana.hightower624100% (20)
- Transplant and Dialysis Handbook 2nd Edition January 2017Document125 pagesTransplant and Dialysis Handbook 2nd Edition January 2017nathanielNo ratings yet
- Wen Et Al 2019 Echinococcosis Advances in The 21st CenturyDocument39 pagesWen Et Al 2019 Echinococcosis Advances in The 21st CenturyguidahiNo ratings yet
- 01499-2021 FullDocument81 pages01499-2021 FullBrendaNo ratings yet
- Seminars in Cell & Developmental BiologyDocument14 pagesSeminars in Cell & Developmental BiologyGlauce L TrevisanNo ratings yet
- Islam Et Al. - 2015 - Cancer Stem Cells in Oesophageal Squamous Cell Carcinoma Identification, Prognostic and Treatment PerspectivesDocument11 pagesIslam Et Al. - 2015 - Cancer Stem Cells in Oesophageal Squamous Cell Carcinoma Identification, Prognostic and Treatment PerspectivesCarly LeungNo ratings yet
- ICRP Pub116Document257 pagesICRP Pub116chibagoNo ratings yet
- Early Versus Delayed Post-Operative Bathing or Showering To Prevent Wound ComplicationsDocument25 pagesEarly Versus Delayed Post-Operative Bathing or Showering To Prevent Wound ComplicationsagusNo ratings yet
- Abscesos Drenaje y Fistula CochraneDocument17 pagesAbscesos Drenaje y Fistula CochraneAgustina ZabiniNo ratings yet
- Atlas of Skin Cancers-Practical Guide To Diagnosis - XXXDocument138 pagesAtlas of Skin Cancers-Practical Guide To Diagnosis - XXXHossam Thabet100% (4)
- Aapm Report 17 Tg29 TbiDocument60 pagesAapm Report 17 Tg29 TbithewholekiboshNo ratings yet
- Vascular Surgery Notes: DR H LouwrensDocument41 pagesVascular Surgery Notes: DR H LouwrensbiancaNo ratings yet
- Corneal Colagen PDFDocument185 pagesCorneal Colagen PDFreza arlasNo ratings yet
- Chest Drain Insertion and Management UHL Childrens Hospital GuidelineDocument21 pagesChest Drain Insertion and Management UHL Childrens Hospital Guidelinehungnguyenmanh2012No ratings yet
- Delineating Organs at Risk in RadiationDocument9 pagesDelineating Organs at Risk in Radiationk3 GiaobanNo ratings yet
- Complete Mesocolic Excision and Central Vascular Ligation For Colon CancerDocument11 pagesComplete Mesocolic Excision and Central Vascular Ligation For Colon CancerMassimiliano CasadeiNo ratings yet
- 2019 ELSO Meeting Abstracts.1Document109 pages2019 ELSO Meeting Abstracts.1Luis Rubén MirandaNo ratings yet
- OAR BookDocument156 pagesOAR BookonlinebookkNo ratings yet
- TH2016PESC1021 ConvertieDocument209 pagesTH2016PESC1021 ConvertieKaviraj SenguntharNo ratings yet
- Rizzieri 2016Document13 pagesRizzieri 2016alinamatei1000000No ratings yet
- Cochrane Systematic ReviewDocument29 pagesCochrane Systematic ReviewSantiago Sandoval JiménezNo ratings yet
- Medical treatment and operative repair of abdominal aortic aneurysmsFrom EverandMedical treatment and operative repair of abdominal aortic aneurysmsNo ratings yet
- Parotidectomia - UpToDate 2022Document2 pagesParotidectomia - UpToDate 2022juanrangoneNo ratings yet
- Glandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.Document2 pagesGlandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.juanrangoneNo ratings yet
- Parathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022Document42 pagesParathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Intraoperative Parathyroid Hormone Assays - Uptodate 2022Document18 pagesIntraoperative Parathyroid Hormone Assays - Uptodate 2022juanrangoneNo ratings yet
- Parathyroid Surgery For Inherited Syndromes - Uptodate 2022Document25 pagesParathyroid Surgery For Inherited Syndromes - Uptodate 2022juanrangoneNo ratings yet
- Parathyroidectomy in End-Stage Kidney Disease - Uptodate 2022Document27 pagesParathyroidectomy in End-Stage Kidney Disease - Uptodate 2022juanrangoneNo ratings yet
- Preoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022Document22 pagesPreoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Niveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesDocument1 pageNiveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesjuanrangoneNo ratings yet
- Surgical Anatomy of The Parathyroid Glands - Uptodate 2022Document8 pagesSurgical Anatomy of The Parathyroid Glands - Uptodate 2022juanrangoneNo ratings yet
- Vandeventer 2016Document10 pagesVandeventer 2016juanrangoneNo ratings yet
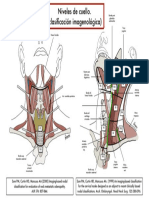
- Clasif Imagenológica Niveles de CuelloDocument1 pageClasif Imagenológica Niveles de CuellojuanrangoneNo ratings yet
- 5 Axillary and Epitrochlear Lymph Node Dissection For MelanomaDocument11 pages5 Axillary and Epitrochlear Lymph Node Dissection For MelanomajuanrangoneNo ratings yet
- The Attachments of The Breast To The Chest Wall: A Dissection StudyDocument12 pagesThe Attachments of The Breast To The Chest Wall: A Dissection StudyjuanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document5 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangoneNo ratings yet
- I HFGDocument31 pagesI HFGmarcelo.lacknerNo ratings yet
- Available BoneDocument46 pagesAvailable BoneAkanksha MahajanNo ratings yet
- Chir Eng 07 Surgical Knots and SuturesDocument20 pagesChir Eng 07 Surgical Knots and SuturesAndrei BarbuNo ratings yet
- Appendicitis Concept MapDocument1 pageAppendicitis Concept MapIris MambuayNo ratings yet
- Does The Artery-First Approach Improve The Rate of R0 Resection in Pancreatoduodenectomy?Document9 pagesDoes The Artery-First Approach Improve The Rate of R0 Resection in Pancreatoduodenectomy?vmdcabanillaNo ratings yet
- Cover LetterDocument1 pageCover Letterm1.nourianNo ratings yet
- Case Study 39-Year-Old Women Diagnosed As Solitary Rectal Ulcer SyndromeDocument5 pagesCase Study 39-Year-Old Women Diagnosed As Solitary Rectal Ulcer SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- TourniquetTouch 1.0 EN 07.18Document11 pagesTourniquetTouch 1.0 EN 07.18Shaikh Emran HossainNo ratings yet
- Course Title: Surgery Tecniques - I & Clinical PracticeDocument4 pagesCourse Title: Surgery Tecniques - I & Clinical PracticeZia KhanNo ratings yet
- Chapter 1 - Coronary WiresDocument9 pagesChapter 1 - Coronary WiresRakesh DashNo ratings yet
- Kathy Huckeba InterviewDocument10 pagesKathy Huckeba Interviewapi-420635428No ratings yet
- Dr. Shazima Ali: ObjectiveDocument3 pagesDr. Shazima Ali: ObjectiveShery ChuhanNo ratings yet
- Network Hospital Grading Proforma: General InformationDocument6 pagesNetwork Hospital Grading Proforma: General InformationSanket SahareNo ratings yet
- CathSap BDocument153 pagesCathSap BSajjad HussainNo ratings yet
- 01 - Hair RemovalDocument2 pages01 - Hair Removalbagus lazuardiNo ratings yet
- Amyand's Hernia: An Up-to-Date Review of The Literature: Dimitrios Patoulias, Maria Kalogirou, Ioannis PatouliasDocument4 pagesAmyand's Hernia: An Up-to-Date Review of The Literature: Dimitrios Patoulias, Maria Kalogirou, Ioannis Patouliasϟ Orbi SinkaNo ratings yet
- A Clinical Sign of Canal ParesisDocument3 pagesA Clinical Sign of Canal ParesisMadelinePérezNo ratings yet
- Wound DehiscenceDocument15 pagesWound DehiscenceManar AlhakamiNo ratings yet
- Interventional Approaches Gallbladder DiseaseDocument9 pagesInterventional Approaches Gallbladder DiseaseAntônio GoulartNo ratings yet
- Pathophysiology of Congestive Heart Failure: Reported By: Jay - Ann M. Cabia BSN II-ADocument21 pagesPathophysiology of Congestive Heart Failure: Reported By: Jay - Ann M. Cabia BSN II-Ajoyrena ochondraNo ratings yet
- Langer1985 Sub Epithelial Connective Tissue GraftDocument6 pagesLanger1985 Sub Epithelial Connective Tissue GraftAna Maria Montoya GomezNo ratings yet
- Pneumoclear IFUDocument77 pagesPneumoclear IFUputraNo ratings yet
- Alfred Hosp ICU-orientation-manualDocument85 pagesAlfred Hosp ICU-orientation-manualdragon66No ratings yet
- Daffa Gemineo Dheona - 31102000017 - Literature ReviewDocument2 pagesDaffa Gemineo Dheona - 31102000017 - Literature ReviewRahmadhani AtmiantoNo ratings yet
- General Surgery Applicant Guide 2023Document16 pagesGeneral Surgery Applicant Guide 2023laithNo ratings yet
- Brain MethsDocument17 pagesBrain MethsBolinho ChuvaNo ratings yet
- Sydney Cherry Knee Replacement TransferDocument3 pagesSydney Cherry Knee Replacement TransferM. GNo ratings yet