Download as docx, pdf, or txt
You might also like
- Level 7 Passage 2Document5 pagesLevel 7 Passage 2WaleedNo ratings yet
- Ldm2 Lac04 Pagaduan, Kimberly RoseDocument19 pagesLdm2 Lac04 Pagaduan, Kimberly Roseseniorhighschool talugtugnhsNo ratings yet
- Consultation Handbook - Bill BevingtonDocument37 pagesConsultation Handbook - Bill BevingtonAnny Aun50% (2)
- ICN Code of Ethics For NursesDocument4 pagesICN Code of Ethics For NursesSj Eclipse100% (1)
- Cot 1 - DLPDocument5 pagesCot 1 - DLPJhay R Quito0% (1)
- HG Grade 10 Module 2Document27 pagesHG Grade 10 Module 2wendell john medianaNo ratings yet
- Filipino 10 CMDocument32 pagesFilipino 10 CMCloue Faye I. Basallo100% (1)
- Clamohoy 1ng10 WHLP q2 - 2020-2021Document12 pagesClamohoy 1ng10 WHLP q2 - 2020-2021michaelNo ratings yet
- 3F Detailed Information On Fire Code Fees Collection by The BFP and LGU For FY Rev00 062118Document2 pages3F Detailed Information On Fire Code Fees Collection by The BFP and LGU For FY Rev00 062118Pascua JarisonNo ratings yet
- Mid Year Review Form 2023 2024 Fil Dept.Document8 pagesMid Year Review Form 2023 2024 Fil Dept.Mar Janeh LouNo ratings yet
- Filipino 7 q3 Las 3 Week 2 Melc 3 2Document6 pagesFilipino 7 q3 Las 3 Week 2 Melc 3 2Charmaine ChienNo ratings yet
- KT. RebongDocument91 pagesKT. RebongJayl Catanjal JuecoNo ratings yet
- Curriculum Map Grade 7 A FilipinoDocument5 pagesCurriculum Map Grade 7 A FilipinoRasec Nayr CoseNo ratings yet
- University of Caloocan City Camarin Campus Graduate School MAED 305Document2 pagesUniversity of Caloocan City Camarin Campus Graduate School MAED 305Silvester CardinesNo ratings yet
- Res Cip ReadingDocument26 pagesRes Cip ReadingMichelle Loben MercadoNo ratings yet
- Tip Course 6 With Answers PDFDocument95 pagesTip Course 6 With Answers PDFAngie Joey AbbottNo ratings yet
- Table of Specification: Republic of The Philippines CARAGA Administrative Region Numancia East DistrictDocument4 pagesTable of Specification: Republic of The Philippines CARAGA Administrative Region Numancia East DistrictArielyn Pame SulapasNo ratings yet
- Course Code FIL Course Title Related Course Titles Pre-Requisite Pre - Requisite To: None Credit 3 Class Hours 3 Lab Hours 0 Course DescriptionDocument19 pagesCourse Code FIL Course Title Related Course Titles Pre-Requisite Pre - Requisite To: None Credit 3 Class Hours 3 Lab Hours 0 Course DescriptionNHOJ SILENCERNo ratings yet
- Brigada NarrativeDocument11 pagesBrigada NarrativeYen Adams Oliverio AlemanNo ratings yet
- Rojo, Christian: Filipino 10 Unang Markaha N Modyul 1Document3 pagesRojo, Christian: Filipino 10 Unang Markaha N Modyul 1Alfie CagampangNo ratings yet
- Deped Form 138-E Division of Iligan City - (User-Editable Entry)Document6 pagesDeped Form 138-E Division of Iligan City - (User-Editable Entry)Von Tatil100% (1)
- 3rd Quarter Tos NewDocument9 pages3rd Quarter Tos NewHANNA GALENo ratings yet
- Filamer Christian University Roxas City Graduate SchoolDocument21 pagesFilamer Christian University Roxas City Graduate SchoolRuth del RosarioNo ratings yet
- Teachers Manual in Filipino 10 PDFDocument2 pagesTeachers Manual in Filipino 10 PDFEdilyn HinotanNo ratings yet
- Fil7 Q4 M8-Final-okDocument16 pagesFil7 Q4 M8-Final-okJOHN JOHNNo ratings yet
- MELC and BOW Q3Document69 pagesMELC and BOW Q3Maria Carmela Rachel GazilNo ratings yet
- ENGLISHDocument81 pagesENGLISHMARIETTA DIANo ratings yet
- Quarter 4 Week 2Document14 pagesQuarter 4 Week 2BENELYN C. CINCONo ratings yet
- Division of Lanao Del Norte Calube Integrated School: Filipino 7 Table of SpecificationsDocument4 pagesDivision of Lanao Del Norte Calube Integrated School: Filipino 7 Table of SpecificationsCharity Anne Camille PenalozaNo ratings yet
- Acr - Brigada Eskwela 2020Document4 pagesAcr - Brigada Eskwela 2020ELYNILYN BANTILANNo ratings yet
- Certificates of RecognitionDocument3 pagesCertificates of RecognitionFlordiles Navarro100% (1)
- Effects of The Simplified PVC Reading Approach Through The Implementation of The 'Basa Baya Lahat' Program To The Reading Skills Development of The Struggling ReadersDocument18 pagesEffects of The Simplified PVC Reading Approach Through The Implementation of The 'Basa Baya Lahat' Program To The Reading Skills Development of The Struggling ReadersPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Certificate of Regognition For Honor Students 2022Document8 pagesCertificate of Regognition For Honor Students 2022Ronna Jean SambitanNo ratings yet
- DM Phrod 2021 0590 Balik Probinsya Bagong Pag Asa BP2 BeneficiariesDocument1 pageDM Phrod 2021 0590 Balik Probinsya Bagong Pag Asa BP2 BeneficiariesannabelleNo ratings yet
- Request SlipDocument1 pageRequest SlipKhymberly Whey MercadoNo ratings yet
- Best Practices in Teaching English 5Document5 pagesBest Practices in Teaching English 5John SolivenNo ratings yet
- Grade Level No. of Pupils Non-Reader Frustration Instructional IndependentDocument2 pagesGrade Level No. of Pupils Non-Reader Frustration Instructional IndependentIrene May Legaspi PalisocNo ratings yet
- Letter LISDocument2 pagesLetter LISPunong Grande NhsNo ratings yet
- DLL Q3W5 Grade10Document11 pagesDLL Q3W5 Grade10MAY DE LA CRUZNo ratings yet
- Narrative Portfolio Gragraduate NaDocument67 pagesNarrative Portfolio Gragraduate NaSantos S Armie LizaNo ratings yet
- ACR Card Day-Distribution of Donated Books-Notebooks06Document1 pageACR Card Day-Distribution of Donated Books-Notebooks06laarniNo ratings yet
- Letter of ConsentDocument1 pageLetter of ConsentElsie Joy D. LicarteNo ratings yet
- Radio-Script - Noting Context Clues - ENGLISHDocument12 pagesRadio-Script - Noting Context Clues - ENGLISHXieanne Soriano RamosNo ratings yet
- Excellent Achievers Learning, Center, IncDocument5 pagesExcellent Achievers Learning, Center, IncJoyR.Alota100% (1)
- 2019 Filgr7q3Document122 pages2019 Filgr7q3Jenalyn TayamNo ratings yet
- Evaluative Statements Assertion: SLK 4 For Reading and Writing Skills For Grade 11 Quarter 4 Week 3-4Document12 pagesEvaluative Statements Assertion: SLK 4 For Reading and Writing Skills For Grade 11 Quarter 4 Week 3-4Heinrich OmerezNo ratings yet
- 2022 NEAP CV For Resource Speakers Gen OardeDocument3 pages2022 NEAP CV For Resource Speakers Gen OardeSVPSNo ratings yet
- SF 9Document3 pagesSF 9Effer Agbay AceNo ratings yet
- Slogan Making Contest CriteriaDocument2 pagesSlogan Making Contest CriteriaWynnebel AnacioNo ratings yet
- Masterlist of Private Elem. Schools S.Y. 2016 2017 Batangas CityDocument6 pagesMasterlist of Private Elem. Schools S.Y. 2016 2017 Batangas CityJaimelyn ManguerraNo ratings yet
- Award Certificates (Elegant)Document4 pagesAward Certificates (Elegant)joyceNo ratings yet
- Catch-Up-Fridays-Teaching-Guide-Filipino 7 FinalDocument5 pagesCatch-Up-Fridays-Teaching-Guide-Filipino 7 FinalDonna Lou Dela CruzNo ratings yet
- Homeroom Guidance Learner's Development Assessment (JHS)Document2 pagesHomeroom Guidance Learner's Development Assessment (JHS)Kent DaradarNo ratings yet
- AR-mam Rowena 2019Document19 pagesAR-mam Rowena 2019San Quintin Central SchoolNo ratings yet
- Maed 202Document2 pagesMaed 202Maan AnonuevoNo ratings yet
- Scout Project Work Plan and Budget Matrix 1Document2 pagesScout Project Work Plan and Budget Matrix 1Romnick PadolinaNo ratings yet
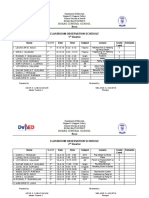
- Roxas Central School: Classroom Observation Schedule 1 QuarterDocument5 pagesRoxas Central School: Classroom Observation Schedule 1 QuarterMarj Reña LunaNo ratings yet
- 50 Beautiful Places To Visit in KoreaDocument51 pages50 Beautiful Places To Visit in KoreaElla MaglunobNo ratings yet
- Leadership & Management in The Different Arts & Fields - GRADE 12Document8 pagesLeadership & Management in The Different Arts & Fields - GRADE 12Jessiah Jade LeyvaNo ratings yet
- Certificate of Appreciation: Mat-I (Naawan) National High SchoolDocument1 pageCertificate of Appreciation: Mat-I (Naawan) National High Schooldolly kate cagadasNo ratings yet
- Narrative Report On Brigada Pagbasa CulminationDocument2 pagesNarrative Report On Brigada Pagbasa Culminationmary ann de leonNo ratings yet
- EC Medical Reimbursement Application Form 1Document2 pagesEC Medical Reimbursement Application Form 1GaryNo ratings yet
- Sonnykalangi,+13 +ok+ (13) +sudarman+68-80Document21 pagesSonnykalangi,+13 +ok+ (13) +sudarman+68-80Nandini Permata SariNo ratings yet
- Hailey Gilbreath Resume 07-23-2020Document1 pageHailey Gilbreath Resume 07-23-2020api-534716659No ratings yet
- Innovative Use of Technology in BABINA DiagnosticsDocument9 pagesInnovative Use of Technology in BABINA DiagnosticsSukumar ThingomNo ratings yet
- TTFPP Questionnaires - by D.C-1-1Document3 pagesTTFPP Questionnaires - by D.C-1-1Kofi AsaaseNo ratings yet
- First AidDocument10 pagesFirst AidArslan Shaukat100% (1)
- Sample Complaints LettersDocument4 pagesSample Complaints LettersZdenka PetroskyNo ratings yet
- Application Form For Punjab Residency Program (Level - Iv) TrainingDocument6 pagesApplication Form For Punjab Residency Program (Level - Iv) TrainingFatima Habib JajjaNo ratings yet
- NSCMP - Claim FormDocument6 pagesNSCMP - Claim FormArun Prabhakaran PNo ratings yet
- DYDRNHS Learners Vax. Status TemplateDocument3 pagesDYDRNHS Learners Vax. Status TemplateCristinaNo ratings yet
- Protocolo de EscritaDocument5 pagesProtocolo de EscritaGabriela Ruggiero NorNo ratings yet
- Reduced Hospital Revenue Due To Error Code Diagnosis in The Implementation of INA-CBGsDocument7 pagesReduced Hospital Revenue Due To Error Code Diagnosis in The Implementation of INA-CBGsIJPHSNo ratings yet
- Psoriasis Biologics RegistryDocument6 pagesPsoriasis Biologics RegistryWei Sheng ChongNo ratings yet
- Civil Hospital Visit Report: TH NDDocument5 pagesCivil Hospital Visit Report: TH NDPranita DisaleNo ratings yet
- Treatment of An Ankylosed Central Incisor by Single Tooth Dento-Osseous Osteotomy and A Simple Distraction DeviceDocument9 pagesTreatment of An Ankylosed Central Incisor by Single Tooth Dento-Osseous Osteotomy and A Simple Distraction DeviceJuan Carlos MeloNo ratings yet
- Trends in Pharmaceutical IndustryDocument20 pagesTrends in Pharmaceutical IndustryAbdelhamidgmNo ratings yet
- PainDocument35 pagesPainixora n100% (1)
- MsacsadpDocument3 pagesMsacsadpJeshiNo ratings yet
- Ed Staff Meeting MinutesDocument3 pagesEd Staff Meeting Minutesapi-236445988No ratings yet
- CPHRM Legal and Regulatory Version 2Document147 pagesCPHRM Legal and Regulatory Version 2Hosam GomaaNo ratings yet
- Andrea KimDocument3 pagesAndrea KimBiju JosephNo ratings yet
- Past, Present, and Future of Antibacterial Economics: Increasing Bacterial Resistance, Limited Antibiotic Pipeline, and Societal ImplicationsDocument14 pagesPast, Present, and Future of Antibacterial Economics: Increasing Bacterial Resistance, Limited Antibiotic Pipeline, and Societal ImplicationsLeonardo SimonciniNo ratings yet
- Abortion BSN 0PR-2: Case Study of BelleDocument27 pagesAbortion BSN 0PR-2: Case Study of BellekervinNo ratings yet
- Part 2 Oral Examination Process PDFDocument9 pagesPart 2 Oral Examination Process PDFTin SantosNo ratings yet
- Dental Hygiene Resume - No ReferencesDocument2 pagesDental Hygiene Resume - No Referencesapi-313829416No ratings yet
- QIMP14 Doctors DirectoryDocument28 pagesQIMP14 Doctors DirectoryShahriar Mostafa100% (3)
- Indonesia Society of Endorcrinology PDFDocument2 pagesIndonesia Society of Endorcrinology PDFAfdol Triatmojo SikumbangNo ratings yet
- Catálogo Benevision N15Document7 pagesCatálogo Benevision N15Filipa VenturaNo ratings yet
- 3 PoshaDocument20 pages3 Poshav_vijayakanth7656No ratings yet