
Dehydroepiandrosterone (DHEA) : Hypes and Hopes
Dehydroepiandrosterone (DHEA) : Hypes and Hopes
You might also like
- Raising Children in IslamDocument40 pagesRaising Children in IslamFaheem Lea100% (1)
- DHEA PrasteronaDocument125 pagesDHEA PrasteronaMiguel Angel Contreras Ramos100% (1)
- Dhea DescriptionDocument23 pagesDhea DescriptionNemes Kovács KataNo ratings yet
- Kroboth 2003Document4 pagesKroboth 2003egrdfgNo ratings yet
- Endocryn DheaDocument3 pagesEndocryn DheaRamona VintilaNo ratings yet
- Ratna Et AlDocument6 pagesRatna Et AleditorijmrhsNo ratings yet
- DHEA Cancer EnvelhecimentoDocument10 pagesDHEA Cancer EnvelhecimentoDr. Ivan MateusNo ratings yet
- Cortisol and DHEA in Development of PsychopathologyDocument56 pagesCortisol and DHEA in Development of PsychopathologyStefaniNo ratings yet
- Butterworth DHEASDocument8 pagesButterworth DHEASMoncef BARZANENo ratings yet
- Article DHEA and AntiagingDocument2 pagesArticle DHEA and AntiagingSatria Adi PutraNo ratings yet
- Legado de Tóxicos en La Etiología de La EADocument2 pagesLegado de Tóxicos en La Etiología de La EAmaria joseNo ratings yet
- Dayan 2013Document12 pagesDayan 2013omar rodriguezNo ratings yet
- New Insights On Attention-Deficit/Hyperactivity Disorder PharmacogenomicsDocument8 pagesNew Insights On Attention-Deficit/Hyperactivity Disorder PharmacogenomicsVeronica BalanNo ratings yet
- Asthma and Dehydroepiandrosterone (DHEA) : Facts and HypothesesDocument5 pagesAsthma and Dehydroepiandrosterone (DHEA) : Facts and HypothesesJosueNo ratings yet
- Harvey 2009Document6 pagesHarvey 2009huwainannisaNo ratings yet
- Pone 0271614Document20 pagesPone 0271614Jefferson LewanNo ratings yet
- Dehydroepiandrosterone Role PDFDocument8 pagesDehydroepiandrosterone Role PDFRiskaNo ratings yet
- DHEA and Aging ArticleDocument5 pagesDHEA and Aging ArticleArdat LiliNo ratings yet
- Rhodiola For de PowerDocument7 pagesRhodiola For de PowerChen222No ratings yet
- DHEA and Its Transformation Into Androgens and Estrogens in Peripheral Target Tissues: IntracrinologyDocument28 pagesDHEA and Its Transformation Into Androgens and Estrogens in Peripheral Target Tissues: IntracrinologyFernanda PérezNo ratings yet
- Dopa Responsive Dystonia in A Child Misdiagnosed As Cerebral PalsyDocument2 pagesDopa Responsive Dystonia in A Child Misdiagnosed As Cerebral PalsyTalib AdilNo ratings yet
- Histone Deacetylases PDFDocument9 pagesHistone Deacetylases PDFATHARVA TANDONNo ratings yet
- Pesticida en EA Comparado Con Controles 2014Document15 pagesPesticida en EA Comparado Con Controles 2014maria joseNo ratings yet
- Recent Genetic Advances in ADHD and DiagDocument12 pagesRecent Genetic Advances in ADHD and DiagBareeha AhmedNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- 10 1016@j NCL 2020 01 004Document18 pages10 1016@j NCL 2020 01 004lucashortencioNo ratings yet
- Apnea Del Sueñoi y Vit DDocument6 pagesApnea Del Sueñoi y Vit Dyanet guzman aybarNo ratings yet
- Supervised Disul Firam's Superior Effectiveness in Alcoholism Treatment: Ethical, Methodological, and Psychological AspectsDocument7 pagesSupervised Disul Firam's Superior Effectiveness in Alcoholism Treatment: Ethical, Methodological, and Psychological AspectsRafia AwanNo ratings yet
- Rhodiola RoseaDocument8 pagesRhodiola RoseapnutsterNo ratings yet
- 1617 FullDocument9 pages1617 FullNuning FebrianyNo ratings yet
- DHEA DR TamilDocument4 pagesDHEA DR TamilDr. Santhi Silambanan, Dept. of Biochemistry, SRUNo ratings yet
- Mode of Action in Human CelDocument2 pagesMode of Action in Human CelrivaldoprimastephianNo ratings yet
- Science of The Total Environment: Ye Yuan, John D. Meeker, Kelly K. FergusonDocument6 pagesScience of The Total Environment: Ye Yuan, John D. Meeker, Kelly K. FergusonSarah Anggita PratiwiNo ratings yet
- Dopamine Serotonin Interactions in Attention Deficit Hyperactivity Disorder ADHDDocument30 pagesDopamine Serotonin Interactions in Attention Deficit Hyperactivity Disorder ADHDpcfernandezdiazNo ratings yet
- JAdd Disease 1Document15 pagesJAdd Disease 1inetwork2001No ratings yet
- Peroksisomal DisordersDocument27 pagesPeroksisomal DisordersLuckyNo ratings yet
- Dopamine Receptors: From Structure To FunctionDocument38 pagesDopamine Receptors: From Structure To FunctionAhmed AlaaNo ratings yet
- The Roles of Dopamine and Noradrenaline in The Pathophysiology and Treatment of Attention-Deficit/ Hyperactivity DisorderDocument13 pagesThe Roles of Dopamine and Noradrenaline in The Pathophysiology and Treatment of Attention-Deficit/ Hyperactivity Disorder-No ratings yet
- Docosahexaenoic Acid Measurements in Food and Dietary ExposureDocument4 pagesDocosahexaenoic Acid Measurements in Food and Dietary ExposureTri WidodoNo ratings yet
- BiomedicinesDocument22 pagesBiomedicinesATIKA INDAH SARINo ratings yet
- Chertow Et AlDocument12 pagesChertow Et AlsheharyarNo ratings yet
- Pi Is 1743609521007529Document9 pagesPi Is 1743609521007529ajfjiwiNo ratings yet
- Zns 9173Document9 pagesZns 9173JuanokNo ratings yet
- Therapeutic ContextDocument10 pagesTherapeutic ContextIsrrel GiNo ratings yet
- Articulo CopDocument46 pagesArticulo CopJorge Luis Archila GuerreroNo ratings yet
- Examining The Effects of Herbs On TestosteroneDocument22 pagesExamining The Effects of Herbs On TestosteroneKelson dos SantosNo ratings yet
- Jurding JiwaDocument8 pagesJurding JiwaAliRifqiAlkaffNo ratings yet
- Abuaish 2021 The Role of Sex Differentiated Variations in Stress Hormones Antiox Neuroimmun Res in Rel To Soc Int Impair in Rodent Model of AutismDocument11 pagesAbuaish 2021 The Role of Sex Differentiated Variations in Stress Hormones Antiox Neuroimmun Res in Rel To Soc Int Impair in Rodent Model of AutismJortegloriaNo ratings yet
- Docosahexaenoic Acid (DHA) : MonographDocument9 pagesDocosahexaenoic Acid (DHA) : MonographBen ClarkeNo ratings yet
- Peretti 1978Document6 pagesPeretti 1978egrdfgNo ratings yet
- Q 2002 Society of The European Journal of Endocrinology: Via Free AccessDocument10 pagesQ 2002 Society of The European Journal of Endocrinology: Via Free AccessThomas ColodelNo ratings yet
- Lack of Defects in Androgen Production in Children With HypospadiasDocument6 pagesLack of Defects in Androgen Production in Children With HypospadiasAndikazaki 74OKNo ratings yet
- 1 s2.0 S266645932300046X MainDocument10 pages1 s2.0 S266645932300046X MainEmmanuel OwonaNo ratings yet
- The Relationship Between Hydration Status Male Sexual Dysfunction and Depression in Hemodialysis PatientsDocument8 pagesThe Relationship Between Hydration Status Male Sexual Dysfunction and Depression in Hemodialysis PatientsMirko ĆalićNo ratings yet
- Review Article: Immunomodulatory Effects Mediated by DopamineDocument32 pagesReview Article: Immunomodulatory Effects Mediated by DopamineCony GSNo ratings yet
- 1 s2.0 S0002916523055235 MainDocument10 pages1 s2.0 S0002916523055235 MainDebbie CharlotteNo ratings yet
- A Possible Plant Adaptogen: Rhodiola RoseaDocument10 pagesA Possible Plant Adaptogen: Rhodiola RoseaAsihPuspitaPutriNo ratings yet
- New Medications Neuropsychiatric DisordersDocument15 pagesNew Medications Neuropsychiatric DisordersJorge Luis German BecerraNo ratings yet
- 1 s2.0 S2212877821001113 MainDocument7 pages1 s2.0 S2212877821001113 MainMonaNo ratings yet
- NIH Public Access: Pharmacotherapy For Stimulant-Related DisordersDocument18 pagesNIH Public Access: Pharmacotherapy For Stimulant-Related DisordersLutfiAnny Rahman HakimNo ratings yet
- The Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianFrom EverandThe Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianNo ratings yet
- Chapter 2-Computer Security Attacks and ThreatsDocument40 pagesChapter 2-Computer Security Attacks and ThreatsYohannes DerejeNo ratings yet
- Almonte HistoryDocument3 pagesAlmonte HistoryAngelo ErispeNo ratings yet
- Critical Thinking Definitions PDFDocument2 pagesCritical Thinking Definitions PDFAlpha Niño S SanguenzaNo ratings yet
- Merton On Structural FunctionalismDocument6 pagesMerton On Structural FunctionalismJahnaviSinghNo ratings yet
- Gmail - Request For Candidates Recruitment To The Structural Engg Dept - Kindly Consider This As Most Urgent - 05-02-2022Document2 pagesGmail - Request For Candidates Recruitment To The Structural Engg Dept - Kindly Consider This As Most Urgent - 05-02-2022Sreeelakshmi P NNo ratings yet
- Planes of SymmetryDocument38 pagesPlanes of SymmetryRuchika Chandna83% (6)
- LocationDocument12 pagesLocationPavithra GowthamNo ratings yet
- EZ-212 ManualDocument32 pagesEZ-212 ManualapiadmbrNo ratings yet
- A REVIEW OF SOIL ERODIBILITY Case Study of UGBOJU Settlement of OTURKPO Local Government Area of Benue State NigeriaDocument9 pagesA REVIEW OF SOIL ERODIBILITY Case Study of UGBOJU Settlement of OTURKPO Local Government Area of Benue State NigeriaTIZA MICHAEL B.Engr., BBS, MBA, Aff. M. ASCE, ASS.M. UACSE, M. IAENG. M.ITE.No ratings yet
- Agung Chrisyancandra MobonguniDocument2 pagesAgung Chrisyancandra Mobongunialfibaria0% (1)
- ESP Standard SizingDocument131 pagesESP Standard Sizingmohamed gamal100% (2)
- The 1 Catholic Mass in The PhilippinesDocument16 pagesThe 1 Catholic Mass in The PhilippinesRosalie AlitaoNo ratings yet
- HR Score CardDocument16 pagesHR Score Cardvijay77777No ratings yet
- Hardcarb - Corporate ProfileDocument8 pagesHardcarb - Corporate ProfileJimit ShahNo ratings yet
- Project - Portugal An Unlikely Empire - Student GuideDocument5 pagesProject - Portugal An Unlikely Empire - Student GuideBeanieNo ratings yet
- Sample Test 1Document3 pagesSample Test 1Bình Phạm ThịNo ratings yet
- Chapter 10 (Epjj)Document59 pagesChapter 10 (Epjj)syuhadaNo ratings yet
- Worksheet (2023-24) Grade: 10 Subject: Information TechnologyDocument49 pagesWorksheet (2023-24) Grade: 10 Subject: Information TechnologyINFWHATNo ratings yet
- SAP Proj Builder Previewer PDFDocument24 pagesSAP Proj Builder Previewer PDFPradeep JagirdarNo ratings yet
- Food Grade Anti-Corrosion Grease: Special FeaturesDocument2 pagesFood Grade Anti-Corrosion Grease: Special Featureschem KhanNo ratings yet
- Formulation Development and Compatibility Study of Dexketoprofen Injection Used in The Management of Post-Operative PainDocument7 pagesFormulation Development and Compatibility Study of Dexketoprofen Injection Used in The Management of Post-Operative PainAdeeva MaulidaNo ratings yet
- Antenna RFI MonitoringDocument71 pagesAntenna RFI MonitoringmoannaNo ratings yet
- The Tallboy BombDocument28 pagesThe Tallboy BombKIRU SILVIUNo ratings yet
- Social Studies K-5Document75 pagesSocial Studies K-5SriniNo ratings yet
- KB Shape CodesDocument9 pagesKB Shape CodesPrashanth TNo ratings yet
- Assignment#2 Submitted To: Dr. Aliya Submitted By: Issma Munir Abbasi MS-SP-19-REL-013Document3 pagesAssignment#2 Submitted To: Dr. Aliya Submitted By: Issma Munir Abbasi MS-SP-19-REL-013issma abbasiNo ratings yet
- Worlds Beyond Our Ice Wall Isoa4Document10 pagesWorlds Beyond Our Ice Wall Isoa4hujankopiairNo ratings yet
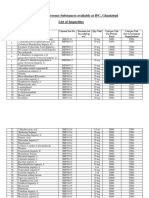
- List of IP Reference Substances Available at IPC, Ghaziabad List of ImpuritiesDocument4 pagesList of IP Reference Substances Available at IPC, Ghaziabad List of ImpuritiesUrva VasavadaNo ratings yet
- Appendix E-Baseline Design StandardsDocument26 pagesAppendix E-Baseline Design StandardsReshad AtmarNo ratings yet

























































































Download as pdf or txt
You might also like
- Raising Children in IslamDocument40 pagesRaising Children in IslamFaheem Lea100% (1)
- DHEA PrasteronaDocument125 pagesDHEA PrasteronaMiguel Angel Contreras Ramos100% (1)
- Dhea DescriptionDocument23 pagesDhea DescriptionNemes Kovács KataNo ratings yet
- Kroboth 2003Document4 pagesKroboth 2003egrdfgNo ratings yet
- Endocryn DheaDocument3 pagesEndocryn DheaRamona VintilaNo ratings yet
- Ratna Et AlDocument6 pagesRatna Et AleditorijmrhsNo ratings yet
- DHEA Cancer EnvelhecimentoDocument10 pagesDHEA Cancer EnvelhecimentoDr. Ivan MateusNo ratings yet
- Cortisol and DHEA in Development of PsychopathologyDocument56 pagesCortisol and DHEA in Development of PsychopathologyStefaniNo ratings yet
- Butterworth DHEASDocument8 pagesButterworth DHEASMoncef BARZANENo ratings yet
- Article DHEA and AntiagingDocument2 pagesArticle DHEA and AntiagingSatria Adi PutraNo ratings yet
- Legado de Tóxicos en La Etiología de La EADocument2 pagesLegado de Tóxicos en La Etiología de La EAmaria joseNo ratings yet
- Dayan 2013Document12 pagesDayan 2013omar rodriguezNo ratings yet
- New Insights On Attention-Deficit/Hyperactivity Disorder PharmacogenomicsDocument8 pagesNew Insights On Attention-Deficit/Hyperactivity Disorder PharmacogenomicsVeronica BalanNo ratings yet
- Asthma and Dehydroepiandrosterone (DHEA) : Facts and HypothesesDocument5 pagesAsthma and Dehydroepiandrosterone (DHEA) : Facts and HypothesesJosueNo ratings yet
- Harvey 2009Document6 pagesHarvey 2009huwainannisaNo ratings yet
- Pone 0271614Document20 pagesPone 0271614Jefferson LewanNo ratings yet
- Dehydroepiandrosterone Role PDFDocument8 pagesDehydroepiandrosterone Role PDFRiskaNo ratings yet
- DHEA and Aging ArticleDocument5 pagesDHEA and Aging ArticleArdat LiliNo ratings yet
- Rhodiola For de PowerDocument7 pagesRhodiola For de PowerChen222No ratings yet
- DHEA and Its Transformation Into Androgens and Estrogens in Peripheral Target Tissues: IntracrinologyDocument28 pagesDHEA and Its Transformation Into Androgens and Estrogens in Peripheral Target Tissues: IntracrinologyFernanda PérezNo ratings yet
- Dopa Responsive Dystonia in A Child Misdiagnosed As Cerebral PalsyDocument2 pagesDopa Responsive Dystonia in A Child Misdiagnosed As Cerebral PalsyTalib AdilNo ratings yet
- Histone Deacetylases PDFDocument9 pagesHistone Deacetylases PDFATHARVA TANDONNo ratings yet
- Pesticida en EA Comparado Con Controles 2014Document15 pagesPesticida en EA Comparado Con Controles 2014maria joseNo ratings yet
- Recent Genetic Advances in ADHD and DiagDocument12 pagesRecent Genetic Advances in ADHD and DiagBareeha AhmedNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- 10 1016@j NCL 2020 01 004Document18 pages10 1016@j NCL 2020 01 004lucashortencioNo ratings yet
- Apnea Del Sueñoi y Vit DDocument6 pagesApnea Del Sueñoi y Vit Dyanet guzman aybarNo ratings yet
- Supervised Disul Firam's Superior Effectiveness in Alcoholism Treatment: Ethical, Methodological, and Psychological AspectsDocument7 pagesSupervised Disul Firam's Superior Effectiveness in Alcoholism Treatment: Ethical, Methodological, and Psychological AspectsRafia AwanNo ratings yet
- Rhodiola RoseaDocument8 pagesRhodiola RoseapnutsterNo ratings yet
- 1617 FullDocument9 pages1617 FullNuning FebrianyNo ratings yet
- DHEA DR TamilDocument4 pagesDHEA DR TamilDr. Santhi Silambanan, Dept. of Biochemistry, SRUNo ratings yet
- Mode of Action in Human CelDocument2 pagesMode of Action in Human CelrivaldoprimastephianNo ratings yet
- Science of The Total Environment: Ye Yuan, John D. Meeker, Kelly K. FergusonDocument6 pagesScience of The Total Environment: Ye Yuan, John D. Meeker, Kelly K. FergusonSarah Anggita PratiwiNo ratings yet
- Dopamine Serotonin Interactions in Attention Deficit Hyperactivity Disorder ADHDDocument30 pagesDopamine Serotonin Interactions in Attention Deficit Hyperactivity Disorder ADHDpcfernandezdiazNo ratings yet
- JAdd Disease 1Document15 pagesJAdd Disease 1inetwork2001No ratings yet
- Peroksisomal DisordersDocument27 pagesPeroksisomal DisordersLuckyNo ratings yet
- Dopamine Receptors: From Structure To FunctionDocument38 pagesDopamine Receptors: From Structure To FunctionAhmed AlaaNo ratings yet
- The Roles of Dopamine and Noradrenaline in The Pathophysiology and Treatment of Attention-Deficit/ Hyperactivity DisorderDocument13 pagesThe Roles of Dopamine and Noradrenaline in The Pathophysiology and Treatment of Attention-Deficit/ Hyperactivity Disorder-No ratings yet
- Docosahexaenoic Acid Measurements in Food and Dietary ExposureDocument4 pagesDocosahexaenoic Acid Measurements in Food and Dietary ExposureTri WidodoNo ratings yet
- BiomedicinesDocument22 pagesBiomedicinesATIKA INDAH SARINo ratings yet
- Chertow Et AlDocument12 pagesChertow Et AlsheharyarNo ratings yet
- Pi Is 1743609521007529Document9 pagesPi Is 1743609521007529ajfjiwiNo ratings yet
- Zns 9173Document9 pagesZns 9173JuanokNo ratings yet
- Therapeutic ContextDocument10 pagesTherapeutic ContextIsrrel GiNo ratings yet
- Articulo CopDocument46 pagesArticulo CopJorge Luis Archila GuerreroNo ratings yet
- Examining The Effects of Herbs On TestosteroneDocument22 pagesExamining The Effects of Herbs On TestosteroneKelson dos SantosNo ratings yet
- Jurding JiwaDocument8 pagesJurding JiwaAliRifqiAlkaffNo ratings yet
- Abuaish 2021 The Role of Sex Differentiated Variations in Stress Hormones Antiox Neuroimmun Res in Rel To Soc Int Impair in Rodent Model of AutismDocument11 pagesAbuaish 2021 The Role of Sex Differentiated Variations in Stress Hormones Antiox Neuroimmun Res in Rel To Soc Int Impair in Rodent Model of AutismJortegloriaNo ratings yet
- Docosahexaenoic Acid (DHA) : MonographDocument9 pagesDocosahexaenoic Acid (DHA) : MonographBen ClarkeNo ratings yet
- Peretti 1978Document6 pagesPeretti 1978egrdfgNo ratings yet
- Q 2002 Society of The European Journal of Endocrinology: Via Free AccessDocument10 pagesQ 2002 Society of The European Journal of Endocrinology: Via Free AccessThomas ColodelNo ratings yet
- Lack of Defects in Androgen Production in Children With HypospadiasDocument6 pagesLack of Defects in Androgen Production in Children With HypospadiasAndikazaki 74OKNo ratings yet
- 1 s2.0 S266645932300046X MainDocument10 pages1 s2.0 S266645932300046X MainEmmanuel OwonaNo ratings yet
- The Relationship Between Hydration Status Male Sexual Dysfunction and Depression in Hemodialysis PatientsDocument8 pagesThe Relationship Between Hydration Status Male Sexual Dysfunction and Depression in Hemodialysis PatientsMirko ĆalićNo ratings yet
- Review Article: Immunomodulatory Effects Mediated by DopamineDocument32 pagesReview Article: Immunomodulatory Effects Mediated by DopamineCony GSNo ratings yet
- 1 s2.0 S0002916523055235 MainDocument10 pages1 s2.0 S0002916523055235 MainDebbie CharlotteNo ratings yet
- A Possible Plant Adaptogen: Rhodiola RoseaDocument10 pagesA Possible Plant Adaptogen: Rhodiola RoseaAsihPuspitaPutriNo ratings yet
- New Medications Neuropsychiatric DisordersDocument15 pagesNew Medications Neuropsychiatric DisordersJorge Luis German BecerraNo ratings yet
- 1 s2.0 S2212877821001113 MainDocument7 pages1 s2.0 S2212877821001113 MainMonaNo ratings yet
- NIH Public Access: Pharmacotherapy For Stimulant-Related DisordersDocument18 pagesNIH Public Access: Pharmacotherapy For Stimulant-Related DisordersLutfiAnny Rahman HakimNo ratings yet
- The Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianFrom EverandThe Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianNo ratings yet
- Chapter 2-Computer Security Attacks and ThreatsDocument40 pagesChapter 2-Computer Security Attacks and ThreatsYohannes DerejeNo ratings yet
- Almonte HistoryDocument3 pagesAlmonte HistoryAngelo ErispeNo ratings yet
- Critical Thinking Definitions PDFDocument2 pagesCritical Thinking Definitions PDFAlpha Niño S SanguenzaNo ratings yet
- Merton On Structural FunctionalismDocument6 pagesMerton On Structural FunctionalismJahnaviSinghNo ratings yet
- Gmail - Request For Candidates Recruitment To The Structural Engg Dept - Kindly Consider This As Most Urgent - 05-02-2022Document2 pagesGmail - Request For Candidates Recruitment To The Structural Engg Dept - Kindly Consider This As Most Urgent - 05-02-2022Sreeelakshmi P NNo ratings yet
- Planes of SymmetryDocument38 pagesPlanes of SymmetryRuchika Chandna83% (6)
- LocationDocument12 pagesLocationPavithra GowthamNo ratings yet
- EZ-212 ManualDocument32 pagesEZ-212 ManualapiadmbrNo ratings yet
- A REVIEW OF SOIL ERODIBILITY Case Study of UGBOJU Settlement of OTURKPO Local Government Area of Benue State NigeriaDocument9 pagesA REVIEW OF SOIL ERODIBILITY Case Study of UGBOJU Settlement of OTURKPO Local Government Area of Benue State NigeriaTIZA MICHAEL B.Engr., BBS, MBA, Aff. M. ASCE, ASS.M. UACSE, M. IAENG. M.ITE.No ratings yet
- Agung Chrisyancandra MobonguniDocument2 pagesAgung Chrisyancandra Mobongunialfibaria0% (1)
- ESP Standard SizingDocument131 pagesESP Standard Sizingmohamed gamal100% (2)
- The 1 Catholic Mass in The PhilippinesDocument16 pagesThe 1 Catholic Mass in The PhilippinesRosalie AlitaoNo ratings yet
- HR Score CardDocument16 pagesHR Score Cardvijay77777No ratings yet
- Hardcarb - Corporate ProfileDocument8 pagesHardcarb - Corporate ProfileJimit ShahNo ratings yet
- Project - Portugal An Unlikely Empire - Student GuideDocument5 pagesProject - Portugal An Unlikely Empire - Student GuideBeanieNo ratings yet
- Sample Test 1Document3 pagesSample Test 1Bình Phạm ThịNo ratings yet
- Chapter 10 (Epjj)Document59 pagesChapter 10 (Epjj)syuhadaNo ratings yet
- Worksheet (2023-24) Grade: 10 Subject: Information TechnologyDocument49 pagesWorksheet (2023-24) Grade: 10 Subject: Information TechnologyINFWHATNo ratings yet
- SAP Proj Builder Previewer PDFDocument24 pagesSAP Proj Builder Previewer PDFPradeep JagirdarNo ratings yet
- Food Grade Anti-Corrosion Grease: Special FeaturesDocument2 pagesFood Grade Anti-Corrosion Grease: Special Featureschem KhanNo ratings yet
- Formulation Development and Compatibility Study of Dexketoprofen Injection Used in The Management of Post-Operative PainDocument7 pagesFormulation Development and Compatibility Study of Dexketoprofen Injection Used in The Management of Post-Operative PainAdeeva MaulidaNo ratings yet
- Antenna RFI MonitoringDocument71 pagesAntenna RFI MonitoringmoannaNo ratings yet
- The Tallboy BombDocument28 pagesThe Tallboy BombKIRU SILVIUNo ratings yet
- Social Studies K-5Document75 pagesSocial Studies K-5SriniNo ratings yet
- KB Shape CodesDocument9 pagesKB Shape CodesPrashanth TNo ratings yet
- Assignment#2 Submitted To: Dr. Aliya Submitted By: Issma Munir Abbasi MS-SP-19-REL-013Document3 pagesAssignment#2 Submitted To: Dr. Aliya Submitted By: Issma Munir Abbasi MS-SP-19-REL-013issma abbasiNo ratings yet
- Worlds Beyond Our Ice Wall Isoa4Document10 pagesWorlds Beyond Our Ice Wall Isoa4hujankopiairNo ratings yet
- List of IP Reference Substances Available at IPC, Ghaziabad List of ImpuritiesDocument4 pagesList of IP Reference Substances Available at IPC, Ghaziabad List of ImpuritiesUrva VasavadaNo ratings yet
- Appendix E-Baseline Design StandardsDocument26 pagesAppendix E-Baseline Design StandardsReshad AtmarNo ratings yet