Download as pdf or txt
You might also like
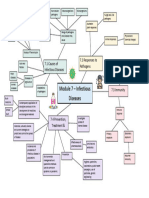
- Module 7 Mind Map BiologyDocument1 pageModule 7 Mind Map BiologyAltSpace TimeNo ratings yet
- Implement and Monitor Infection Control Policies and ProceduresDocument29 pagesImplement and Monitor Infection Control Policies and ProceduresJM Ramos100% (2)
- DischargeDocument2 pagesDischargeபென்ஸிஹர்No ratings yet
- IMDocument56 pagesIMHannahboi G DesckyNo ratings yet
- Anatomy and Pathophysiology of ProstrateDocument44 pagesAnatomy and Pathophysiology of Prostraterajan kumar100% (3)
- Ijerph 17 07233Document12 pagesIjerph 17 07233Mumtaz MaulanaNo ratings yet
- An Intervention of 12 Weeks of (V)Document16 pagesAn Intervention of 12 Weeks of (V)Isabel MarcoNo ratings yet
- Effect of A 26-Month Floorball Training On Male Elderly's Cardiovascular Fitness, Glucose Control, Body Composition, and Functional CapacityDocument10 pagesEffect of A 26-Month Floorball Training On Male Elderly's Cardiovascular Fitness, Glucose Control, Body Composition, and Functional CapacityYanuarwongiiNo ratings yet
- Study Proposal For Senior CitizensDocument15 pagesStudy Proposal For Senior CitizensParul ThakurNo ratings yet
- Financial Impact of A Comprehensive Multisite Workplace Health Promotion ProgramDocument7 pagesFinancial Impact of A Comprehensive Multisite Workplace Health Promotion ProgramGaurav SharmaNo ratings yet
- Sam-Kit Tin T. Et Al. (2019)Document7 pagesSam-Kit Tin T. Et Al. (2019)Andrés MenesesNo ratings yet
- Jurnal 444Document7 pagesJurnal 444rizalmantaNo ratings yet
- Art 272Document8 pagesArt 272Homemade ANo ratings yet
- In-Season Weightlifting Training Exercise in Healthy Male Handball Players: E Muscle Volume, Maximal Strength, and Ball-Throwing VelocityDocument14 pagesIn-Season Weightlifting Training Exercise in Healthy Male Handball Players: E Muscle Volume, Maximal Strength, and Ball-Throwing VelocityPabloT81No ratings yet
- 1 s2.0 S2095254617301187 MainDocument10 pages1 s2.0 S2095254617301187 MainYanuarwongiiNo ratings yet
- 2006 20 1 Two Short Daily Activity Bouts VS One LongDocument6 pages2006 20 1 Two Short Daily Activity Bouts VS One LongVictor Hugo VeraNo ratings yet
- Fitness in SportsDocument7 pagesFitness in SportsFifyana Fify AnaNo ratings yet
- Exercise Guidelines in Pregnancy: New PerspectivesDocument16 pagesExercise Guidelines in Pregnancy: New PerspectivesCarlos VieiraNo ratings yet
- Nightingale 2018Document10 pagesNightingale 2018Ayu SuprabawatiNo ratings yet
- Thematic Poster Bioenergetics and Training: (No Relationships Reported)Document2 pagesThematic Poster Bioenergetics and Training: (No Relationships Reported)pantufoNo ratings yet
- JPES Chenetal 2016 PDFDocument7 pagesJPES Chenetal 2016 PDFRizqiAnnisaPermatasariNo ratings yet
- Prospective Echocardiographic Assessment of Androgenic-Anabolic Steroids Effects On Cardiac Structure and Function in Strength Athletes.Document8 pagesProspective Echocardiographic Assessment of Androgenic-Anabolic Steroids Effects On Cardiac Structure and Function in Strength Athletes.Waleed El-HawarryNo ratings yet
- Exercice Is MedicineDocument55 pagesExercice Is MedicineDario MoralesNo ratings yet
- Artikel Review Kesehatan OlahragaDocument10 pagesArtikel Review Kesehatan OlahragaTRI PRASETYONo ratings yet
- Prescription of Resistance Training For Healthy PopulationsDocument12 pagesPrescription of Resistance Training For Healthy PopulationsChristine LeeNo ratings yet
- Physiology & Behavior: SciencedirectDocument8 pagesPhysiology & Behavior: SciencedirectScottNo ratings yet
- Krustrup Et Al - 2009 - Recreational Soccer Is An Effective Health-Promoting Activity For Untrained MenDocument7 pagesKrustrup Et Al - 2009 - Recreational Soccer Is An Effective Health-Promoting Activity For Untrained MenIainNo ratings yet
- 1 s2.0 S2405587515300263 MainDocument8 pages1 s2.0 S2405587515300263 Maindianaerlita97No ratings yet
- Versic 2021Document16 pagesVersic 2021Willian da costaNo ratings yet
- Physiotherapy 3 1 2Document4 pagesPhysiotherapy 3 1 2AjiNo ratings yet
- Ajay VermaDocument18 pagesAjay VermabugsbusgNo ratings yet
- Phenomenon of Athlete'S Heart, Positive Physiological Adaptation To Exercise: When and How?Document6 pagesPhenomenon of Athlete'S Heart, Positive Physiological Adaptation To Exercise: When and How?Jasmina Pluncevic GligoroskaNo ratings yet
- 1 s2.0 S2405587515300263 MainDocument8 pages1 s2.0 S2405587515300263 MainmaracioNo ratings yet
- 1320-Article Text-2447-1-10-20200722Document5 pages1320-Article Text-2447-1-10-20200722KURNIA PRISTIYANINo ratings yet
- Babraj EffectsOfIn-SeasonUphillSprintingOnPhysicalCharacteristics Author 2015Document15 pagesBabraj EffectsOfIn-SeasonUphillSprintingOnPhysicalCharacteristics Author 2015Kostas LiougkosNo ratings yet
- Final Project Exp590-3Document19 pagesFinal Project Exp590-3api-315973465No ratings yet
- High Intensity Small Muscle Mass Training in Patients With CHFDocument7 pagesHigh Intensity Small Muscle Mass Training in Patients With CHFbcvaughn019No ratings yet
- Zavorsky Longo 2011Document17 pagesZavorsky Longo 2011Heidy Bravo RamosNo ratings yet
- Muhammad Faisol 2018A 015Document4 pagesMuhammad Faisol 2018A 015muhammadfaisol933No ratings yet
- Protocolo Valés-Badilla Et Al., 2022Document12 pagesProtocolo Valés-Badilla Et Al., 2022Alberto I. Cruz FloresNo ratings yet
- Jurnal 1Document6 pagesJurnal 1fister19 rifaudinNo ratings yet
- Effects of Low-Intensity Resistance Exercise With Vascular Occlusion On Physical Function in Healthy Elderly People.-2Document7 pagesEffects of Low-Intensity Resistance Exercise With Vascular Occlusion On Physical Function in Healthy Elderly People.-2Ingrid Ramirez PNo ratings yet
- Comparative Analysis of Hematological Parameters in Well Trained Athletes and Untrained MenDocument5 pagesComparative Analysis of Hematological Parameters in Well Trained Athletes and Untrained MensarahNo ratings yet
- (Human Movement) Blood Pressure Responses After A Session of Functional Training in Young Adults and The Elderly A Pilot StudyDocument7 pages(Human Movement) Blood Pressure Responses After A Session of Functional Training in Young Adults and The Elderly A Pilot StudyEvaNo ratings yet
- JurnalDocument7 pagesJurnalghozi hilmyNo ratings yet
- Jurnal Olahraga 2Document7 pagesJurnal Olahraga 2Gangsar DamaiNo ratings yet
- Wa0011.Document6 pagesWa0011.MOHD HARIZ ADDNANNo ratings yet
- Prescripción EjerciciosDocument9 pagesPrescripción Ejercicioschuchinchis pedoNo ratings yet
- 04 - Cardiometabolic Effects of High-Intensity Hybrid Functional Electrical Stimulation Exercise After Spinal Cord InjuryDocument20 pages04 - Cardiometabolic Effects of High-Intensity Hybrid Functional Electrical Stimulation Exercise After Spinal Cord Injurywellington contieroNo ratings yet
- The Relationship Between Physical Activity Levels and Mental Health in Individuals With Spinal Cord Injury in South KoreaDocument9 pagesThe Relationship Between Physical Activity Levels and Mental Health in Individuals With Spinal Cord Injury in South KoreaĐỗ Văn ĐứcNo ratings yet
- HolidaysDocument12 pagesHolidaysGabriela PopescuNo ratings yet
- Harrington Stress Chapter 11 PPT 2023Document75 pagesHarrington Stress Chapter 11 PPT 2023mohapisthaba77No ratings yet
- Subjective Training Recovery MeasuresDocument11 pagesSubjective Training Recovery Measuresjlambe9No ratings yet
- Intra Dial y TicDocument8 pagesIntra Dial y Ticratna220693No ratings yet
- 527 - Research ProposalDocument15 pages527 - Research ProposalPanktiNo ratings yet
- Ffects of Neuromuscular Training On Motor: E Competence and Physical Performance in Young Female Volleyball PlayersDocument12 pagesFfects of Neuromuscular Training On Motor: E Competence and Physical Performance in Young Female Volleyball PlayersnurulaqilahizzatiNo ratings yet
- Ffect of Static and Dynamic Stretching Exercises: The E On Sprint Ability of Recreational Male Volleyball PlayersDocument10 pagesFfect of Static and Dynamic Stretching Exercises: The E On Sprint Ability of Recreational Male Volleyball Players'fanny Quenhita'No ratings yet
- MemberDocument8 pagesMemberHuy HoàngNo ratings yet
- Cardiovascular Responses During RecreationalDocument7 pagesCardiovascular Responses During RecreationalmarcferrNo ratings yet
- 10 1111@sms 13853Document17 pages10 1111@sms 13853Cintia BeatrizNo ratings yet
- Research Paper DOMASIG ENGLISHDocument10 pagesResearch Paper DOMASIG ENGLISHAustin FerweloNo ratings yet
- Evaluating the Relation Between Maximum Heart Rate and Resting Heart Rate in Three Groups of People Nonathletes الدراسة مهمةathletesDocument4 pagesEvaluating the Relation Between Maximum Heart Rate and Resting Heart Rate in Three Groups of People Nonathletes الدراسة مهمةathletesabdmalek forloulNo ratings yet
- Inter HugoDocument10 pagesInter HugorizkaNo ratings yet
- Aerobic Power in JudoDocument6 pagesAerobic Power in JudoMaciejNo ratings yet
- Exercise Physiology for the Pediatric and Congenital CardiologistFrom EverandExercise Physiology for the Pediatric and Congenital CardiologistNo ratings yet
- Alopecia Areata in Covid 19 Case ReportDocument2 pagesAlopecia Areata in Covid 19 Case ReportAnti TjahyaNo ratings yet
- Lymphatic Drainage Massage Intake Form: Medical InformationDocument1 pageLymphatic Drainage Massage Intake Form: Medical InformationNoé PolancoNo ratings yet
- Erectile Function After Partial Penectomy For Penile CancerDocument8 pagesErectile Function After Partial Penectomy For Penile CancerTai rascunhos TaiNo ratings yet
- Physical Therapy Patient Assessment FormDocument7 pagesPhysical Therapy Patient Assessment FormZA IDNo ratings yet
- Research EssayDocument9 pagesResearch Essayapi-550531643No ratings yet
- Grieco Et Al-2023-Intensive Care MedicineDocument4 pagesGrieco Et Al-2023-Intensive Care MedicineDr Vikas GuptaNo ratings yet
- Unit 1 - Week (1) - Comprehensive Assessment: Intended Learning Outcomes (Week 1-ILO)Document28 pagesUnit 1 - Week (1) - Comprehensive Assessment: Intended Learning Outcomes (Week 1-ILO)John Van Dave TaturoNo ratings yet
- Ankle & Foot Exam - OSCE StationsDocument2 pagesAnkle & Foot Exam - OSCE StationsEmiel AwadNo ratings yet
- 01 1 PDFDocument8 pages01 1 PDFpravikumar1989No ratings yet
- NP - V Psyc pb08Document121 pagesNP - V Psyc pb08Reyna Marie Labadan-LasacarNo ratings yet
- Balance Retraining - YardleyDocument10 pagesBalance Retraining - YardleyMeenakshiputraeashwarprasad MacherlaNo ratings yet
- Accounting Information Systems 5th Edition Parkes Solutions ManualDocument36 pagesAccounting Information Systems 5th Edition Parkes Solutions Manualnubilegoggler.i8cm100% (18)
- Blood GlucoseDocument8 pagesBlood Glucoseعبدالرحمن عابدNo ratings yet
- Science 9 First Quarter ALL NotesDocument9 pagesScience 9 First Quarter ALL Notesliannicole884No ratings yet
- In Vitro Anti Arthritic Activity of Acacia Catechu WilldDocument3 pagesIn Vitro Anti Arthritic Activity of Acacia Catechu WilldEditor IJTSRDNo ratings yet
- Year A EBM Semester 1 EditedDocument96 pagesYear A EBM Semester 1 EditedMary AmeenNo ratings yet
- Atreyi Chakraborty, Et AlDocument9 pagesAtreyi Chakraborty, Et Alkavya bharadhwajNo ratings yet
- 024 Defining-Value-Vbhc enDocument94 pages024 Defining-Value-Vbhc enmert05No ratings yet
- Psychopathology/Problems in LivingDocument44 pagesPsychopathology/Problems in LivingDeadly ChillerNo ratings yet
- TOPIC 1 Laboratory SafetyDocument7 pagesTOPIC 1 Laboratory SafetyJames Anthony ParasNo ratings yet
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungDocument47 pagesKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiNo ratings yet
- 4 Depression Rissmann Engl 2008Document7 pages4 Depression Rissmann Engl 2008Nina Elezovic SimunovicNo ratings yet
- VitaminsDocument15 pagesVitaminsNaseer UllahNo ratings yet
- Clinical Conditions of Hepatitis BDocument2 pagesClinical Conditions of Hepatitis BnurseNo ratings yet
- Birth TraumaDocument57 pagesBirth TraumaAbu HajerahNo ratings yet