Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- DHA Dental QuestionsDocument297 pagesDHA Dental QuestionsKhalid Iqbal91% (22)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Drug StudyDocument13 pagesDrug StudyGi Ey ElNo ratings yet
- 1 s2.0 S1347861316300251 MainDocument107 pages1 s2.0 S1347861316300251 MainNurul HafizaNo ratings yet
- Antibiotic Cross-Sensitivity Chart PDFDocument1 pageAntibiotic Cross-Sensitivity Chart PDFanareadsNo ratings yet
- ClearPoint Healthcare KPIsDocument19 pagesClearPoint Healthcare KPIsJosue Paz100% (1)
- Identification InfectionDocument6 pagesIdentification Infectioneva arna abrarNo ratings yet
- Modern Wound Care (Article Journal)Document14 pagesModern Wound Care (Article Journal)eva arna abrarNo ratings yet
- Clinical Relevance MicrobiologyDocument14 pagesClinical Relevance Microbiologyeva arna abrarNo ratings yet
- Biomarker For InfectionDocument21 pagesBiomarker For Infectioneva arna abrarNo ratings yet
- Community Wound BacteriDocument11 pagesCommunity Wound Bacterieva arna abrarNo ratings yet
- Bioburden in Chronic WoundDocument24 pagesBioburden in Chronic Woundeva arna abrarNo ratings yet
- Chronic Wound BiofilmDocument9 pagesChronic Wound Biofilmeva arna abrarNo ratings yet
- Research Methods For Nurses and MidwivesDocument5 pagesResearch Methods For Nurses and Midwiveseva arna abrarNo ratings yet
- Women & Diabetes Our Right To A Healthy FutureDocument4 pagesWomen & Diabetes Our Right To A Healthy Futureeva arna abrarNo ratings yet
- Management of Wounds in The Community: Five Principles: Clinical FocusDocument4 pagesManagement of Wounds in The Community: Five Principles: Clinical Focuseva arna abrarNo ratings yet
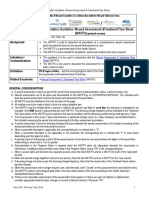
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)Document4 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)eva arna abrarNo ratings yet
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (WATFS) Portrait Version With PSLS#Document6 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (WATFS) Portrait Version With PSLS#eva arna abrarNo ratings yet
- Ound Ssessment and Anagement: Document Summary/Key PointsDocument21 pagesOund Ssessment and Anagement: Document Summary/Key Pointseva arna abrarNo ratings yet
- Lab 2Document22 pagesLab 2fgnjdgnNo ratings yet
- Colds: What Is A Cold?Document2 pagesColds: What Is A Cold?Mocha BorgsNo ratings yet
- VITAMANIADocument4 pagesVITAMANIAiceeiNo ratings yet
- 2022 - Acute Kidney Injury and Critical Care NephrologyDocument123 pages2022 - Acute Kidney Injury and Critical Care NephrologyEdson MarquesNo ratings yet
- Effects of Non-Ionizing Radiation by Hitarth Mihs-IsTARDocument26 pagesEffects of Non-Ionizing Radiation by Hitarth Mihs-IsTARHM04No ratings yet
- Salt and High Blood Pressure: Sailesh MOHAN and Norm R. C. CAMPBELLDocument11 pagesSalt and High Blood Pressure: Sailesh MOHAN and Norm R. C. CAMPBELLIndadul MozumdarNo ratings yet
- A 1 CDocument8 pagesA 1 CRajiv Ranjan100% (1)
- Anatomy MCQ SBA eMRCSDocument121 pagesAnatomy MCQ SBA eMRCSTowhid HasanNo ratings yet
- 5096 s07 Ms 2Document7 pages5096 s07 Ms 2mstudy1234560% (1)
- Kuliah 8, (Pras2021) Obat Anti Kanker (Kemoterapi)Document35 pagesKuliah 8, (Pras2021) Obat Anti Kanker (Kemoterapi)Nur Afiya NandaNo ratings yet
- January VIPDocument52 pagesJanuary VIPbeaumontenterpriseNo ratings yet
- Tru Trac User ManualDocument41 pagesTru Trac User ManualHAITHM MURSHEDNo ratings yet
- Icm Rehab Medik Senin 28 OktDocument5 pagesIcm Rehab Medik Senin 28 OktsylviaNo ratings yet
- Varisara Kriya PDFDocument14 pagesVarisara Kriya PDFGottimukkala Muralikrishna100% (1)
- Genetic Mutation Research Student HandoutDocument9 pagesGenetic Mutation Research Student Handoutapi-369085916No ratings yet
- Osteoporosis PDFDocument4 pagesOsteoporosis PDFmawarNo ratings yet
- Joint Seminar With SFEMG/QEMG Group: Single Fiber EMG and Quantitative EMGDocument1 pageJoint Seminar With SFEMG/QEMG Group: Single Fiber EMG and Quantitative EMGShauki AliNo ratings yet
- Complications of 3rd Molar SurgeryDocument12 pagesComplications of 3rd Molar Surgeryhamad_kayani_774954No ratings yet
- Latest Thesis. Rough Print12Document107 pagesLatest Thesis. Rough Print12Ajmal Hussain100% (1)
- Physical Examinations Respiratory System: InspectionDocument5 pagesPhysical Examinations Respiratory System: InspectionAzizan HannyNo ratings yet
- Biology Contents - RPSC FSO by Food TecKnowDocument35 pagesBiology Contents - RPSC FSO by Food TecKnowRahul JainNo ratings yet
- SEMI Final Coverage Fundamentals of NursingDocument14 pagesSEMI Final Coverage Fundamentals of NursingGlory NeriNo ratings yet
- Biogeography and TaxonomyDocument291 pagesBiogeography and TaxonomyTamásMártaNo ratings yet
- COVID Cluster Epi Curves 11052020Document1 pageCOVID Cluster Epi Curves 11052020Adrian MojicaNo ratings yet
- The Students' ProblemDocument21 pagesThe Students' ProblemAmairaNo ratings yet