Download as pdf or txt
You might also like
- YB2021 Executive SummaryDocument34 pagesYB2021 Executive SummaryValerie Strauss100% (2)
- My Pico PaperDocument6 pagesMy Pico Paperraddy109No ratings yet
- Advanced History TakingDocument15 pagesAdvanced History TakingErik DewantoNo ratings yet
- Adaptasi Masa NifasDocument28 pagesAdaptasi Masa NifasEliza HafniNo ratings yet
- BSM Bohol Research EditedDocument78 pagesBSM Bohol Research EditedBal Ri MekoleuNo ratings yet
- Konsep Gender & Ham Dalam Asuhan KebidananDocument15 pagesKonsep Gender & Ham Dalam Asuhan Kebidanantri yulianiNo ratings yet
- Adolescent PregnancyDocument60 pagesAdolescent PregnancyRafael CarrielNo ratings yet
- 92 Personal HygieneDocument9 pages92 Personal HygieneanisNo ratings yet
- Jurnal - Pendampingan Perencanaan Kehamilan SehatDocument6 pagesJurnal - Pendampingan Perencanaan Kehamilan SehatElly Naila Fauziah100% (1)
- 1280 2976 1 SMDocument15 pages1280 2976 1 SMNovita Lina100% (1)
- Efektivitas Penggunaan Buku Kia Dan Aplikasi Monsca Dalam Penerapan Standar Pelayanan Antenatal 14 TDocument6 pagesEfektivitas Penggunaan Buku Kia Dan Aplikasi Monsca Dalam Penerapan Standar Pelayanan Antenatal 14 TWaliya MursyidaNo ratings yet
- Konsep Askeb KomunitasDocument58 pagesKonsep Askeb Komunitassulthoni ikaNo ratings yet
- LP Speech DelayDocument16 pagesLP Speech DelayLina LinaNaNo ratings yet
- Format Dokumentasi Asuhan Kebidanan Pada Ibu Nifas: Data SubyektifDocument4 pagesFormat Dokumentasi Asuhan Kebidanan Pada Ibu Nifas: Data Subyektifsiti romlahNo ratings yet
- Evidance BasedDocument15 pagesEvidance BasedMelisa HutabaratNo ratings yet
- QUESTIONNAIREDocument3 pagesQUESTIONNAIREJohn Carl AparicioNo ratings yet
- Jurnal Komprehensif Pada NeonatusDocument14 pagesJurnal Komprehensif Pada Neonatusdesy sekarini100% (1)
- Chapter IDocument8 pagesChapter IMighty GooseNo ratings yet
- Breastfeeding Self EfficacyDocument18 pagesBreastfeeding Self EfficacyFitri Wahyuni PutriNo ratings yet
- Perbandingan Pemberian Ikan Gabus Dan Telur Ayam Terhadap Penyembuhan Luka Pasca Bedah Post Sectio CeasereaDocument11 pagesPerbandingan Pemberian Ikan Gabus Dan Telur Ayam Terhadap Penyembuhan Luka Pasca Bedah Post Sectio CeasereaSaskiyanto ManggabaraniNo ratings yet
- Clinical Learning Model in Professional Midwifery Education ProgramDocument59 pagesClinical Learning Model in Professional Midwifery Education ProgramHana NazeefaNo ratings yet
- Jurnal Kompres Bawang Merah Terhadap Bayi Demam Paska ImunisasiDocument12 pagesJurnal Kompres Bawang Merah Terhadap Bayi Demam Paska Imunisasiindah dwina putriNo ratings yet
- Grade 11 PR Proj. Teenage PregnancyDocument12 pagesGrade 11 PR Proj. Teenage PregnancyDairienne Mae MaiqueNo ratings yet
- Kemitraan Dukun Dengan Bidan Dalam Pertolongan PerDocument6 pagesKemitraan Dukun Dengan Bidan Dalam Pertolongan PerKiki TonaNo ratings yet
- Anemia2014 108593Document9 pagesAnemia2014 108593AaronMaroonFive100% (1)
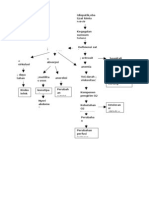
- Pathway AnemiaDocument1 pagePathway AnemiaRayn ChristNo ratings yet
- Teenage MommiesDocument6 pagesTeenage MommiesLeslie VillegasNo ratings yet
- Leaflet Senam HamilDocument2 pagesLeaflet Senam HamildianawatiNo ratings yet
- Role of Motivation in Academic Procrastination PDFDocument6 pagesRole of Motivation in Academic Procrastination PDFElonic AirosNo ratings yet
- Skripsi Tablet FeDocument7 pagesSkripsi Tablet FeYessiana Luthfia BahriNo ratings yet
- What Is AbortionDocument11 pagesWhat Is Abortionrumki99100% (1)
- Wafda Jurnal+bahasa+inggrisDocument9 pagesWafda Jurnal+bahasa+inggrisDesta Ayu Cahya RosyidaNo ratings yet
- Gangguan Siklus Menstruasi Akibat Aktivitas Fisik Dan KecemasanDocument12 pagesGangguan Siklus Menstruasi Akibat Aktivitas Fisik Dan KecemasanSri AstutiNo ratings yet
- Knowledge Behavior Attitude of Teenage Pregnant Women On Reproductive HealthDocument67 pagesKnowledge Behavior Attitude of Teenage Pregnant Women On Reproductive HealthJacklyn Pacible100% (1)
- MANUSKRIPDocument11 pagesMANUSKRIPandika saputraNo ratings yet
- Chapter-I 1.1 Context InformationDocument33 pagesChapter-I 1.1 Context InformationAshmi NeupaneNo ratings yet
- Makalah Askeb RentanDocument11 pagesMakalah Askeb RentanNovita Nur RasyidNo ratings yet
- Pengaruh Effleurage Massage Terhadap Nyeri Persali (1) - DikonversiDocument14 pagesPengaruh Effleurage Massage Terhadap Nyeri Persali (1) - DikonversiMihnati NatiNo ratings yet
- Safe Motherhood PDFDocument13 pagesSafe Motherhood PDFJoseph Kimaro100% (1)
- The Positive and Negative Effects of An Early Marriage Vs Marriage in Old AgeDocument2 pagesThe Positive and Negative Effects of An Early Marriage Vs Marriage in Old Agecintaksatria50% (4)
- RESUMEDocument4 pagesRESUMEJomari A. Cruz100% (1)
- Rangkuman Undang-UndangDocument59 pagesRangkuman Undang-UndangDidi HaryadiNo ratings yet
- Explaining Procedure and Giving InstructionDocument9 pagesExplaining Procedure and Giving InstructionErviaYonindaNo ratings yet
- Kesehatan Mental Masa PerinatalDocument37 pagesKesehatan Mental Masa PerinatalluxNo ratings yet
- Nurhasni - 2020 - HUBUNGAN MUTU PELAYANAN KESEHATAN DENGANDocument11 pagesNurhasni - 2020 - HUBUNGAN MUTU PELAYANAN KESEHATAN DENGANAswar AmiruddinNo ratings yet
- Perceptorship Mentorship Dian LestariDocument60 pagesPerceptorship Mentorship Dian LestariDiah Ayu lestariNo ratings yet
- Efektivitas Teknik Meneran Terhadap Pencegahan Ruptur Perineum Spontan Pada Ibu Bersalin Primigravida Di BPM SidoarjoDocument4 pagesEfektivitas Teknik Meneran Terhadap Pencegahan Ruptur Perineum Spontan Pada Ibu Bersalin Primigravida Di BPM SidoarjoAnggraini WuLandhariNo ratings yet
- Komunikasi Terapeutik: Ns. Suci Ratna Estria, M.KepDocument39 pagesKomunikasi Terapeutik: Ns. Suci Ratna Estria, M.KepKhusnul FatihaNo ratings yet
- 3 - Materi - Continuity of Midwifery CareDocument39 pages3 - Materi - Continuity of Midwifery CareRiani PutriNo ratings yet
- Asuhan Kebidanan Ibu Hamil Patologi, Andra DewiDocument13 pagesAsuhan Kebidanan Ibu Hamil Patologi, Andra DewiSilva RachmaNo ratings yet
- Case Study: Factors Affecting The Behavior of School Students in The Age of Pre-AdolescenceDocument9 pagesCase Study: Factors Affecting The Behavior of School Students in The Age of Pre-AdolescencePoonam KilaniyaNo ratings yet
- I. Growth and Development: Nature or Nurture?Document7 pagesI. Growth and Development: Nature or Nurture?rizzamae belenNo ratings yet
- Adolescence: An Age of Storm and Stress: Saba HashmiDocument15 pagesAdolescence: An Age of Storm and Stress: Saba HashmiVANDANA MISHRANo ratings yet
- SocioDocument3 pagesSocioGene Lloyd NacorNo ratings yet
- Child&AdolDocument4 pagesChild&AdolShelby OmanNo ratings yet
- BF4 AdolescenceVisits PDFDocument91 pagesBF4 AdolescenceVisits PDFhavidhasd100% (1)
- DebotuDocument3 pagesDebotuKobs ForeignerNo ratings yet
- A Hungarian-American Psychologist NamedDocument6 pagesA Hungarian-American Psychologist NamedMonique Clarivel Malalis LlamisNo ratings yet
- Ed 1 - Article FinalsDocument6 pagesEd 1 - Article FinalsMonique Clarivel Malalis LlamisNo ratings yet
- J.B Handayan - RRLDocument14 pagesJ.B Handayan - RRLRussel NagpacanNo ratings yet
- Who Is The Child and Adolescent LearnerDocument7 pagesWho Is The Child and Adolescent LearnerArJhay ObcianaNo ratings yet
- Lesson 1.2 The Formation of Heavier ElementsDocument5 pagesLesson 1.2 The Formation of Heavier ElementsMichaer AmingNo ratings yet
- Smadav 2020 Rev 138Document1 pageSmadav 2020 Rev 138Michaer AmingNo ratings yet
- WMSU-ISMP-GU-003.00: Effective Date: 7-DEC-2016Document3 pagesWMSU-ISMP-GU-003.00: Effective Date: 7-DEC-2016Michaer AmingNo ratings yet
- MIL-workbook-lesson-5 - 6-Understanding-Media-Aesthetics-of-New-Media (Recovered)Document4 pagesMIL-workbook-lesson-5 - 6-Understanding-Media-Aesthetics-of-New-Media (Recovered)Michaer AmingNo ratings yet
- Mining Right For A Sustainable FutureDocument1 pageMining Right For A Sustainable FutureMichaer AmingNo ratings yet
- Lesson 7 USCPDocument14 pagesLesson 7 USCPMichaer AmingNo ratings yet
- Lesson 7: Formation of Fossil Fuels: Earth & Life ScienceDocument8 pagesLesson 7: Formation of Fossil Fuels: Earth & Life ScienceMichaer AmingNo ratings yet
- Understanding Society, Culture and PoliticsDocument7 pagesUnderstanding Society, Culture and PoliticsMichaer AmingNo ratings yet
- Diass InfographicDocument1 pageDiass InfographicMichaer AmingNo ratings yet
- San Agustin Masterlist of Barangay and SK Officials 2023 1Document30 pagesSan Agustin Masterlist of Barangay and SK Officials 2023 1Barangay LusongNo ratings yet
- What Is Avoidant AttachmentDocument6 pagesWhat Is Avoidant AttachmentFannyKaruniaRamadhaniNo ratings yet
- JustineDocument2 pagesJustineNancy Dimapilis De SagunNo ratings yet
- Certificate: Internal External PrincipalDocument36 pagesCertificate: Internal External PrincipalNitesh kuraheNo ratings yet
- Smoke-Free Campus ProposalDocument6 pagesSmoke-Free Campus Proposalapi-360775870No ratings yet
- Program Coordinator (M-F) Nigeria SECOURS ISLAMIQUE FRANCE (SIF) Maiduguri NigeriaDocument3 pagesProgram Coordinator (M-F) Nigeria SECOURS ISLAMIQUE FRANCE (SIF) Maiduguri NigeriaMustapha Bello AdeoyeNo ratings yet
- Certification 4psDocument5 pagesCertification 4psJaneDandanNo ratings yet
- Cigarette Smoking Teens Published JNSRDocument10 pagesCigarette Smoking Teens Published JNSRJusil RayoNo ratings yet
- NURS 3055 Exam I InformationDocument1 pageNURS 3055 Exam I InformationCarrie DAndreaNo ratings yet
- 2013 Book HandbookOfCulturallyResponsiveDocument280 pages2013 Book HandbookOfCulturallyResponsiveStratos Mari100% (1)
- RiyaDocument1 pageRiyaArun KumarNo ratings yet
- Article1425026815 - Iwuchukwu Et Al.Document7 pagesArticle1425026815 - Iwuchukwu Et Al.i-Link Tech SolutionsNo ratings yet
- Kenya Youth Development Policy 2019Document127 pagesKenya Youth Development Policy 2019Norbert SiteyiNo ratings yet
- PA00W6T5Document48 pagesPA00W6T5jafariNo ratings yet
- 2013 - 14 RosterDocument2 pages2013 - 14 Rosterapi-233573146No ratings yet
- MODULE 12 Physical Development of Infants ToddlersDocument4 pagesMODULE 12 Physical Development of Infants ToddlersGillian Sanzinin GervacioNo ratings yet
- Early Childhood Development Iec Material DevelopmentDocument22 pagesEarly Childhood Development Iec Material DevelopmentNAMANYA ASA MUHOOZINo ratings yet
- Sexual I DadDocument8 pagesSexual I DadAql AqlNo ratings yet
- Adolescent HealthDocument36 pagesAdolescent HealthDeepak Samal100% (1)
- Conversation Questions TeenagersDocument3 pagesConversation Questions Teenagersjuan jnoseNo ratings yet
- Poised For Emerging Adulthood in Latin America: A Pleasure For The PrivilegedDocument6 pagesPoised For Emerging Adulthood in Latin America: A Pleasure For The PrivilegedCamiloPeñaNo ratings yet
- Hiv PREVENTIONDocument145 pagesHiv PREVENTIONThokala Sujatja100% (1)
- Full Report (Thinking Skills) (Final Project)Document30 pagesFull Report (Thinking Skills) (Final Project)irfancrummyNo ratings yet
- Research c3 FINALDocument36 pagesResearch c3 FINALLans HeheNo ratings yet
- Improving The Health, Safety, and Well-Being of Young AdultsDocument203 pagesImproving The Health, Safety, and Well-Being of Young AdultsYixi WangNo ratings yet
- Botswana NCD Strategy FinalDocument26 pagesBotswana NCD Strategy FinalDonaldinoNo ratings yet
- USAID Rwanda Youth Assessment - Public - 10-15-19Document49 pagesUSAID Rwanda Youth Assessment - Public - 10-15-19Estiphanos GetNo ratings yet
- 03 - Expectations and Resources in Different Context of Development - Towards Positive DevelopmentalDocument22 pages03 - Expectations and Resources in Different Context of Development - Towards Positive DevelopmentalRODESSA MAY CASTRONo ratings yet
- 2 Brief Inclusion Fact SheetDocument4 pages2 Brief Inclusion Fact Sheetapi-286077776No ratings yet