Professional Documents
Culture Documents
EPOC, Lancet 2015
EPOC, Lancet 2015
Uploaded by
Sebastian BurgosOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
EPOC, Lancet 2015
EPOC, Lancet 2015
Uploaded by
Sebastian BurgosCopyright:
Available Formats
Series
Chronic obstructive pulmonary disease 2
Current concepts in targeting chronic obstructive pulmonary
disease pharmacotherapy: making progress towards
personalised management
Prescott G Woodruff, Alvar Agusti, Nicolas Roche, Dave Singh, Fernando J Martinez
Chronic obstructive pulmonary disease (COPD) is a common, complex, and heterogeneous disorder that is Lancet 2015; 385: 1789–98
responsible for substantial and growing morbidity, mortality, and health-care expense worldwide. Of imperative See Editorial page 1697
importance to decipher the complexity of COPD is to identify groups of patients with similar clinical characteristics, This is the second in a Series of
prognosis, or therapeutic needs, the so-called clinical phenotypes. This strategy is logical for research but might be of two papers on chronic
obstructive pulmonary disease
little clinical value because clinical phenotypes can overlap in the same patient and the same clinical phenotype could
result from different biological mechanisms. With the goal to match assessment with treatment choices, the latest Division of Pulmonary, Critical
Care, Sleep and Allergy,
iteration of guidelines from the Global Initiative for Chronic Obstructive Lung Disease reorganised treatment Department of Medicine and
objectives into two categories: to improve symptoms (ie, dyspnoea and health status) and to decrease future risk (as Cardiovascular Research
predicted by forced expiratory volume in 1 s level and exacerbations history). This change thus moves treatment closer Institute, University of
to individualised medicine with available bronchodilators and anti-inflammatory drugs. Yet, future treatment options California, San Francisco, CA,
USA (Prof P G Woodruff MD);
are likely to include targeting endotypes that represent subtypes of patients defined by a distinct pathophysiological Thorax Institute, Hospital
mechanism. Specific biomarkers of these endotypes would be particularly useful in clinical practice, especially in Clinic, IDIBAPS, University of
patients in which clinical phenotype alone is insufficient to identify the underlying endotype. A few series of potential Barcelona, CIBERES, Barcelona,
Spain (Prof A Agusti MD);
COPD endotypes and biomarkers have been suggested. Empirical knowledge will be gained from proof-of-concept
Cochin Hospital Group,
trials in COPD with emerging drugs that target specific inflammatory pathways. In every instance, specific endotype Assistance Publique Hôpitaux
and biomarker efforts will probably be needed for the success of these trials, because the pathways are likely to be de Paris, University Paris
operative in only a subset of patients. Network analysis of human diseases offers the possibility to improve Descartes (EA2511), Paris,
France (Prof N Roche MD);
understanding of disease pathobiological complexity and to help with the development of new treatment alternatives
University of Manchester,
and, importantly, a reclassification of complex diseases. All these developments should pave the way towards University Hospital of South
personalised treatment of patients with COPD in the clinic. Manchester Foundations Trust,
Manchester, UK
(Prof D Singh MD); Weill
Introduction short-acting beta-2 agonists [SABA] and long-acting
Department of Medicine,
Chronic obstructive pulmonary disease (COPD) is a beta-2 agonists [LABA]), antimuscarinics (eg, short- New York-Presbyterian
common, complex, and heterogeneous condition that is acting antimuscarinic agent [SAMA] and long-acting Hospital/Weill Cornell Medical
responsible for substantial and growing morbidity, antimuscarinic agent [LAMA]), and inhaled College, New York, NY, USA
(Prof F J Martinez MD); and
mortality, and health-care expenses worldwide.1 In this corticosteroids. University of Michigan Health
context, complexity relates to many different components The Global Initiative for Chronic Obstructive Lung System, Ann Arbor, MI, USA
with non-linear dynamic interactions, whereas Disease (GOLD) was established in 1998 to improve (Prof F J Martinez)
heterogeneity implies that not all of these components the diagnosis, management, and prevention of COPD.
are present in all patients at any given timepoint or in the
same patient at different timepoints.2 To address this
complexity and heterogeneity, identification of groups of Search strategy and selection criteria
patients with similar clinical characteristics, prognosis or For this Series paper, we used several search approaches. We searched the Cochrane Library,
treatment needs (so-called clinical phenotypes), is Medline, and Embase using the search term “COPD” in combination with “clinical trial”,
imperative.3 On one hand, this strategy is logical for “effectiveness”, or “systematic review”, for 1 year between Jan 1, 2014 and Feb 28, 2015. For
research because it might create an increasingly the years preceding this search we used the bibliography cited in the Global Initiative for
homogeneous selection of patients in whom to decipher Chronic Obstructive Lung Disease (GOLD) document (GOLD search strategy used COPD,
the complexity of COPD. On the other hand, this strategy filters “human”, “all adult”, or “items” with “abstracts”, “clinical trial”, or “systematic review”).
might be of restricted clinical value because, first, clinical Additionally, we used the search terms “COPD”, “chronic obstructive pulmonary disease”,
phenotypes can overlap in the same patient and, second, “emphysema”, or “chronic bronchitis”, in combination with “LABA”, “LAMA”, “LABA/LAMA”,
the same clinical phenotype could result from different “ICS”, “ICS/LABA”, “COPD”, “chronic obstructive pulmonary disease”, “emphysema”, or
biological mechanisms (ie, aetiological heterogeneity). “chronic bronchitis” in combination with “endotype”, “molecular phenotype”, “biomarker-
Although the development of therapeutic approaches has directed”, “biomarker-driven”, or “targeted therapy”. Because some of these terms have only
increasingly attempted to address these complexities, so recently entered the medical vocabulary, we then searched for relevant references in the
far most treatment options belong to a restricted number bibliographies of selected articles.
of pharmacological classes—ie, bronchodilators (eg,
www.thelancet.com Vol 385 May 2, 2015 1789
Series
Correspondence to: A challenge for GOLD has since been to provide GOLD treatment propositions
Prof Fernando J Martinez, recommendations for the correct use of the available For all GOLD groups, short-acting bronchodilators are
Weill Department of Medicine,
Weill Cornell Medical College,
treatments and at the same time to flexibly position recommended for symptom relief. These drugs could be
New York-Presbyterian Hospital/ recommendations to allow the use of future innovative sufficient for patients in group A (of low risk and low
Weill Cornell Medical College, treatments that have the potential to target a personalised symptom burden). In patients who present more
New York, NY 10065, USA medicine approach. Another challenge faced by GOLD symptomatic limitations (GOLD B; of low risk but with
fjm2003@med.cornell.edu
and other guideline or strategy documents is the paucity increased symptom burden), long-acting bronchodilators
of evidence on how clinicians can identify patients who are recommended as maintenance treatment to decrease
are most likely to benefit from available COPD symptoms. Patients who are at an increased risk of
treatments. This difficulty underlines the need for new exacerbation (GOLD groups C [of high risk and low
treatment approaches in conjunction with refining of the symptom burden] and D [of high risk and increased
way treatment indications are established. Finally, in symptom burden]), the first choice of pharmacotherapy
most patients COPD is associated with other chronic includes inhaled corticosteroids and LABA combinations
diseases, a factor that should be addressed globally. This or LAMA, because both of these drug classes reduce
comorbidity might decrease the likelihood that exacerbation rates and improve lung function and health
treatments targeting only the COPD component will status.1 LABA and LAMA combinations are suggested as
change the natural history of a patient’s disease. an option for patients of GOLD groups B, C, and D because
This Series paper addresses the strengths and evidence showed that these drugs are more effective than
limitations, including gaps in the evidence, of the long-acting bronchodilator monotherapy is; although,
approaches taken to move treatment of COPD towards most of these studies were not designed to report effects
personalised medicine, and also addresses potential on exacerbations10 or were undertaken in patients who did
future approaches to position emerging treatments that not have a history of frequent exacerbations.11 Roflumilast,
will probably target specific biological pathways. As such, a phosphodiesterase-4 inhibitor, is positioned to prevent
we review the concept of an endotype, a subtype of a exacerbations in patients in GOLD groups C or D who
clinical disorder defined by a distinct pathophysiological have a chronic bronchitic phenotype, a novel example of
mechanism,4 because it could be associated with future phenotypically driven treatment.3,12
COPD treatments, and also review the role of biomarkers
in marking endotypes and directing treatment. Strengths and weaknesses of GOLD propositions
The overall concept to increase the close match between
Present treatment options the clinical assessment of an individual patient and
GOLD revolution specific treatment options is an appealing one and is a
The GOLD 20015 and 20066 reports used airflow limitation first step towards personalised therapy. For example,
alone (as assessed by the forced expiratory volume in 1 s patients with many symptoms (GOLD groups B and D)
[FEV1] value) to assess disease severity. Bronchodilators need more bronchodilators, whereas those patients
were recommended as treatments to improve lung at high risk (groups C and D) might need anti-
function and reduce symptoms in all patients, with inflammatory treatment. However, some treatment
inhaled corticosteroids reserved for patients with severe propositions from GOLD could be criticised for not
and very severe airflow limitation and repeated exacer- being strictly evidence-based,13 which is largely a result
bations. In 2011, the GOLD document acknowledged that of the paucity of evidence for treatment effects in
use of FEV1 alone to assess disease severity was an overly different subgroups of patients. For example, additional
simplistic approach,1 because FEV1 is often a poor studies are needed to investigate the effects of LABA
predictor of the extent of symptoms, health status and LAMA combinations in patients with a history
impairment, and risk of exacerbations.7 Treatment of exacerbations.14 Additionally, triple therapy (the
objectives were reorganised into two categories: relief of combination of inhaled corticosteroids and LABA plus
present symptoms and reduction in the risk of future LAMA) is a treatment option for patients in GOLD
adverse events to health. A well known system of group D and is frequently prescribed in clinical practice,
four-quadrant assessment characterises patients into but evidence for this regimen preventing exacerbations
broad phenotypic categories based on symptoms and risk is scarce.15 Patients in GOLD groups C and D are
of exacerbations (assessed by FEV1 and the history of heterogeneous with respect to their future risk,
exacerbations in the past year). The four-quadrant system depending on the way that they were assigned to one of
was introduced with the goal to match assessment with these categories (ie, low FEV1, history of exacerbations,
treatment choices, thus moving COPD treatment towards or both). Use of the inhaled corticosteroids and LABA
individualised medicine by matching the patient’s combination would logically thus be restricted to
treatment to their needs. This development was a major patients who have a history of exacerbations with or
step forward in the strategy for COPD management without severe airflow limitation, and long-acting
and other groups have proposed conceptually similar bronchodilators being preferred for those with low
approaches, but with several variations.8,9 FEV1 and no exacerbation history.16 Furthermore,
1790 www.thelancet.com Vol 385 May 2, 2015
Series
although results of the ECLIPSE study17 identified a history of exacerbations despite often being on inhaled
stable clinical phenotype of patients with 2 or more corticosteroids treatment (70% were taking inhaled
exacerbations every year (supporting GOLD’s threshold corticosteroids treatment at screening), and those who
to define patients at risk), inhaled corticosteroids and received triple-therapy during a run-in period before
LABA combinations have been studied mainly in being randomly assigned into either the inhaled
populations with an annual exacerbation rate nearer to corticosteroids withdrawal or control (inhaled cortico-
one per year; thus, the corresponding GOLD treatment steroids maintained) groups. In the withdrawal group,
position does not quite match the evidence generated the dose of fluticasone propionate was progressively
by clinical, randomised controlled trials (RCTs). No reduced (from 1000 μg/day, to 500 μg/day, and then to
therapeutic trial reported before the 2011 GOLD 200 μg/day) every 6 weeks before the drug was
document and only a few reported after this date did eventually stopped after 12 weeks. No difference in the
use selection criteria that strictly matched the present occurrence of exacerbations was reported between the
GOLD classification.18 two groups, but a difference was recorded between
groups of 40 mL loss of FEV1 during the 40 weeks after
Evidence from clinical trials: do they support, enrich, or complete drug withdrawal. Despite extensive subgroup
challenge treatment propositions? analyses27 the study did not identify patients at an
Use of inhaled corticosteroids in patients with COPD increased risk of withdrawal-associated exacerbations,
should mainly focus on prevention of exacerbations but of note is that the overall exacerbation rate in
because studies have shown inconsistent effects of both groups was quite low (about 0·5 exacerbations
these drugs on the rate of FEV1 decrease.19 Inhaled per patient per year), which probably made it difficult to
corticosteroids are generally used as part of fixed-dose detect a treatment difference in the context of a low rate
combinations with LABAs to maximise their clinical of events. As for many clinical trials, the WISDOM
benefits. Since the early 2000s,20 many clinical trials trial26 was not powered for such subgroup analysis.
assessing these fixed-dose combinations included Nevertheless, the loss of lung function after inhaled
patients with FEV1 of less than 50% predicted and a corticosteroids withdrawal, also reported by two other
history of exacerbations.21,22 By contrast, the TORCH previous studies,28,29 suggests some benefit for this type
study23 included patients with FEV1 of less than 60% of drug in these patients. Likewise, these results also
predicted (before administration of a bronchodilator) suggest that low doses of inhaled corticosteroids might
to study fluticasone propionate and salmeterol, and be sufficient in some patients to prevent exacerbations
patients with FEV1 of less than 70% predicted (after and to maintain lung function.
treatment with a bronchodilator) were included to study The question remains for when to use combination
the effects of the combination fluticasone furoate and treatments. Comparisons between inhaled corticosteroids
vilanterol.24 In both studies,23,24 these combinations of with LABA fixed-dose combinations and LAMAs did not
inhaled corticosteroids and LABA had a greater effect show any consistent difference in terms of exacerbation
than the use of LABA alone on exacerbation rates. This rate.30 Generally, combination treatments including
result suggests that for patients with a history of inhaled corticosteroids and LABA, LABA and LAMA, and
exacerbations, the extent of airflow limitation is not as inhaled corticosteroids with LABA plus LAMA were
important to predict benefit from inhaled corticosteroids. better than bronchodilator monotherapy treatments, at
Furthermore, combination of 25 μg vilanterol with least for some clinical endpoints.30–35 However, the scale
fluticasone furoate (an inhaled corticosteroid) at doses of the overall difference between combination treatments
of 50 μg, 100 μg, and 200 μg was studied, addressing for and monotherapy is often small and less than the
the first time the scarcity of evidence on dose-response expected additive effect of the components in the
associations for long-term effects of inhaled cortico- combinations. Furthermore, most studies of LABA and
steroids.24 The dose-response curve was quite flat in LAMA combination inhalers included patients that
terms of exacerbations, suggesting that high doses of were previously treated with at least one long-acting
inhaled corticosteroids are not needed to achieve an bronchodilator monotherapy. Thus, to restrict the use of
optimum benefit in COPD. However, of note is that the combination treatments seems logical for patients with
number of side-effects of interest (ie, pneumonia and dyspnoea or persisting exacerbations despite previous
bone fractures) was not decreased at lower dosages of long-acting bronchodilator monotherapy. GOLD does
these drugs. not include such a step-by-step approach in its
In 2011, a systematic review25 concluded that inhaled recommendations, but this could be what many
corticosteroids withdrawal was not associated with clinicians expect from therapeutic guidance, provided
important deterioration in overall patient outcomes, but that the rules and criteria to guide choices are simple
that this result could be affected by the definition of enough and evidence-based. Combination of precision
exacerbations and concomitant treatments. In 2014, and simplicity, as a prerequisite for successful guidelines’
results of the WISDOM trial were reported.26 This RCT26 implementation, is a major challenge for personalised
included patients with severe airflow limitation and a medicine.36
www.thelancet.com Vol 385 May 2, 2015 1791
Series
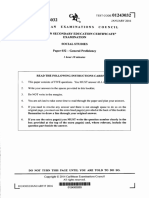
Individual presentation and Individual risk factors and
characteristics.43–46 With respect to inhaled corticosteroids,
underlying mechanisms comorbidities growing concerns about these drugs are associated with
• Mortality • Pneumonia the risk of pneumonia and systemic side-effects.47 Yet,
• Disease progression • Tuberculosis these risks should be balanced with an apparent reduction
• Lung function • Skin bruising
• Symptoms: • Osteoporosis or fractures of a composite outcome of death and admissions to
cough, Individualisation of • Muscle dysfunction hospital for COPD, as described in patients who received
sputum production, and treatment choices in COPD • Nutritional impairment
dyspnoea • Cataract
LABA and inhaled corticosteroids compared with those
• Excercise tolerance • Diabetes given LABA alone.48 However, as these data are from an
• Exacerbations • Tremour observational database study they warrant further
• Disability • Cardiovascular events
• Health status and quality • Neuropsychological effects confirmation.
of life • Gastrointestinal symptoms
Expected benefits
Present COPD pharmacological
Expected risks
Identification of responders or patients at increased risk
treatments of side-effects
Although some patient characteristics clearly affect
LABA; treatment choice for invasive approaches, such as
LAMA; surgery for lung volume reduction,49 most large trials
LABA + LAMA;
LABA + ICS; investigating COPD pharmacological treatments have
LABA + LAMA + ICS; not clearly identified predictors of responders or non-
LABA + roflumilast;
LAMA + roflumilast responders, or patients at increased risk of side-effects.
Importantly, the common way to analyse data from
Figure 1: Benefit–risk balance and its individual determinants with personalised COPD treatment choices clinical RCTs is to compare mean effects between
When a clinician is deciding which pharmacological treatment options to prescribe to a patient, they have to treatment arms, which could miss a patient who goes in
consider expected benefits (determined by individual presentation and underlying mechanisms of disease) and
possible risks (which depend on individual risk factors and comorbidities). COPD=chronic obstructive pulmonary
a direction opposite to most participants. An example of
disease. LABA=long-acting beta-2 agonists. LAMA=long-acting antimuscarinic agents. ICS=inhaled corticosteroids. this is the identification of a subgroup of patients with
COPD and persistent systemic inflammation by
Future treatment directions network analysis that was not identified by use of the
Disappointingly, the overall scale of clinical benefit of the comparison between conventional group means.50
different pharmacological treatment options in patients Furthermore, most RCTs do not fully represent real-life
with COPD is somewhat restricted. Although populations and contexts,51 and sample sizes are too
symptomatic benefits and reductions in exacerbation small for extensive and powerful subgroup analyses.
frequency can be achieved with available treatments, An exception is roflumilast, which was shown to
effects on the decrease of lung function and mortality in be especially effective when used with long-acting
long-term studies have been disappointing.23,37 This poor bronchodilators in patients with symptoms of chronic
effect can be at least partly accounted for by the presence bronchitis, FEV1 less than 50% predicted, and a history
of some extent of irreversible morphological of exacerbations.52 Similarly, azithromycin was most
abnormalities, including emphysema and loss of small effective at reducing exacerbations in older patients
airways.38 Various inflammatory mechanisms involved in (aged >65 years) with mild disease who have stopped
COPD do not respond well to corticosteroids, thus also smoking.53 In terms of side-effects, a greater increase in
restricting treatment effects.39 Furthermore, the response the risk of pneumonia related to inhaled corticosteroids
to corticosteroids seems to differ based on inflammatory was found in current smokers, and patients with prior
cells present—eg, the presence of eosinophils suggests pneumonia, body-mass index less than 25 kg/m² and
the increased likelihood of response to corticosteroids.40 severe airflow limitation.54 Beyond intrinsic patient
Because morphological changes and biological features characteristics, environmental factors could also affect
are substantially heterogeneous in people with COPD,41,42 the benefit–risk ratio of inhaled corticosteroids, as was
the sensitivity to pharmacological treatments will vary suggested55 for the inhaled corticosteroids-associated
between patients. These observations suggest that risk of tuberculosis, which is increased in countries
individualising available treatments based on increasing with a high prevalence of tuberculosis.
in-depth individual characterisation of pathophysiology Additional progress in the identification of specific
might optimise effectiveness; and, development of new characteristics associated with response or adverse effects
treatments that target specific mechanisms involved in from treatment can be provided by several approaches:
subgroups of patients might be an effective strategy. post-hoc exploratory analyses of available treatment trials;
Additionally, we need to use a benefit–risk approach for observational cohort studies (retrospective [eg, with
treatments36 rather than an approach purely based on databases] or prospective), especially with a comparative
effectiveness (figure 1). For long-acting bronchodilators, effectiveness design; pragmatic RCTs; novel analytical
the risk of cardiovascular events has been the topic of strategies, such as cluster and network analysis;51 and,
several studies with, somehow, contradictory results large, long term, classic RCTs. All these studies should
depending on study designs and population be undertaken in carefully selected and extensively
1792 www.thelancet.com Vol 385 May 2, 2015
Series
characterised patients. In addition to precise clinical
Symptom
characterisation (including physiology and imaging), Clinical phenotype
driven Tx
biomarkers will most likely be of major interest to both
identify target patients and assess treatment effects. In Endotype
Biomarker-
view of the complex associations between different directed Tx
biological levels (eg, genomics, epigenetics, proteomics,
metabolomics, cell physiology, inflammation, and repair
Risk factors
mechanisms), their identification of these associations (or avoidance Exposome Genome
interactions) is likely to come from multilevel, dynamic
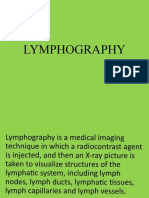
network analyses.50,56 In fact, studies of gene signatures Figure 2: Interrelations between exposome, genome, endotype, and clinical
that used this analytical approach have already generated phenotype of COPD
Diagram of the interrelations (thin black arrows) between the exposome (the
hypotheses regarding mechanisms and predictors of totality of human environmental exposures, from conception onwards60),
steroid response independent of the clinical phenotype.57,58 genome (the genetic background of the individual), the endotype (biological
All these avenues of research were emphasised in an networks that enable and restrict reactions), and the clinical phenotype (final
American Thoracic Society and European Respiratory clinical expression of the disease; eg, symptoms, exacerbations, response to
treatment, rate of disease progression, or death). Large arrows represent
Society statement about research questions in COPD.59 different treatment strategies. COPD=chronic obstructive pulmonary disease.
Tx=treatment.
Potential effect of endotyping and biomarker-
directed approaches to future treatment that they are worthy of further investigation as potential
decisions endotypes. Three of the potential endotypes of COPD we
COPD endotypes refer to are based on markers of inflammation or airway
As previously discussed, an endotype4 is a subtype of a colonisation with pathogenic bacteria. Both of these
clinical disorder defined by a distinct pathophysiological processes can contribute to disease progression in
mechanism, whereas a clinical phenotype3 is a single patients with COPD through persistent activation of the
or combination of disease attributes that describe immune response (eg, neutrophil inflammation in
differences between individuals with COPD as they response to bacterial colonisation), production of factors
relate to clinically meaningful outcomes (ie, symptoms, that injure lung cells or the extracellular matrix (eg,
exacerbations, response to treatment, rate of disease neutrophil elastase), structural changes that result from
progression, or death; figure 2). In the past decade, cellular and extracellular matrix injury (eg, emphysema),
studies aiming to identify and characterise sub- and physiological dysfunction that is recognised as
populations of patients with COPD were directed at COPD (eg, loss of elastic recoil and resulting airflow
clinical phenotyping. By use of various statistical obstruction; figure 3).
techniques to explore cohorts and link cross-sectional
characteristics together with longitudinal outcomes, α-1 antitrypsin (α1AT) deficiency
some phenotypes have been reproducibly identified, α-1 antitrypsin (α1AT) deficiency meets all of the criteria
including patients with metabolic and cardiovascular for an endotype of COPD. It has known genetic under-
comorbidities, patients with severe airflow limitation pinnings, distinct clinical characteristics, characteristic
that occurred with an onset when aged 40–45 years,61 histopathology, distinct epidemiology, and a mechanism-
frequent exacerbators, and patients with predominant directed treatment approach that is guided by biomarkers
emphysema versus predominant airways disease.62,63 (such as serum α1AT concentration, α1AT protein
Some, but not all, of these phenotypes have been phenotyping, and α1AT genotyping).64 However, α1AT
associated with specific biological mechanisms deficiency is a quite unique endotype of COPD in that it is
(eg, endotypes), whereas many can actually correspond a Mendelian disorder. Other endotypes of COPD, as they
with several endotypes (eg, frequent exacerbators or are identified, are likely to be complex diseases in which
patients with cardiovascular comorbidities). As noted predispositions are dependent on several genes and
previously, linking of endotypes to clinical phenotypes developmental and environmental effects are prominent.
and to endotype-specific biomarkers will be crucial
because phenotypes and biomarkers are more accessible Persistent systemic inflammation
to clinicians than endotypes are. Therefore, formal A subgroup of patients with COPD has persistently
identification of an endotype implies the recognition of raised concentrations of inflammatory biomarkers in the
several shared features including clinical characteristics, blood (including the white blood cell count, C-reactive
biomarkers, physiology, genetics, histopathology, epi- protein, interleukin 6, and fibrinogen) and this group has
demiology, and treatment response.4 A well recognised significantly increased all-cause mortality and
subset of COPD is α-1 antitrypsin deficiency, which exacerbation frequency.65 However, whether this
already meets all criteria for an endotype. Although persistent systemic inflammation can be treated
other potential COPD endotypes that we identify in this pharmacologically and which biomarkers would be most
Series paper only partly fulfil these criteria, we believe relevant to target with specific treatments, is not yet clear.
www.thelancet.com Vol 385 May 2, 2015 1793
Series
asthma COPD overlap syndrome that might be useful to
Endotypes Exposome Biomarker- distinguish between the effects of Th2 cytokines and
• COPD with persistent directed
systemic inflamation personalised
could point to blood biomarkers that might be clinically
• eosinophilic or Th2 medicines useful in addition to or as an alternative to eosinophilia.
high COPD Inflammation approaches
(variable) Endotype
Biomarker- • α-1 antitrypsin Bacterial colonisation
directed
personalised
Infection deficiency Bacterial colonisation is common in COPD, is thought to
(variable)
medicines Cellular and matrix changes drive inflammation and risk for exacerbation,73 and
approaches Extracellular matrix destruction; characterises an important subset of patients with stable
abnormal cell repair or apoptosis; Genetics
Endotype ciliary dysfunction, mucus COPD. Thus COPD with bacterial colonisation represents
• COPD with persistent a clinical phenotype and, so far as this colonisation
pathogenic bacterial
colonisation Structural changes contributes to the biological mechanisms that perpetuate
Airways remodelling; alveolar destruction
COPD, it could be regarded as an endotype. A new
therapy that reduces the risk for exacerbation in COPD is
Physiological dysfunction
Clinical manifestations of COPD with an antibiotic azithromycin.53,74 Whether this benefit
is due to the antibacterial effect of azithromycin on
Figure 3: Present understanding of potential COPD endotypes
bacterial colonisation or more from direct anti-
Shown in black are the relations between inflammation, cellular changes, structural changes, and physiological
dysfunction in COPD, and the role that chronic infection can have in perpetuating inflammation. In red are inflammatory effects is uncertain, but biomarkers of
potential endotypes of COPD that relate to subtypes of inflammation, the presence of pathogenic bacterial bacterial colonisation in COPD could be valuable to target
colonisation, and the absence of a mechanism to protect against extracellular matrix destruction (α-1 antitrypsin azithromycin or other emerging antibacterial approaches.
deficiency). COPD=chronic obstructive pulmonary disease. Th2=T-helper-2 cell.
Although procalcitonin has been mostly assessed as a
marker of bacterial infection rather than colonisation,75,76
Raised eosinophil or T-helper-2 cell concentrations the electric nose (E-nose) is a method that measures
Patients with COPD who have raised sputum volatile organic compounds in exhaled breath and could
or blood eosinophils or inflammation associated with help to identify patients colonised with bacteria.77 This
T-helper-2 (Th2) cells might constitute an endotype of beneficial reduction in risk for exacerbation of
this disease. Accumulating evidence shows that this azithromycin is accompanied by a reduction in plasma
subgroup of patients with COPD who have sputum or concentrations of soluble tumour necrosis factor receptor 2,
blood eosinophilia might respond to corticosteroids and which suggests a possible surrogate outcome measure.78
possibly to blockers of cytokines produced by Th2 cells.66 Overall, because different bacteria can elicit different host
For example, the presence of raised sputum eosinophils responses,79–81 the optimum endotype of COPD based on
in patients with stable COPD was associated with bacterial colonisation could depend on methods that are
improvement in symptoms, post-bronchodilator FEV1, specific for pathogenic species.
and shuttle walk (a test of functional capacity) in a
crossover, randomised trial of systemic corticosteroids.67 Biological subtypes of COPD endotypes
Another study67 accorded with this result that sputum Exacerbations of COPD are associated with a clinically-
eosinophilia predicts benefit with systemic relevant negative effect in both the short term (ie,
corticosteroids, and other studies68–70 showed that this morbidity, mortality, and increased cost of treatment)
predictive association extends to inhaled corticosteroids and the long term (ie, by accelerating decrease in lung
too. Thus, sputum eosinophils are a biomarker that function).82,83 Optimised strategies to prevent and treat
could be useful in future decisions relevant to the exacerbations better are therefore an important medical
targeted use of inhaled corticosteroid in COPD. Blood need. To maximise the benefit of corticosteroids and
eosinophils could possibly be a useful surrogate for antibiotics in COPD exacerbations, and to develop new
sputum eosinophils. Persistent blood eosinophilia (>2%) therapeutic alternatives, it would be valuable to have
was present in 37% of participants with COPD in the biomarkers that identify subtypes of exacerbations that
ECLIPSE study.71 Additionally, post-hoc analyses from the respond to specific therapies. Bafadhel and colleagues84
2014 reported randomised trial72 of benralizumab (an in 2011 described four subtypes of exacerbations
anti-interleukin-5-receptor α monoclonal antibody) in (bacterial, viral, eosinophilic, and pauci-inflammatory)
patients with COPD and sputum eosinophilia, suggested defined by distinct biomarker profiles (sputum
a response in a subgroup with raised concentrations of interleukin 1β, serum CXCL10, and blood eosinophils,
blood eosinophils (defined as either ≥200 cells per μL or respectively), which they postulated to represent distinct
≥300 cells per μL). As in asthma, several Th2 cytokines underlying biology. Randomised trial data85 and a meta-
could drive inflammation in eosinophilic or Th2 high analysis86 suggest that blood eosinophil levels could be
COPD. Since these Th2 cytokines (interleukin 5, 4, and used to target use of oral corticosteroids for the acute
13) are difficult to measure directly, specific biomarkers treatment of COPD exacerbations. Other data suggest
of these cytokines could be valuable. In 2015, Christenson that procalcitonin and C-reactive protein could be used to
and colleagues57 identified molecular biomarkers of the guide antibiotic use.76,87
1794 www.thelancet.com Vol 385 May 2, 2015
Series
Comorbidities could be argued to be of sufficient magnitude amount to
Comorbidities such as cardiovascular disease or make them clinically relevant. Another important future
sarcopenia (muscle wasting) are prevalent in patients direction is the longitudinal study of biomarker-defined
with COPD and negatively affect its clinical course and subgroups to improve understanding of the stability of
prognosis.88 Yet, not all patients with COPD have them or, these subgroupings. Finally, of importance is to consider
if they do, present the same pattern. Analyses published that the subgroups of patients with COPD defined by
in the past year89,90 suggest that specific comorbidities these groupings who might themselves be extremely
share molecular pathways and might constitute shared complex and include non-linear dynamic interactions
treatment targets. Therefore, efforts to understand the mediated by biological networks that enable, filter,
biology of clinical phenotypes of COPD characterised by condition, and buffer them.97 Systems biology and
specific constellations of comorbidities could lead to the network medicine offer an integrative, multilevel, and
identification of specific endotypes of COPD characterised dynamic approach to understand and eventually lead to
by specific biomarkers and treatment responses. treatment changes of these complex molecular,
functional, clinical, and environmental networks,50,98,99 a
Lung cancer strategy that studies42,100,101 published in the past year have
Lung cancer is highly prevalent in patients with COPD used. Network analysis of human diseases not only offers
and is one of the main causes of death in this the possibility of a better understanding of pathobiological
population, especially in those patients with mild to complexity of different disease subtypes (endotypes), but
moderate airflow limitation.91 Smoking is the main risk also helps with the development of new therapeutic
factor for both COPD and lung cancer, but not all alternatives and, importantly, a reclassification of complex
smokers develop either of these diseases.1,92 Yet, people diseases.36,102,103 In essence, all these developments should
who develop COPD, particularly if emphysema is pave the way towards personalised medicine, also known
present, have a much higher risk of developing lung as P4 medicine or precision medicine.2,104,105 In this context,
cancer than those without COPD,93,94 suggesting a the precision medicine initiative106 launched by the
synergistic effect between COPD (and emphysema) and US president Barack Obama on Jan 20, 2015, suggests
lung cancer. Molecular mechanisms linking COPD how to progress towards better health. In the meantime,
with lung cancer are unclear, but accumulating the concept of a so-called control panel for COPD107 that
evidence suggests that the chronic inflammatory identifies treatable clinical traits could represent an
response that characterises COPD is likely to have a key appropriate way forward to the implementation of an
pathogenic role.95 Improvements in understanding of increasingly personalised treatment of COPD in
the complex molecular networks that characterise such the clinic.2
response is essential to design effective chemopreventive Contributors
and immune-treatment strategies. All authors contributed equally in writing the first version and the
revisions of this Series paper.
Conclusions and future directions Declaration of interests
We will gain empiric knowledge from proof-of-concept PGW has received a grant from Genentech to study interleukin 13 in
asthma. PGW has received personal fees for being on the advisory board
trials in COPD with emerging drugs that target specific for Genentech, Johnson and Johnson, and Neostem, and received
inflammatory pathways (eg, monoclonal antibodies personal fees for being a consultant for Roche, AstraZeneca, and
against interleukins 4, 5, 6, 13, 17, and 1β).96 Yet, at least Novartis, all outside the submitted work. PGW has a pending patent
two reasons exist for caution as these clinical trials are (12/935822) for compositions and methods for treating and diagnosing
asthma. PGW is supported by grants from the National Institute of
approached. First, a given endotype might possibly be Health (HL126493, HL107202, AI077439, HL114447, and SPIROMICS
relevant for only a small subset of the population with contract HHSN268200900014C). DS has received grants and personal
this disease. If so, these trials will have to consider either fees from Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi,
enrolment of only people who are likely to respond to the GlaxoSmithKline (GSK), Glenmark, Johnson and Johnson, Merck,
NAPP, Novartis, Pfizer, Takeda, Teva, Therevance, and Verona, outside
treatment based on a specific biomarker, or enrolment of the submitted work. DS has received personal fees from Genentech and
all people with COPD and stratification of participants Skyepharma, outside the submitted work. FJM has received grants from
based on concentrations of biomarkers. This second National Heart, Lung, and Blood Institute for studies into chronic
approach, has the advantage of allowing for assessment obstructive pulmonary disease. FJM has received personal fees from
Actelion, American College of Chest Physicians, Amgen, AstraZeneca,
of response in the biomarker negative group. Second, an Bayer, Boehringer Ingelheim, Carden Jennings, CME Incite, Center for
endotype or biomarker-directed treatment could be weak Healthcare Education, CSA Medical, Forest, Genentech, Grey Healthcare,
if it were to target a pathway that represents only one of GSK, Ikaria, Informa, Inova Health System, Janssens, MedScape, Merck,
Merion, Miller Medical, National Association for Continuing Education,
several contributing pathways to COPD in a patient.
Nycomed/Takeda, Paradigm, Peer Voice, Pearl, Pfizer, Projects in
However, from experience in other respiratory diseases, Knowledge, St John’s Hospital (Livonia, MI, USA), St Mary’s Hospital
such as lung cancer (epidermal growth factor receptor), (Detroit, MI, USA), Sudler and Hennessey, Roche, University of Illinois
asthma (Th2 high, based on periostin), and even in COPD (Chicago, USA), University of Virginia (Virginia, USA), UpToDate,
Wayne State University (Detroit, USA), and Western Society of Allergy
(steroids for eosinophilic COPD and augmentation
and Clinical Immunology, all outside the submitted work. NR has
therapy for α1AT), the benefits of targeted treatment
www.thelancet.com Vol 385 May 2, 2015 1795
Series
received grants from Boehringer Ingelheim, Novartis, and Pfizer. NR has 18 Rossi A, van der Molen T, del Olmo R, et al. INSTEAD: a randomised
received personal fees from Boehringer Ingelheim, Novartis, Pfizer, Teva, switch trial of indacaterol versus salmeterol/fluticasone in moderate
GSK, AstraZeneca, Chiesi, Mundipharma, Almirall, Aerocrine, COPD. Eur Respir J 2014; 44: 1548–56.
Stallergenes, and Merck Sharp & Dohme (MSD). AA has received grants 19 Yang IA, Clarke MS, Sim EH, Fong KM. Inhaled corticosteroids for
from Almirall, GSK, MSD, AstraZeneca, Menarini, Instituto de Salud stable chronic obstructive pulmonary disease.
Carlos III (PI12/01117), Recercaixa-2012 (AA084096), SEPAR (PI065/2013, Cochrane Database Syst Rev 2012; 7: CD002991.
PI192/2012), and FUCAP 2012, outside the submitted work. AA has 20 Burge PS, Calverley PM, Jones PW, Spencer S, Anderson JA,
received personal fees from Almirall, GSK, Teva, Novartis, AstraZeneca, Maslen TK. Randomised, double blind, placebo controlled study of
and Menarini, outside the submitted work. fluticasone propionate in patients with moderate to severe chronic
obstructive pulmonary disease: the ISOLDE trial. BMJ 2000;
References 320: 1297–303.
1 Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, 21 Wedzicha JA, Singh D, Vestbo J, et al, and the FORWARD
management, and prevention of chronic obstructive pulmonary Investigators. Extrafine beclomethasone/formoterol in severe
disease: GOLD executive summary. Am J Respir Crit Care Med 2013; COPD patients with history of exacerbations. Respir Med 2014;
187: 347–65. 108: 1153–62.
2 Agusti A. The path to personalised medicine in COPD. Thorax 22 Szafranski W, Cukier A, Ramirez A, et al. Efficacy and safety of
2014; 69: 857–64. budesonide/formoterol in the management of chronic obstructive
3 Han MK, Agusti A, Calverley PM, et al. Chronic obstructive pulmonary disease. Eur Respir J 2003; 21: 74–81.
pulmonary disease phenotypes: the future of COPD. 23 Calverley PM, Anderson JA, Celli B, et al, and the TORCH
Am J Respir Crit Care Med 2010; 182: 598–604. investigators. Salmeterol and fluticasone propionate and survival in
4 Lötvall J, Akdis CA, Bacharier LB, et al. Asthma endotypes: a new chronic obstructive pulmonary disease. N Engl J Med 2007;
approach to classification of disease entities within the asthma 356: 775–89.
syndrome. J Allergy Clin Immunol 2011; 127: 355–60. 24 Dransfield MT, Bourbeau J, Jones PW, et al. Once-daily inhaled
5 Global Initiative for Chronic Obstructive Lung Disease. Global fluticasone furoate and vilanterol versus vilanterol only for
strategy for diagnosis, management, and prevention of chronic prevention of exacerbations of COPD: two replicate double-blind,
obstructive pulmonary disease NHLBI/WHO workshop. 2001. parallel-group, randomised controlled trials. Lancet Respir Med 2013;
http://www.goldcopd.org/uploads/users/files/GOLDWkshp2001. 1: 210–23.
pdf (accessed April 14, 2015). 25 Nadeem NJ, Taylor SJ, Eldridge SM. Withdrawal of inhaled
6 Global Initiative for Chronic Obstructive Lung Disease. Global strategy corticosteroids in individuals with COPD—a systematic review and
for diagnosis, management, and prevention of chronic obstructive comment on trial methodology. Respir Res 2011; 12: 107.
pulmonary disease. 2006. http://www.goldcopd.org/uploads/users/ 26 Magnussen H, Disse B, Rodriguez-Roisin R, et al, and the
files/GOLDReport2006_0122.pdf (accessed April 14, 2015). WISDOM Investigators. Withdrawal of inhaled glucocorticoids and
7 Agusti A, Calverley PM, Celli B, et al, and the Evaluation of COPD exacerbations of COPD. N Engl J Med 2014; 371: 1285–94.
Longitudinally to Identify Predictive Surrogate Endpoints 27 Magnussen H, Tetzlaff K, Calverley PM. Inhaled glucocorticoids
(ECLIPSE) investigators. Characterisation of COPD heterogeneity and COPD exacerbations. N Engl J Med 2015; 372: 93–94.
in the ECLIPSE cohort. Respir Res 2010; 11: 122. 28 van der Valk P, Monninkhof E, van der Palen J, Zielhuis G,
8 Miravitlles M, Soler-Cataluña JJ, Calle M, et al. A new approach to van Herwaarden C. Effect of discontinuation of inhaled
grading and treating COPD based on clinical phenotypes: summary corticosteroids in patients with chronic obstructive pulmonary
of the Spanish COPD guidelines (GesEPOC). Prim Care Respir J disease: the COPE study. Am J Respir Crit Care Med 2002;
2013; 22: 117–21. 166: 1358–63.
9 Koblizek V, Chlumsky J, Zindr V, et al, and the Czech 29 Wouters EF, Postma DS, Fokkens B, et al, and the COSMIC (COPD
Pneumological and Phthisiological Society. Chronic Obstructive and Seretide: a Multi-Center Intervention and Characterization)
Pulmonary Disease: official diagnosis and treatment guidelines of Study Group. Withdrawal of fluticasone propionate from combined
the Czech Pneumological and Phthisiological Society; a novel salmeterol/fluticasone treatment in patients with COPD causes
phenotypic approach to COPD with patient-oriented care. immediate and sustained disease deterioration: a randomised
Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2013; controlled trial. Thorax 2005; 60: 480–87.
157: 189–201. 30 Welsh EJ, Cates CJ, Poole P. Combination inhaled steroid and
10 Tashkin DP, Pearle J, Iezzoni D, Varghese ST. Formoterol and long-acting beta2-agonist versus tiotropium for chronic
tiotropium compared with tiotropium alone for treatment of COPD. obstructive pulmonary disease. Cochrane Database Syst Rev 2013;
COPD 2009; 6: 17–25. 5: CD007891.
11 Vogelmeier CF, Bateman ED, Pallante J, et al. Efficacy and safety of 31 Aaron SD, Vandemheen KL, Fergusson D, et al, and the Canadian
once-daily QVA149 compared with twice-daily salmeterol- Thoracic Society/Canadian Respiratory Clinical Research
fluticasone in patients with chronic obstructive pulmonary disease Consortium. Tiotropium in combination with placebo, salmeterol, or
(ILLUMINATE): a randomised, double-blind, parallel group study. fluticasone-salmeterol for treatment of chronic obstructive pulmonary
Lancet Respir Med 2013; 1: 51–60. disease: a randomized trial. Ann Intern Med 2007; 146: 545–55.
12 Martinez FJ, Calverley PMA, Goehring U-M, Brose M, Fabbri LM, 32 Wedzicha JA, Calverley PM, Seemungal TA, Hagan G, Ansari Z,
Rabe KF. Effect of roflumilast on exacerbations in patients with Stockley RA, and the INSPIRE Investigators. The prevention of
severe chronic obstructive pulmonary disease uncontrolled by chronic obstructive pulmonary disease exacerbations by salmeterol/
combination therapy (REACT): a multicentre randomised fluticasone propionate or tiotropium bromide.
controlled trial. Lancet 2015; 385: 857–66. Am J Respir Crit Care Med 2008; 177: 19–26.
13 Lin FJ, Lee TA, Wong PS, Pickard AS. Evaluation of changes in 33 Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and
guidelines for medication management of stable chronic long-acting beta(2)-agonist in one inhaler versus long-acting
obstructive pulmonary disease. J Eval Clin Pract 2013; 19: 953–60. beta(2)-agonists for chronic obstructive pulmonary disease.
14 Frampton JE. QVA149 (indacaterol/glycopyrronium fixed-dose Cochrane Database Syst Rev 2012; 9: CD006829.
combination): a review of its use in patients with chronic 34 Nannini LJ, Poole P, Milan SJ, Kesterton A. Combined
obstructive pulmonary disease. Drugs 2014; 74: 465–88. corticosteroid and long-acting beta(2)-agonist in one inhaler versus
15 Karner C, Cates CJ. Combination inhaled steroid and long-acting inhaled corticosteroids alone for chronic obstructive pulmonary
beta(2)-agonist in addition to tiotropium versus tiotropium or disease. Cochrane Database Syst Rev 2013; 8: CD006826.
combination alone for chronic obstructive pulmonary disease. 35 Kew KM, Dias S, Cates CJ. Long-acting inhaled therapy
Cochrane Database Syst Rev 2011; 3: CD008532. (beta-agonists, anticholinergics and steroids) for COPD: a network
16 Agusti A, Fabbri LM. Inhaled steroids in COPD: when should they meta-analysis. Cochrane Database Syst Rev 2014; 3: CD010844.
be used? Lancet Respir Med 2014; 2: 869–71. 36 Agustí A, Antó JM, Auffray C, et al. Personalized Respiratory
17 Hurst JR, Vestbo J, Anzueto A, et al, and the Evaluation of COPD Medicine: Exploring the Horizon, Addressing the Issues. Summary
Longitudinally to Identify Predictive Surrogate Endpoints of a BRN-AJRCCM Workshop Held in Barcelona on June 12, 2014.
(ECLIPSE) Investigators. Susceptibility to exacerbation in chronic Am J Respir Crit Care Med 2015; 191: 391–401.
obstructive pulmonary disease. N Engl J Med 2010; 363: 1128–38.
1796 www.thelancet.com Vol 385 May 2, 2015
Series
37 Tashkin DP, Celli B, Senn S, et al, and the UPLIFT Study 59 Celli BR, Decramer M, Wedzicha JA, et al, ATS/ERS Task Force for
Investigators. A 4-year trial of tiotropium in chronic obstructive COPD Research. An official American Thoracic Society/European
pulmonary disease. N Engl J Med 2008; 359: 1543–54. Respiratory Society statement: research questions in chronic
38 McDonough JE, Yuan R, Suzuki M, et al. Small-airway obstruction obstructive pulmonary disease. Am J Respir Crit Care Med 2015;
and emphysema in chronic obstructive pulmonary disease. 191: e4–e27.
N Engl J Med 2011; 365: 1567–75. 60 Vrijheid M. The exposome: a new paradigm to study the impact of
39 Barnes PJ, Adcock IM. Glucocorticoid resistance in inflammatory environment on health. Thorax 2014; 69: 876–78.
diseases. Lancet 2009; 373: 1905–17. 61 Silverman EK, Chapman HA, Drazen JM, et al. Genetic
40 Chanez P, Vignola AM, O’Shaugnessy T, et al. Corticosteroid epidemiology of severe, early-onset chronic obstructive pulmonary
reversibility in COPD is related to features of asthma. disease. Risk to relatives for airflow obstruction and chronic
Am J Respir Crit Care Med 1997; 155: 1529–34. bronchitis. Am J Respir Crit Care Med 1998; 157: 1770–78.
41 Caramori G, Adcock IM, Di Stefano A, Chung KF. Cytokine 62 Vestbo J, Agusti A, Wouters EF, et al, and the Evaluation of COPD
inhibition in the treatment of COPD. Longitudinally to Identify Predictive Surrogate Endpoints Study
Int J Chron Obstruct Pulmon Dis 2014; 9: 397–412. Investigators. Should we view chronic obstructive pulmonary
42 Castaldi PJ, Dy J, Ross J, et al. Cluster analysis in the COPDGene disease differently after ECLIPSE? A clinical perspective from the
study identifies subtypes of smokers with distinct patterns of airway study team. Am J Respir Crit Care Med 2014; 189: 1022–30.
disease and emphysema. Thorax 2014; 69: 415–22. 63 Burgel PR, Paillasseur JL, Roche N. Identification of clinical
43 Wise RA, Anzueto A, Cotton D, et al, and the TIOSPIR phenotypes using cluster analyses in COPD patients with multiple
Investigators. Tiotropium Respimat inhaler and the risk of death in comorbidities. Biomed Res Int 2014; 2014: 420134.
COPD. N Engl J Med 2013; 369: 1491–501. 64 Stockley RA, Turner AM. α-1-Antitrypsin deficiency: clinical variability,
44 Verhamme KM, Afonso A, Romio S, Stricker BC, Brusselle GG, assessment, and treatment. Trends Mol Med 2014; 20: 105–15.
Sturkenboom MC. Use of tiotropium Respimat Soft Mist Inhaler 65 Agustí A, Edwards LD, Rennard SI, et al, and the Evaluation of
versus HandiHaler and mortality in patients with COPD. COPD Longitudinally to Identify Predictive Surrogate Endpoints
Eur Respir J 2013; 42: 606–15. (ECLIPSE) Investigators. Persistent systemic inflammation is
45 Gershon A, Croxford R, Calzavara A, et al. Cardiovascular safety of associated with poor clinical outcomes in COPD: a novel phenotype.
inhaled long-acting bronchodilators in individuals with chronic PLoS One 2012; 7: e37483.
obstructive pulmonary disease. JAMA Intern Med 2013; 173: 1175–85. 66 Bujarski S, Parulekar AD, Sharafkhaneh A, Hanania NA. The
46 Groenwold RH, de Vries F, de Boer A, et al. Balance measures for asthma COPD overlap syndrome (ACOS). Curr Allergy Asthma Rep
propensity score methods: a clinical example on beta-agonist use 2015; 15: 509.
and the risk of myocardial infarction. Pharmacoepidemiol Drug Saf 67 Brightling CE, Monteiro W, Ward R, et al. Sputum eosinophilia and
2011; 20: 1130–37. short-term response to prednisolone in chronic obstructive
47 Price D, Yawn B, Brusselle G, Rossi A. Risk-to-benefit ratio of pulmonary disease: a randomised controlled trial. Lancet 2000;
inhaled corticosteroids in patients with COPD. Prim Care Respir J 356: 1480–85.
2013; 22: 92–100. 68 Siva R, Green RH, Brightling CE, et al. Eosinophilic airway
48 Gershon AS, Campitelli MA, Croxford R, et al. Combination inflammation and exacerbations of COPD: a randomised controlled
long-acting β-agonists and inhaled corticosteroids compared with trial. Eur Respir J 2007; 29: 906–13.
long-acting β-agonists alone in older adults with chronic obstructive 69 Brightling CE, McKenna S, Hargadon B, et al. Sputum eosinophilia
pulmonary disease. JAMA 2014; 312: 1114–21. and the short term response to inhaled mometasone in chronic
49 Criner GJ, Cordova F, Sternberg AL, Martinez FJ. The National obstructive pulmonary disease. Thorax 2005; 60: 193–98.
Emphysema Treatment Trial (NETT) part II: lessons learned about 70 Leigh R, Pizzichini MM, Morris MM, Maltais F, Hargreave FE,
lung volume reduction surgery. Am J Respir Crit Care Med 2011; Pizzichini E. Stable COPD: predicting benefit from high-dose
184: 881–93. inhaled corticosteroid treatment. Eur Respir J 2006; 27: 964–71.
50 Diez D, Agustí A, Wheelock CE. Network analysis in the 71 Singh D, Kolsum U, Brightling CE, Locantore N, Agusti A,
investigation of chronic respiratory diseases. From basics to Tal-Singer R, and the ECLIPSE investigators. Eosinophilic
application. Am J Respir Crit Care Med 2014; 190: 981–88. inflammation in COPD: prevalence and clinical characteristics.
51 Roche N, Reddel HK, Agusti A, et al, on behalf of the Respiratory Eur Respir J 2014; 44: 1697–700.
Effectiveness Group. Integrating real-life studies in the global 72 Brightling CE, Bleecker ER, Panettieri RA Jr, et al. Benralizumab
therapeutic research framework. Lancet Respir Med 2013; for chronic obstructive pulmonary disease and sputum
1: e29–30. eosinophilia: a randomised, double-blind, placebo-controlled,
52 Rabe KF. Roflumilast for the treatment of chronic obstructive phase 2a study. Lancet Respir Med 2014; 2: 891–901.
pulmonary disease. Expert Rev Respir Med 2010; 4: 543–55. 73 Sethi S, Maloney J, Grove L, Wrona C, Berenson CS. Airway
53 Han MK, Tayob N, Murray S, et al. Predictors of chronic inflammation and bronchial bacterial colonization in chronic
obstructive pulmonary disease exacerbation reduction in response obstructive pulmonary disease. Am J Respir Crit Care Med 2006;
to daily azithromycin therapy. Am J Respir Crit Care Med 2014; 173: 991–98.
189: 1503–08. 74 Albert RK, Connett J, Bailey WC, et al, and the COPD Clinical
54 Crim C, Dransfield MT, Bourbeau J, et al. Pneumonia risk with Research Network. Azithromycin for prevention of exacerbations of
inhaled fluticasone furoate and vilanterol compared with COPD. N Engl J Med 2011; 365: 689–98.
vilanterol alone in patients with COPD. Ann Am Thorac Soc 2015; 75 Bafadhel M, Clark TW, Reid C, et al. Procalcitonin and C-reactive
12: 27–34. protein in hospitalized adult patients with community-acquired
55 Chung WS, Chen YF, Hsu JC, Yang WT, Chen SC, Chiang JY. pneumonia or exacerbation of asthma or COPD. Chest 2011;
Inhaled corticosteroids and the increased risk of pulmonary 139: 1410–18.
tuberculosis: a population-based case-control study. Int J Clin Pract 76 Martinez FJ, Curtis JL. Procalcitonin-guided antibiotic therapy in
2014; 68: 1193–99. COPD exacerbations: closer but not quite there. Chest 2007;
56 Wheelock CE, Goss VM, Balgoma D, et al, and the U-BIOPRED Study 131: 1–2.
Group. Application of ’omics technologies to biomarker discovery in 77 Sibila O, Garcia-Bellmunt L, Giner J, et al. Identification of airway
inflammatory lung diseases. Eur Respir J 2013; 42: 802–25. bacterial colonization by an electronic nose in chronic obstructive
57 Christenson SA, Steiling K, van den Berge M, et al. Asthma-COPD pulmonary disease. Respir Med 2014; 108: 1608–14.
overlap: clinical relevance of genomic signatures of type 2 78 Woodruff PG, Chatila W, Connett JE, et al, and the COPD Clinical
inflammation in COPD. Am J Respir Crit Care Med 2015; published Research Network. Tumour necrosis factor receptor-75 and risk of
online Jan 22. DOI:10.1164/rccm.201408-1458OC. COPD exacerbation in the azithromycin trial. Eur Respir J 2014;
58 van den Berge M, Steiling K, Timens W, et al. Airway gene 43: 295–98.
expression in COPD is dynamic with inhaled corticosteroid 79 Singh R, Mackay AJ, Patel AR, et al. Inflammatory thresholds and
treatment and reflects biological pathways associated with disease the species-specific effects of colonising bacteria in stable chronic
activity. Thorax 2014; 69: 14–23. obstructive pulmonary disease. Respir Res 2014; 15: 114.
www.thelancet.com Vol 385 May 2, 2015 1797
Series
80 Hill AT, Campbell EJ, Hill SL, Bayley DL, Stockley RA. Association 93 de Torres JP, Marín JM, Casanova C, et al. Lung cancer in patients
between airway bacterial load and markers of airway inflammation with chronic obstructive pulmonary disease—incidence and
in patients with stable chronic bronchitis. Am J Med 2000; predicting factors. Am J Respir Crit Care Med 2011; 184: 913–19.
109: 288–95. 94 de-Torres JP, Wilson DO, Sanchez-Salcedo P, et al. Lung cancer in
81 Barker BL, Haldar K, Patel H, et al. Association between pathogens patients with chronic obstructive pulmonary disease. Development
detected using quantitative polymerase chain reaction with airway and validation of the COPD lung cancer screening score.
inflammation in COPD at stable state and exacerbations. Am J Respir Crit Care Med 2015; 191: 285–91.
Chest 2015; 147: 46–55. 95 Kadara H, Fujimoto J, Yoo SY, et al. Transcriptomic architecture of
82 Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA. the adjacent airway field cancerization in non-small cell lung
Relationship between exacerbation frequency and lung function cancer. J Natl Cancer Inst 2014; 106: dju004.
decline in chronic obstructive pulmonary disease. Thorax 2002; 96 Brusselle G, Bracke K. Targeting immune pathways for therapy in
57: 847–52. asthma and chronic obstructive pulmonary disease.
83 Kanner RE, Anthonisen NR, Connett JE, and the Lung Health Ann Am Thorac Soc 2014; 11 (suppl 5): S322–28.
Study Research Group. Lower respiratory illnesses promote FEV(1) 97 Kohl P, Crampin EJ, Quinn TA, Noble D. Systems biology: an
decline in current smokers but not ex-smokers with mild chronic approach. Clin Pharmacol Ther 2010; 88: 25–33.
obstructive pulmonary disease: results from the lung health study. 98 Barabási AL. Network medicine--from obesity to the “diseasome”.
Am J Respir Crit Care Med 2001; 164: 358–64. N Engl J Med 2007; 357: 404–07.
84 Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of 99 Barabási AL, Gulbahce N, Loscalzo J. Network medicine: a network-
chronic obstructive pulmonary disease: identification of biologic based approach to human disease. Nat Rev Genet 2011; 12: 56–68.
clusters and their biomarkers. Am J Respir Crit Care Med 2011;
100 Menche J, Sharma A, Cho MH, et al. A diVIsive Shuffling Approach
184: 662–71.
(VIStA) for gene expression analysis to identify subtypes in Chronic
85 Bafadhel M, McKenna S, Terry S, et al. Blood eosinophils to direct Obstructive Pulmonary Disease. BMC Syst Biol 2014; 8 (suppl 2): S8.
corticosteroid treatment of exacerbations of chronic obstructive
101 Rennard SI, Locantore N, Delafont B, et al, on behalf of the
pulmonary disease: a randomized placebo-controlled trial.
Evaluation of COPD Longitudinally to Identify Predictive Surrogate
Am J Respir Crit Care Med 2012; 186: 48–55.
Endpoints investigators. Identification of five chronic obstructive
86 Bafadhel M, Davies L, Calverley PM, Aaron SD, Brightling CE, pulmonary disease subgroups with different prognoses in the
Pavord ID. Blood eosinophil guided prednisolone therapy for ECLIPSE cohort using cluster analysis. Ann Am Thorac Soc 2015;
exacerbations of COPD: a further analysis. Eur Respir J 2014; 12: 303–12.
44: 789–91.
102 Loscalzo J, Kohane I, Barabasi AL. Human disease classification in
87 Stolz D, Christ-Crain M, Morgenthaler NG, et al. Copeptin, the postgenomic era: a complex systems approach to human
C-reactive protein, and procalcitonin as prognostic biomarkers in pathobiology. Mol Syst Biol 2007; 3: 124.
acute exacerbation of COPD. Chest 2007; 131: 1058–67.
103 Vanfleteren LE, Kocks JW, Stone IS, et al. Moving from the Oslerian
88 Faner R, Cruz T, López-Giraldo A, Agustí A. Network medicine, paradigm to the post-genomic era: are asthma and COPD outdated
multimorbidity and the lung in the elderly. Eur Respir J 2014; terms? Thorax 2014; 69: 72–79.
44: 775–88.
104 Hood L, Balling R, Auffray C. Revolutionizing medicine in the
89 Grosdidier S, Ferrer A, Faner R, et al. Network medicine analysis of 21st century through systems approaches. Biotechnol J 2012;
COPD multimorbidities. Respir Res 2014; 15: 111. 7: 992–1001.
90 Cohen S, Nathan JA, Goldberg AL. Muscle wasting in disease: 105 Mirnezami R, Nicholson J, Darzi A. Preparing for precision
molecular mechanisms and promising therapies. medicine. N Engl J Med 2012; 366: 489–91.
Nat Rev Drug Discov 2015; 14: 58–74.
106 Collins FS, Varmus H. A new initiative on precision medicine.
91 Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in N Engl J Med 2015; 372: 793–95.
COPD: role of comorbidities. Eur Respir J 2006; 28: 1245–57.
107 Agusti A, MacNee W. The COPD control panel: towards
92 Gaga M, Powell CA, Schraufnagel DE, et al, and the ATS/ERS Task personalised medicine in COPD. Thorax 2013; 68: 687–90.
Force on the Role of the Pulmonologist in the Management of Lung
Cancer. An official American Thoracic Society/European
Respiratory Society statement: the role of the pulmonologist in the
diagnosis and management of lung cancer.
Am J Respir Crit Care Med 2013; 188: 503–07.
1798 www.thelancet.com Vol 385 May 2, 2015
You might also like
- PPS Pidsp Joint Position Statement On Pertussis Infection in Children and Support ForDocument6 pagesPPS Pidsp Joint Position Statement On Pertussis Infection in Children and Support ForDoc BenjchzNo ratings yet
- Test Bank For Merrills Atlas of Radiographic Positioning and Procedures 13th Edition by LongDocument6 pagesTest Bank For Merrills Atlas of Radiographic Positioning and Procedures 13th Edition by LongDonald Bonilla100% (34)
- Lesson Plan On MenopauseDocument16 pagesLesson Plan On MenopauseRavina Patel100% (6)
- Treatment of Fibrotic Interstitial Lung Disease Current ApproachesDocument11 pagesTreatment of Fibrotic Interstitial Lung Disease Current ApproachescastillojessNo ratings yet
- MakananDocument8 pagesMakananAnonymous VXZymiNo ratings yet
- Tani 2014Document4 pagesTani 2014Besiel Buendia J.No ratings yet
- PIIS2213260021001570Document14 pagesPIIS2213260021001570Hasna Ulya AnnafisNo ratings yet
- Multiple Sclerosis Lancet 2018Document15 pagesMultiple Sclerosis Lancet 2018Sarah Miryam CoffanoNo ratings yet
- Trauma To ArdsDocument9 pagesTrauma To ArdsSihsusetyaningtyas Tiominar SiregarNo ratings yet
- Chest: Health-Care-Associated Pneumonia Among Hospitalized Patients in A Japanese Community HospitalDocument8 pagesChest: Health-Care-Associated Pneumonia Among Hospitalized Patients in A Japanese Community HospitalAndi BintangNo ratings yet
- PIIS2213858721002357Document29 pagesPIIS2213858721002357Bladimir CentenoNo ratings yet
- Etanercept 80Document5 pagesEtanercept 805fqkqkcdhtNo ratings yet
- Effect of Procalcitonin-Guided Antibiotic Treatment On Mortality in Acute Respiratory Infections: A Patient Level Meta-AnalysisDocument36 pagesEffect of Procalcitonin-Guided Antibiotic Treatment On Mortality in Acute Respiratory Infections: A Patient Level Meta-Analysisrista ria ariniNo ratings yet
- Position Paper: David M Hansell, Jonathan G Goldin, Talmadge E King JR, David A Lynch, Luca Richeldi, Athol U WellsDocument14 pagesPosition Paper: David M Hansell, Jonathan G Goldin, Talmadge E King JR, David A Lynch, Luca Richeldi, Athol U WellsroachikitoNo ratings yet
- CD DX, LancetDocument29 pagesCD DX, Lancetimran karimNo ratings yet
- Myopathies Inflammatory InglesDocument13 pagesMyopathies Inflammatory InglesIvan VelasquezNo ratings yet
- Aetiology of Bronchiectasis in AdultsDocument8 pagesAetiology of Bronchiectasis in AdultsPamela CastilloNo ratings yet
- LancetDocument11 pagesLancetvieira.beatrizNo ratings yet
- Kumar Et Al. - 2016 - International Myeloma Working Group Consensus CritDocument19 pagesKumar Et Al. - 2016 - International Myeloma Working Group Consensus CritCarina MoitaNo ratings yet
- MJR 30 1 1Document2 pagesMJR 30 1 1landoo oooNo ratings yet
- Antibiotico en SepsisDocument15 pagesAntibiotico en SepsisJuan RodriguezNo ratings yet
- COPD 365771 New Perspectives On Chronic Obstructive Pulmonary DiseaseDocument10 pagesCOPD 365771 New Perspectives On Chronic Obstructive Pulmonary DiseaseDi LaNo ratings yet
- Acute Respiratory Distress Syndrome (ARDS) Developed Clinical Pathway: Suggested ProtocolDocument6 pagesAcute Respiratory Distress Syndrome (ARDS) Developed Clinical Pathway: Suggested ProtocolRia sasmitaNo ratings yet
- Paper Alumnos 5Document14 pagesPaper Alumnos 5Victor Martinez HagenNo ratings yet
- Bronchiectasis ExacerbationDocument14 pagesBronchiectasis ExacerbationAriandindi AriandiNo ratings yet
- Pneumonia 4Document10 pagesPneumonia 4furqan92No ratings yet
- Ethos 2020Document14 pagesEthos 2020Radu CiprianNo ratings yet
- 16 RaDocument10 pages16 RaNitish TankNo ratings yet
- Diagnosis of Stroke-Associated PneumoniaDocument6 pagesDiagnosis of Stroke-Associated Pneumoniapalmaputri pinantiNo ratings yet
- Cecconi_Sepsis_SepticShock_Review_Lancet_2018Document13 pagesCecconi_Sepsis_SepticShock_Review_Lancet_2018wendy pimientaperezNo ratings yet
- 2023 Canadian Thoracic Society GuidelineDocument25 pages2023 Canadian Thoracic Society GuidelineJohn Fray Totora CalisayaNo ratings yet
- Terapia Triple para EPOCDocument14 pagesTerapia Triple para EPOCSebastian Cebrian GuerreroNo ratings yet
- Review Sepsi LancetDocument13 pagesReview Sepsi LancetMr. LNo ratings yet
- Pone 0165942Document15 pagesPone 0165942rastiNo ratings yet
- Bronquiectasias Nuevas TerapiasDocument12 pagesBronquiectasias Nuevas TerapiasJuan ZamoraNo ratings yet
- Pro CalcDocument13 pagesPro CalcEdison QueirozNo ratings yet
- FullDocument20 pagesFulledith calderonNo ratings yet
- Transforming Translation Impact of Clinical and Translational ScienceDocument3 pagesTransforming Translation Impact of Clinical and Translational ScienceSamNo ratings yet
- Quantitative CT Analysis of Diffuse Lung DiseaseDocument16 pagesQuantitative CT Analysis of Diffuse Lung DiseaseLicinioBritoNo ratings yet
- BMJ 2021 065871.fullDocument24 pagesBMJ 2021 065871.fullEfen YtNo ratings yet
- PIIS2213260022005355Document16 pagesPIIS2213260022005355evelyn.minichNo ratings yet
- 2023 Canadian Thoracic Society Guideline On Pharmacotherapy in Patients With Stable COPDDocument25 pages2023 Canadian Thoracic Society Guideline On Pharmacotherapy in Patients With Stable COPDgramachandran186No ratings yet
- Clinical Microbiology and InfectionDocument6 pagesClinical Microbiology and InfectionAccel XtremeNo ratings yet
- COPD Biomarkers and Their Interpretation. Ajrccm.2018Document10 pagesCOPD Biomarkers and Their Interpretation. Ajrccm.2018Claudio Rafael Salazar MNo ratings yet
- Lancet Sclerosi MultiplaDocument15 pagesLancet Sclerosi MultiplaMr. LNo ratings yet
- Glasgow Prognostic Score Class 2 Predicts Prolonged Intensive Care Unit Stay in Patients Undergoing PneumonectomyDocument7 pagesGlasgow Prognostic Score Class 2 Predicts Prolonged Intensive Care Unit Stay in Patients Undergoing PneumonectomyDavide RadiceNo ratings yet
- Migraine Integrated Approaches To Clinical ManagementDocument14 pagesMigraine Integrated Approaches To Clinical ManagementJOHN ROMERO CEVALLOSNo ratings yet
- Efficacy and Safety of Acupoint Autohemotherapy in PDFDocument5 pagesEfficacy and Safety of Acupoint Autohemotherapy in PDFtizziana carollaNo ratings yet
- Pittsburgh Lung Conference: PneumoniaDocument4 pagesPittsburgh Lung Conference: PneumoniaYudha Rental'sNo ratings yet
- A New Vision of Definition, Commentary, and Understanding in Clinical and Translational MedicineDocument3 pagesA New Vision of Definition, Commentary, and Understanding in Clinical and Translational MedicineMahmoud HakimNo ratings yet
- Emergencia CoronavirusDocument19 pagesEmergencia CoronavirusFelixNo ratings yet
- Immunotherapy in Non Small Cell Lung Cancer Facts and HopeDocument22 pagesImmunotherapy in Non Small Cell Lung Cancer Facts and HopeasdffdsaNo ratings yet
- New Guidelines For Hospital-Acquired Pneumonia/ Ventilator-Associated Pneumonia: USA vs. EuropeDocument6 pagesNew Guidelines For Hospital-Acquired Pneumonia/ Ventilator-Associated Pneumonia: USA vs. EuropeWillian Palma GómezNo ratings yet
- Primer: BronchiectasisDocument18 pagesPrimer: BronchiectasisAnanta Bryan Tohari WijayaNo ratings yet
- 2012 Opioides em CancerDocument11 pages2012 Opioides em CancerSarha AndradeNo ratings yet
- Clinical Commentary: Chronic Obstructive Pulmonary Disease PhenotypesDocument7 pagesClinical Commentary: Chronic Obstructive Pulmonary Disease PhenotypesNurusshiami KhairatiNo ratings yet
- Early ViewDocument34 pagesEarly Viewyesid urregoNo ratings yet
- JTD 09 07 2178Document8 pagesJTD 09 07 2178Hafiz Hari NugrahaNo ratings yet
- Chest.126.2.592 MBE EN UCIDocument9 pagesChest.126.2.592 MBE EN UCIJaime RomeroNo ratings yet
- Comparison of Methicillin-Resistant Community-Acquired and Healthcare-Associated PneumoniaDocument8 pagesComparison of Methicillin-Resistant Community-Acquired and Healthcare-Associated PneumoniaSuarniNo ratings yet
- Clinical Characterization Cohort Systemic Lupus Erythematosus. PLoS One-2023Document14 pagesClinical Characterization Cohort Systemic Lupus Erythematosus. PLoS One-2023Jorge Ricardo Parra CamachoNo ratings yet
- Phenotypes Copd 2018Document10 pagesPhenotypes Copd 2018Angelica ChavesNo ratings yet
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareFrom EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareNo ratings yet
- Awareness and Utilization of Rehabilitation Services AmongDocument4 pagesAwareness and Utilization of Rehabilitation Services AmongAnindita BalaganesanNo ratings yet
- CSEC Social Studies January 2016 P032Document8 pagesCSEC Social Studies January 2016 P032Luke NancooNo ratings yet
- NRL GlassDocument28 pagesNRL Glasskaf micrNo ratings yet
- Dental WaiverDocument1 pageDental WaiverMary Grace LemonNo ratings yet
- Ebook Rook S Dermatology Handbook Christopher E Griffiths Tanya O Bleiker Daniel Creamer John R Ingram Rosalind C Simpson Eds Online PDF All ChapterDocument70 pagesEbook Rook S Dermatology Handbook Christopher E Griffiths Tanya O Bleiker Daniel Creamer John R Ingram Rosalind C Simpson Eds Online PDF All Chaptermichael.faircloth221100% (7)
- Carpal Tunnel SyndromeDocument5 pagesCarpal Tunnel SyndromeBùi Ngọc Anh HSTCNo ratings yet
- CardiomegalyDocument91 pagesCardiomegalyMariquita Buenafe100% (1)
- Fructose and ObesityDocument27 pagesFructose and Obesitya.enesmadenNo ratings yet
- Microsoft Word - Aow 11-15-20Document2 pagesMicrosoft Word - Aow 11-15-20api-539266252No ratings yet
- NO Particular Pages 1. 2 2. Problem Statement 3 3. Literature Review 4-6 4. Discussion 7-13 5. Conclusion 14 6. Reference List 15 7. Attachment 16-17Document17 pagesNO Particular Pages 1. 2 2. Problem Statement 3 3. Literature Review 4-6 4. Discussion 7-13 5. Conclusion 14 6. Reference List 15 7. Attachment 16-17Fardzli MatjakirNo ratings yet
- Routine UrinalysisDocument2 pagesRoutine UrinalysisSkylar MendesNo ratings yet
- كتاب دكتور حبشي- جزء 2 ;كامل- مجانا PDFDocument359 pagesكتاب دكتور حبشي- جزء 2 ;كامل- مجانا PDFSara YehiaNo ratings yet
- Application of Fascial Manipulation Technique in Chronic Shoulder Pain Ok PDFDocument8 pagesApplication of Fascial Manipulation Technique in Chronic Shoulder Pain Ok PDFBruno DiasNo ratings yet
- Conjunction ParagraphDocument1 pageConjunction ParagraphMuhammad Dimas Syahadatain50% (2)
- Ujian Feb 2023Document7 pagesUjian Feb 2023kumoro panjiNo ratings yet
- Awen Homeopathy - Introduction To HomeopathyDocument81 pagesAwen Homeopathy - Introduction To HomeopathyPaulo JiurgiuNo ratings yet
- Cir 0000000000000549Document120 pagesCir 0000000000000549MSNo ratings yet
- LYMPHOGRAPHY-WPS OfficeDocument11 pagesLYMPHOGRAPHY-WPS OfficePax Giuseppe0% (1)
- FNCPDocument12 pagesFNCPMikko McDonie VeloriaNo ratings yet
- First Aid Safety Dimensions of Development 1Document28 pagesFirst Aid Safety Dimensions of Development 1contactlucielphNo ratings yet
- Lecture 33-Structure and Physiology of Fungi-Prof. Dr. Tri Wibawa, PHD, SP - MK (2018) PDFDocument56 pagesLecture 33-Structure and Physiology of Fungi-Prof. Dr. Tri Wibawa, PHD, SP - MK (2018) PDFannisaNo ratings yet
- Aetcom QuesDocument11 pagesAetcom QuesDiyNo ratings yet
- What Is Chronic Venous Insufficiency (CVI) ?Document2 pagesWhat Is Chronic Venous Insufficiency (CVI) ?atika5No ratings yet
- 3 in 1 40k Ultrasonic Cavitation Slimming Machine ManualDocument15 pages3 in 1 40k Ultrasonic Cavitation Slimming Machine ManualyasarspaNo ratings yet
- AkapulkoDocument18 pagesAkapulkoGladys Degala DizonNo ratings yet
- Urinary Diagnosis TestDocument31 pagesUrinary Diagnosis TestR الالمعيNo ratings yet
- Ljungberg 1992Document7 pagesLjungberg 1992LIZARDO CRUZADO DIAZNo ratings yet