Download as pdf or txt
You might also like
- Information Technology (Pure Genius-1,2 & 8)Document3 pagesInformation Technology (Pure Genius-1,2 & 8)michael almadenNo ratings yet
- All India 20 Crore Database SampleDocument304 pagesAll India 20 Crore Database SampleVikram100% (1)
- Brand Audit - Red BullDocument13 pagesBrand Audit - Red BullLavi BeeNo ratings yet
- Bureau GrotDocument4 pagesBureau GrotMay KrivanishNo ratings yet
- Odontogenic Tumors IIDocument24 pagesOdontogenic Tumors IIIbn HabibNo ratings yet
- Syncope: - Selvarathi KDocument27 pagesSyncope: - Selvarathi KSelvarathi KandhaswamyNo ratings yet
- Calcium Homeostasis: Endocrine Regulation of (Ca)Document4 pagesCalcium Homeostasis: Endocrine Regulation of (Ca)PRANAB KUMAR MUKHERJEENo ratings yet
- Diseases of The Temporomandibular JointDocument27 pagesDiseases of The Temporomandibular JointJustDen090% (1)
- Muscles of MasticationDocument112 pagesMuscles of MasticationEazhil RajNo ratings yet
- TMJ ImanDocument46 pagesTMJ Imanimaniyas imanNo ratings yet
- I.T.S Dental College, Greater Noida: FacultyDocument70 pagesI.T.S Dental College, Greater Noida: FacultyAMIT GUPTANo ratings yet
- Amelogenesis: Prof. Shaleen ChandraDocument16 pagesAmelogenesis: Prof. Shaleen ChandraSheshayi RoyNo ratings yet
- SalivaDocument102 pagesSalivacareNo ratings yet
- Space InfectionsDocument60 pagesSpace InfectionsDan 04No ratings yet
- Temporomandibular Disorders and ManagementDocument79 pagesTemporomandibular Disorders and ManagementVijay ChinthaNo ratings yet
- Evolution of TMJ and Development of TMJDocument11 pagesEvolution of TMJ and Development of TMJAkash AmbhoreNo ratings yet
- Alveolar Bone in HealthDocument43 pagesAlveolar Bone in HealthAdit VekariaNo ratings yet
- TMJDocument40 pagesTMJARIF PUJI LAKSONONo ratings yet
- Dev of Hard & Soft PalateDocument94 pagesDev of Hard & Soft PalatepriyaNo ratings yet
- Development of Palate: DR - Sowmya K 1 Year PG Dept of ProsthodonticsDocument49 pagesDevelopment of Palate: DR - Sowmya K 1 Year PG Dept of Prosthodonticssowmya krishnamurthiNo ratings yet
- Ankylosis of Temporomandibular JointDocument46 pagesAnkylosis of Temporomandibular JointRambabu SatipedakalaNo ratings yet
- Surgical Anatomy of Parotid Gland - Ommos - Edition-01-SoiDocument32 pagesSurgical Anatomy of Parotid Gland - Ommos - Edition-01-SoiDr Prashant Kumar100% (1)
- Cranial Fossae: Zara Denisse Garcia Ella Carmela Chavez Mae Nen Vedeja Mardred MarceloDocument40 pagesCranial Fossae: Zara Denisse Garcia Ella Carmela Chavez Mae Nen Vedeja Mardred MarceloZara Sebastianne GarciaNo ratings yet
- Functional Anatomy of Temporomandibular JointDocument46 pagesFunctional Anatomy of Temporomandibular JointSiddharth Sharma100% (2)
- Giant Cell Lesions of The Jaws: DR Syeda Noureen IqbalDocument61 pagesGiant Cell Lesions of The Jaws: DR Syeda Noureen IqbalMuhammad maaz khanNo ratings yet
- Embolism and InfarctionDocument34 pagesEmbolism and InfarctionDiviya ArikrishnanNo ratings yet
- Trigeminal Nerve (Cranial Nerve V) : Presented By: Hamza Yousaf Usaid Yousaf Amna Khalil Maha Aziz Rimsha AkramDocument30 pagesTrigeminal Nerve (Cranial Nerve V) : Presented By: Hamza Yousaf Usaid Yousaf Amna Khalil Maha Aziz Rimsha AkramHamza YousafNo ratings yet
- Fracture of The Mandible (Repaired)Document67 pagesFracture of The Mandible (Repaired)Arafat Masud NiloyNo ratings yet
- Corticosteroids: Ghadi Mahmoud Elbarghathi Roll Number: 1950 5 Year 2021-2022Document26 pagesCorticosteroids: Ghadi Mahmoud Elbarghathi Roll Number: 1950 5 Year 2021-2022Ghadi ElbarghathiNo ratings yet
- Muscles of MasticationDocument130 pagesMuscles of MasticationDevanand GuptaNo ratings yet
- AmelogenesisDocument84 pagesAmelogenesisdiksha sinhaNo ratings yet
- InfluenzaDocument16 pagesInfluenzaTrue AlphaNo ratings yet
- EnamelDocument61 pagesEnamelRehab NaeemNo ratings yet
- Anestesi LokalDocument12 pagesAnestesi LokalKurniatiKhasanahQhafisaQurratul'ainNo ratings yet
- Alveolar Bone: Ist Year ClassDocument47 pagesAlveolar Bone: Ist Year ClassABHINAVNo ratings yet
- 5 HypoxiaDocument42 pages5 HypoxiaShanzayNo ratings yet
- Development of Face and Oral Cavity 12042015Document40 pagesDevelopment of Face and Oral Cavity 12042015Jamal NaimNo ratings yet
- Muscles of Mastication 2Document80 pagesMuscles of Mastication 2DENTALORG.COMNo ratings yet
- Mandible FinalDocument105 pagesMandible FinalErly Berlianda100% (1)
- Facial Nerve - AnatomyDocument19 pagesFacial Nerve - AnatomyMeghana Patil100% (1)
- Odontomes & Odontogenic Tumors II (Slide 18+19)Document39 pagesOdontomes & Odontogenic Tumors II (Slide 18+19)JustDen09No ratings yet
- 11 Residual Ridge ResorptionDocument66 pages11 Residual Ridge ResorptionSuman JainNo ratings yet
- Healing of Extraction SocketDocument21 pagesHealing of Extraction SocketSushant Pandey100% (1)
- Oncology: Study of TumorsDocument32 pagesOncology: Study of TumorsGeorge CherianNo ratings yet
- Condylar Fracture: Muhammad Tahoor D17015Document36 pagesCondylar Fracture: Muhammad Tahoor D17015Umair KhalidNo ratings yet
- Prenatal Growth of MaxillaDocument27 pagesPrenatal Growth of MaxillaAnubhuti SabhlokNo ratings yet
- Rectum & Anal CanalDocument14 pagesRectum & Anal CanalLisa DentonNo ratings yet
- Development of TeethDocument25 pagesDevelopment of TeethDrShweta Saini100% (1)
- 03 Amelogenesis - EnglishDocument158 pages03 Amelogenesis - Englishvishal tiwaryNo ratings yet
- II - 51. The Parotid Salivary GlandDocument5 pagesII - 51. The Parotid Salivary GlandAndra BauerNo ratings yet
- Surgical Anatomy of Mandible DeptDocument92 pagesSurgical Anatomy of Mandible Deptbhavaaishu100% (1)
- Slides 9 - Pulp and Periradicular PathosisDocument39 pagesSlides 9 - Pulp and Periradicular PathosisCWT2010100% (1)
- Anatomy of PalateDocument33 pagesAnatomy of Palatekvellingiri0% (1)
- Cleft PalateDocument11 pagesCleft Palatealison quahNo ratings yet
- ORAL MICROBIAL FLORA PriyaDocument149 pagesORAL MICROBIAL FLORA Priyajaishreerijhwani100% (1)
- Mandibular Second Premolar: Prof. A. El-SahnDocument68 pagesMandibular Second Premolar: Prof. A. El-SahnRekha PtsNo ratings yet
- Le Fort FracturesDocument105 pagesLe Fort FracturesnasimNo ratings yet
- Management of The Temporomandibular JointDocument45 pagesManagement of The Temporomandibular JointErinda ChuzaifahNo ratings yet
- Muscles of MasticationDocument8 pagesMuscles of MasticationNaisi Naseem100% (1)
- Fix. Musculosceletal Anatomy (DR - Hendra)Document33 pagesFix. Musculosceletal Anatomy (DR - Hendra)rumah sakit daerahNo ratings yet
- Fracture HealingDocument23 pagesFracture Healingjomari dvNo ratings yet
- Bone HealingDocument23 pagesBone Healingpecolaa3No ratings yet
- Handout - Bone Anatomy and Healing - Nlogo - HighDocument11 pagesHandout - Bone Anatomy and Healing - Nlogo - HighlevimacoNo ratings yet
- Fractures: Anandkumar Balakrishna Wong Poh Sean Mohd Hanafi RamleeDocument160 pagesFractures: Anandkumar Balakrishna Wong Poh Sean Mohd Hanafi RamleeMahadhir AkmalNo ratings yet
- Hg-Minutes Homeroom GuidanceDocument3 pagesHg-Minutes Homeroom GuidanceJayr CaponponNo ratings yet
- Upload Paper For OpapersDocument31 pagesUpload Paper For OpapersMuhamad Eddin SyazriNo ratings yet
- Overview of Academic Researches On VranaDocument15 pagesOverview of Academic Researches On VranaMSKCNo ratings yet
- Form 5 of DILG MC No. 2018-135 BPOC Monitoring Form 2 (DILG MC No. 2020-047) Ltia Form 3 (Dilg MC No. 2016-58)Document5 pagesForm 5 of DILG MC No. 2018-135 BPOC Monitoring Form 2 (DILG MC No. 2020-047) Ltia Form 3 (Dilg MC No. 2016-58)jacquelyn samson100% (1)
- Miasms and Nosodes Volume I Louis Klein.04531 1Document22 pagesMiasms and Nosodes Volume I Louis Klein.04531 1Velu SubramanianNo ratings yet
- 12 - Umali Utilizing Onion (Allium Cepa L.) Peels Into Organic StrawDocument35 pages12 - Umali Utilizing Onion (Allium Cepa L.) Peels Into Organic Strawfaith tolentinoNo ratings yet
- @anesthesia Books 2018 AnaesthesiaDocument64 pages@anesthesia Books 2018 AnaesthesiaEva Garcia MartinezNo ratings yet
- Omoung LassiDocument3 pagesOmoung LassiWaqas MehmoodNo ratings yet
- Lecture 8Document23 pagesLecture 8tarhuniNo ratings yet
- Csa 121 Softening ResinDocument2 pagesCsa 121 Softening ResinkjadnNo ratings yet
- Jobs Lost Jobs Gain - McKinsey Slide DeckDocument14 pagesJobs Lost Jobs Gain - McKinsey Slide DeckThành Trung LêNo ratings yet
- IEEE STD 1050-89Document81 pagesIEEE STD 1050-89Flo Mirca100% (1)
- TLE Worksheets Carpentry 7 and 8 Q3Document2 pagesTLE Worksheets Carpentry 7 and 8 Q3Xyra Zheniel PerezNo ratings yet
- HV Cable Sizing Calculation (MOL) - FahahilDocument5 pagesHV Cable Sizing Calculation (MOL) - Fahahilkarikal_valavan100% (3)
- TDS - PURITY GUM® Ultra EmulsifierDocument2 pagesTDS - PURITY GUM® Ultra EmulsifierKapithas KNo ratings yet
- Calculations in ChemistryDocument7 pagesCalculations in ChemistryKhondokar TarakkyNo ratings yet
- Down SyndromeDocument12 pagesDown SyndromeUrbanus Matilu100% (1)
- CLASS - XII - BIOLOGY - MCQS - Chapter 2 Sexual Reproduction in Flowering PlantsDocument9 pagesCLASS - XII - BIOLOGY - MCQS - Chapter 2 Sexual Reproduction in Flowering PlantsJijendarNo ratings yet
- Women EntrepreneursDocument7 pagesWomen Entrepreneursvinodjoshi22No ratings yet
- Psych BulletsDocument16 pagesPsych BulletsPrince Rener Velasco PeraNo ratings yet
- All Things Black Seed OilDocument39 pagesAll Things Black Seed Oilreza zulfi prasetyaNo ratings yet
- Ajsir 4 6 540 545Document6 pagesAjsir 4 6 540 545Zahiroh Maulida A NNo ratings yet
- The Science of LoveDocument12 pagesThe Science of LoveJerico Kier YesyesNo ratings yet
- HavmoreDocument11 pagesHavmorebhhhhNo ratings yet
- Friedreich AtaxiaDocument18 pagesFriedreich AtaxiaGamer MadaNo ratings yet
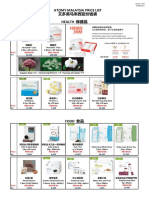
- Atomy Malaysia Price List 艾多美马来西亚价钱表 Health 保健品Document6 pagesAtomy Malaysia Price List 艾多美马来西亚价钱表 Health 保健品Lee Ling PengNo ratings yet