
Penatalaksanaan Kejang Pada Covid19: Suryo Bantolo Rs Dcwak
Penatalaksanaan Kejang Pada Covid19: Suryo Bantolo Rs Dcwak
You might also like
- Cramsheet (Exam Cram Nclex PN)Document2 pagesCramsheet (Exam Cram Nclex PN)Katrina Reyes94% (32)
- Neonatal Seizures: Postgraduate Dept of PediatricsDocument42 pagesNeonatal Seizures: Postgraduate Dept of PediatricsG VenkateshNo ratings yet
- ESCOP Monographien Suppl 2009Document4 pagesESCOP Monographien Suppl 2009AN Marcos0% (1)
- Neurology Paediatric ProtocolDocument44 pagesNeurology Paediatric ProtocolkirannesarajahNo ratings yet
- Status EpilepticusDocument28 pagesStatus EpilepticusDaniel AlfredNo ratings yet
- Neo SeizureDocument27 pagesNeo SeizureAchyut KanungoNo ratings yet
- Protocolo de Estatus EpilepticoDocument3 pagesProtocolo de Estatus EpilepticojiovannaescalanteNo ratings yet
- Status Epilepticus - Clinical Featurespathopysiologyand Treatmentcraig WatsonmdphdDocument30 pagesStatus Epilepticus - Clinical Featurespathopysiologyand Treatmentcraig WatsonmdphdSri Ram 07No ratings yet
- Status EpilepticusDocument27 pagesStatus EpilepticusSaad KhanNo ratings yet
- Epi LepsiDocument41 pagesEpi LepsiElvon DailyNo ratings yet
- Status Epilepticus ManagementDocument20 pagesStatus Epilepticus Managementarunvij797No ratings yet
- Convulsion, Spasm and UnconsciousnessDocument19 pagesConvulsion, Spasm and UnconsciousnessKatrin Marcelina SihombingNo ratings yet
- 1st Line Medication of An e CartDocument5 pages1st Line Medication of An e CartColette Marie PerezNo ratings yet
- Pediatric Status Epilepticus Pathway-FINALDocument5 pagesPediatric Status Epilepticus Pathway-FINALvural kesikNo ratings yet
- Case PBL Icm II Week 6 MondayDocument4 pagesCase PBL Icm II Week 6 MondayRaqqi PujatmikoNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- Status Epilepticus: Susilo SiswonotoDocument14 pagesStatus Epilepticus: Susilo SiswonotoAhmad Shafwan NatsirNo ratings yet
- Status EpilepticusDocument43 pagesStatus EpilepticusPatsuda DreematurakulNo ratings yet
- Convulsion, Spasm and UnconsciousnessDocument19 pagesConvulsion, Spasm and UnconsciousnessDesima Tamara sinuratNo ratings yet
- Convulsion, Spasm and UnconsciousnessDocument19 pagesConvulsion, Spasm and UnconsciousnessJoko Pratama AtmayudhaNo ratings yet
- Paediatric Clinical GuidelinesDocument7 pagesPaediatric Clinical GuidelinesAndriNo ratings yet
- ConnectorDocument4 pagesConnectoryetaung8No ratings yet
- Treatment Protocol of SnakebiteDocument23 pagesTreatment Protocol of SnakebiteEduconsultNo ratings yet
- Crisis ConvulsivaDocument3 pagesCrisis ConvulsivaJosé Victor Velez DelgadoNo ratings yet
- 7698alorithm SeizureDocument3 pages7698alorithm Seizureboromeus abyasa daniswara100% (1)
- Febrile Seizures: Status EpilepticusDocument34 pagesFebrile Seizures: Status EpilepticusSAIMA BATOOLNo ratings yet
- UNIT: Internal Medicine REG NO.: BMS/2014/72732 DATE: 30/7/2021 ASSIGNMENT: Status EpilepticusDocument10 pagesUNIT: Internal Medicine REG NO.: BMS/2014/72732 DATE: 30/7/2021 ASSIGNMENT: Status EpilepticusGladys MainaNo ratings yet
- Status EpilepticusDocument42 pagesStatus EpilepticusJesse EstradaNo ratings yet
- Approach and Management of Neonatal SeizuresDocument42 pagesApproach and Management of Neonatal SeizuresG Venkatesh100% (1)
- O&G Off-Tag Assesment Logbook: Traces-Pdf-248732173Document9 pagesO&G Off-Tag Assesment Logbook: Traces-Pdf-248732173niwasNo ratings yet
- Treatment of Prolonged SeizuresDocument1 pageTreatment of Prolonged SeizuresAhmad ShukriNo ratings yet
- Lec 4 CNSDocument12 pagesLec 4 CNShusainozelNo ratings yet
- Status Epilepticus: DR Abdelmoniem SaeedDocument24 pagesStatus Epilepticus: DR Abdelmoniem SaeedYousef Al-AmeenNo ratings yet
- Status Epilepticus: BY DR Muhammad Usman DR Areeba NaeemDocument16 pagesStatus Epilepticus: BY DR Muhammad Usman DR Areeba NaeemFarhan AfzalNo ratings yet
- Neurological EmergenciesDocument47 pagesNeurological EmergenciesStellate Repentance100% (1)
- Case Study Assignment On Open Cholecystectomy - MoodleDocument2 pagesCase Study Assignment On Open Cholecystectomy - MoodleHouda HayekNo ratings yet
- Pediatric Status Epilepticus CPGDocument3 pagesPediatric Status Epilepticus CPGAlex GasnasNo ratings yet
- Diabetic Foot Case PresentationDocument58 pagesDiabetic Foot Case PresentationZH. omg sarNo ratings yet
- Management of Eclampsia and Magnesium ToxicityDocument34 pagesManagement of Eclampsia and Magnesium ToxicityRezki IsharNo ratings yet
- Status EpilepsiDocument11 pagesStatus EpilepsiNurul aulia AbdullahNo ratings yet
- Approach To Status EpilepticusDocument21 pagesApproach To Status EpilepticusRoopam OjhaNo ratings yet
- Neonatal Seizures and Management: Dhaka Sishu Hospital BangladeshDocument19 pagesNeonatal Seizures and Management: Dhaka Sishu Hospital BangladeshGoha BashaNo ratings yet
- ENLS Status Epilepticus ProtocolDocument12 pagesENLS Status Epilepticus ProtocolFransiskus MikaelNo ratings yet
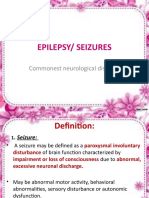
- Epilepsy/ Seizures: Commonest Neurological DisorderDocument25 pagesEpilepsy/ Seizures: Commonest Neurological DisorderAlokh Saha RajNo ratings yet
- Approach in Children With SeizuresDocument26 pagesApproach in Children With SeizuresMD Luthfy LubisNo ratings yet
- Eclampsia-Icu Management ProtocolDocument3 pagesEclampsia-Icu Management ProtocolmatentenNo ratings yet
- Malignan HipertermiaDocument10 pagesMalignan HipertermiaAstrid Ghea GayatriNo ratings yet
- Management of EclampsiaDocument24 pagesManagement of EclampsiaDup SuNo ratings yet
- Obat-Obat Emergency: DR T. Mamfaluti, SPPDDocument36 pagesObat-Obat Emergency: DR T. Mamfaluti, SPPDIqbal AminNo ratings yet
- Management of Hypertensive EmergencyDocument35 pagesManagement of Hypertensive EmergencyRaditya Indah TofaniNo ratings yet
- Seminar On SEDocument49 pagesSeminar On SEmubarak abdulkadirNo ratings yet
- Status Epileptic UsDocument66 pagesStatus Epileptic UsHakimah K. SuhaimiNo ratings yet
- Advanced Cardiac Life Support PDFDocument9 pagesAdvanced Cardiac Life Support PDFYulias YoweiNo ratings yet
- Management of Severe Hypertension, Hypertension in Special ConditionDocument43 pagesManagement of Severe Hypertension, Hypertension in Special Conditionabhandlung100% (3)
- Status Epilepticus and Its Management AssignmentDocument11 pagesStatus Epilepticus and Its Management AssignmentStanley KarugaNo ratings yet
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Fast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteFrom EverandFast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteNo ratings yet
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Vertigo, A Simple Guide to The Condition, Treatment And Related ConditionsFrom EverandVertigo, A Simple Guide to The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Biopharmaceutics-RED PACOPDocument588 pagesBiopharmaceutics-RED PACOPArk Olfato ParojinogNo ratings yet
- Aspirin and Salicylates: SourcesDocument3 pagesAspirin and Salicylates: SourcesahmedNo ratings yet
- Compliled DrugstudyDocument15 pagesCompliled DrugstudyApril Jan D. Alagon0% (1)
- Running Head: Pharmacology 1Document5 pagesRunning Head: Pharmacology 1jacobNo ratings yet
- Price List Generik PT Bernofarm Per 18 April THN 2011Document3 pagesPrice List Generik PT Bernofarm Per 18 April THN 2011Mandha UmamiiNo ratings yet
- Menghitung DosisDocument17 pagesMenghitung Dosisbaekhyunwoo1010No ratings yet
- Vere Labs: VL-Delta 8 THC Cartridge 1Document1 pageVere Labs: VL-Delta 8 THC Cartridge 1Michael WalkerNo ratings yet
- KlienDocument47 pagesKlientareq.sefatNo ratings yet
- HCG - Human Chorionic GonadotropinDocument2 pagesHCG - Human Chorionic GonadotropinOvidiu IgnatNo ratings yet
- BPL Annual 2019 20Document192 pagesBPL Annual 2019 20Ehsan Ul Karim Aonkon (181011286)No ratings yet
- PT - Permata Delta Agung: Halaman: (All)Document35 pagesPT - Permata Delta Agung: Halaman: (All)abdul husainNo ratings yet
- PRELIM EXAM - International BusinessDocument4 pagesPRELIM EXAM - International BusinessVel JuneNo ratings yet
- DRUG STUDY-Magnesium SulfateDocument2 pagesDRUG STUDY-Magnesium SulfateCarissa Mae Tapec Estrada80% (5)
- Immunization Training GuideDocument91 pagesImmunization Training Guidezenagit123456100% (1)
- Original Article: AbstractDocument4 pagesOriginal Article: AbstractAndikaPratamaPutraNo ratings yet
- Appropriateness For Ldts Companion DX Assays: Perspectives On To Be Used AsDocument16 pagesAppropriateness For Ldts Companion DX Assays: Perspectives On To Be Used AsfdablogNo ratings yet
- Apotik ApotikDocument66 pagesApotik Apotikdessy wilantariNo ratings yet
- 50 Most Commonly Used DrugsDocument1 page50 Most Commonly Used DrugsElizabeth uNo ratings yet
- Thrombolytics & Anti Platelet DrugsDocument38 pagesThrombolytics & Anti Platelet DrugsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- CiprofloxacinDocument6 pagesCiprofloxacinNasser AlhajjNo ratings yet
- Drugalertnov 23Document14 pagesDrugalertnov 23rashidhasan2001No ratings yet
- Rapid Tranquillisation Training PresentationDocument42 pagesRapid Tranquillisation Training PresentationmindpinkNo ratings yet
- Daftar Inventaris ApotekDocument3 pagesDaftar Inventaris ApotekMei Kurniawati TaharaNo ratings yet
- Ospolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)Document7 pagesOspolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)ddandan_2No ratings yet
- Pharmacology ReviewDocument64 pagesPharmacology ReviewRichard BakerNo ratings yet
- Anaesthetic Drug Crib Sheet-8 PDFDocument1 pageAnaesthetic Drug Crib Sheet-8 PDFKevin Ariel Tiopan SimanjuntakNo ratings yet
- Contoh Form ChecklistDocument39 pagesContoh Form ChecklistYastika YarsalNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka: Medicinal Chemistry - I Q.P. CODE: 5014Document1 pageRajiv Gandhi University of Health Sciences, Karnataka: Medicinal Chemistry - I Q.P. CODE: 5014Monica100% (1)
























































































Download as pdf or txt
You might also like
- Cramsheet (Exam Cram Nclex PN)Document2 pagesCramsheet (Exam Cram Nclex PN)Katrina Reyes94% (32)
- Neonatal Seizures: Postgraduate Dept of PediatricsDocument42 pagesNeonatal Seizures: Postgraduate Dept of PediatricsG VenkateshNo ratings yet
- ESCOP Monographien Suppl 2009Document4 pagesESCOP Monographien Suppl 2009AN Marcos0% (1)
- Neurology Paediatric ProtocolDocument44 pagesNeurology Paediatric ProtocolkirannesarajahNo ratings yet
- Status EpilepticusDocument28 pagesStatus EpilepticusDaniel AlfredNo ratings yet
- Neo SeizureDocument27 pagesNeo SeizureAchyut KanungoNo ratings yet
- Protocolo de Estatus EpilepticoDocument3 pagesProtocolo de Estatus EpilepticojiovannaescalanteNo ratings yet
- Status Epilepticus - Clinical Featurespathopysiologyand Treatmentcraig WatsonmdphdDocument30 pagesStatus Epilepticus - Clinical Featurespathopysiologyand Treatmentcraig WatsonmdphdSri Ram 07No ratings yet
- Status EpilepticusDocument27 pagesStatus EpilepticusSaad KhanNo ratings yet
- Epi LepsiDocument41 pagesEpi LepsiElvon DailyNo ratings yet
- Status Epilepticus ManagementDocument20 pagesStatus Epilepticus Managementarunvij797No ratings yet
- Convulsion, Spasm and UnconsciousnessDocument19 pagesConvulsion, Spasm and UnconsciousnessKatrin Marcelina SihombingNo ratings yet
- 1st Line Medication of An e CartDocument5 pages1st Line Medication of An e CartColette Marie PerezNo ratings yet
- Pediatric Status Epilepticus Pathway-FINALDocument5 pagesPediatric Status Epilepticus Pathway-FINALvural kesikNo ratings yet
- Case PBL Icm II Week 6 MondayDocument4 pagesCase PBL Icm II Week 6 MondayRaqqi PujatmikoNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- Status Epilepticus: Susilo SiswonotoDocument14 pagesStatus Epilepticus: Susilo SiswonotoAhmad Shafwan NatsirNo ratings yet
- Status EpilepticusDocument43 pagesStatus EpilepticusPatsuda DreematurakulNo ratings yet
- Convulsion, Spasm and UnconsciousnessDocument19 pagesConvulsion, Spasm and UnconsciousnessDesima Tamara sinuratNo ratings yet
- Convulsion, Spasm and UnconsciousnessDocument19 pagesConvulsion, Spasm and UnconsciousnessJoko Pratama AtmayudhaNo ratings yet
- Paediatric Clinical GuidelinesDocument7 pagesPaediatric Clinical GuidelinesAndriNo ratings yet
- ConnectorDocument4 pagesConnectoryetaung8No ratings yet
- Treatment Protocol of SnakebiteDocument23 pagesTreatment Protocol of SnakebiteEduconsultNo ratings yet
- Crisis ConvulsivaDocument3 pagesCrisis ConvulsivaJosé Victor Velez DelgadoNo ratings yet
- 7698alorithm SeizureDocument3 pages7698alorithm Seizureboromeus abyasa daniswara100% (1)
- Febrile Seizures: Status EpilepticusDocument34 pagesFebrile Seizures: Status EpilepticusSAIMA BATOOLNo ratings yet
- UNIT: Internal Medicine REG NO.: BMS/2014/72732 DATE: 30/7/2021 ASSIGNMENT: Status EpilepticusDocument10 pagesUNIT: Internal Medicine REG NO.: BMS/2014/72732 DATE: 30/7/2021 ASSIGNMENT: Status EpilepticusGladys MainaNo ratings yet
- Status EpilepticusDocument42 pagesStatus EpilepticusJesse EstradaNo ratings yet
- Approach and Management of Neonatal SeizuresDocument42 pagesApproach and Management of Neonatal SeizuresG Venkatesh100% (1)
- O&G Off-Tag Assesment Logbook: Traces-Pdf-248732173Document9 pagesO&G Off-Tag Assesment Logbook: Traces-Pdf-248732173niwasNo ratings yet
- Treatment of Prolonged SeizuresDocument1 pageTreatment of Prolonged SeizuresAhmad ShukriNo ratings yet
- Lec 4 CNSDocument12 pagesLec 4 CNShusainozelNo ratings yet
- Status Epilepticus: DR Abdelmoniem SaeedDocument24 pagesStatus Epilepticus: DR Abdelmoniem SaeedYousef Al-AmeenNo ratings yet
- Status Epilepticus: BY DR Muhammad Usman DR Areeba NaeemDocument16 pagesStatus Epilepticus: BY DR Muhammad Usman DR Areeba NaeemFarhan AfzalNo ratings yet
- Neurological EmergenciesDocument47 pagesNeurological EmergenciesStellate Repentance100% (1)
- Case Study Assignment On Open Cholecystectomy - MoodleDocument2 pagesCase Study Assignment On Open Cholecystectomy - MoodleHouda HayekNo ratings yet
- Pediatric Status Epilepticus CPGDocument3 pagesPediatric Status Epilepticus CPGAlex GasnasNo ratings yet
- Diabetic Foot Case PresentationDocument58 pagesDiabetic Foot Case PresentationZH. omg sarNo ratings yet
- Management of Eclampsia and Magnesium ToxicityDocument34 pagesManagement of Eclampsia and Magnesium ToxicityRezki IsharNo ratings yet
- Status EpilepsiDocument11 pagesStatus EpilepsiNurul aulia AbdullahNo ratings yet
- Approach To Status EpilepticusDocument21 pagesApproach To Status EpilepticusRoopam OjhaNo ratings yet
- Neonatal Seizures and Management: Dhaka Sishu Hospital BangladeshDocument19 pagesNeonatal Seizures and Management: Dhaka Sishu Hospital BangladeshGoha BashaNo ratings yet
- ENLS Status Epilepticus ProtocolDocument12 pagesENLS Status Epilepticus ProtocolFransiskus MikaelNo ratings yet
- Epilepsy/ Seizures: Commonest Neurological DisorderDocument25 pagesEpilepsy/ Seizures: Commonest Neurological DisorderAlokh Saha RajNo ratings yet
- Approach in Children With SeizuresDocument26 pagesApproach in Children With SeizuresMD Luthfy LubisNo ratings yet
- Eclampsia-Icu Management ProtocolDocument3 pagesEclampsia-Icu Management ProtocolmatentenNo ratings yet
- Malignan HipertermiaDocument10 pagesMalignan HipertermiaAstrid Ghea GayatriNo ratings yet
- Management of EclampsiaDocument24 pagesManagement of EclampsiaDup SuNo ratings yet
- Obat-Obat Emergency: DR T. Mamfaluti, SPPDDocument36 pagesObat-Obat Emergency: DR T. Mamfaluti, SPPDIqbal AminNo ratings yet
- Management of Hypertensive EmergencyDocument35 pagesManagement of Hypertensive EmergencyRaditya Indah TofaniNo ratings yet
- Seminar On SEDocument49 pagesSeminar On SEmubarak abdulkadirNo ratings yet
- Status Epileptic UsDocument66 pagesStatus Epileptic UsHakimah K. SuhaimiNo ratings yet
- Advanced Cardiac Life Support PDFDocument9 pagesAdvanced Cardiac Life Support PDFYulias YoweiNo ratings yet
- Management of Severe Hypertension, Hypertension in Special ConditionDocument43 pagesManagement of Severe Hypertension, Hypertension in Special Conditionabhandlung100% (3)
- Status Epilepticus and Its Management AssignmentDocument11 pagesStatus Epilepticus and Its Management AssignmentStanley KarugaNo ratings yet
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Fast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteFrom EverandFast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteNo ratings yet
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Vertigo, A Simple Guide to The Condition, Treatment And Related ConditionsFrom EverandVertigo, A Simple Guide to The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Biopharmaceutics-RED PACOPDocument588 pagesBiopharmaceutics-RED PACOPArk Olfato ParojinogNo ratings yet
- Aspirin and Salicylates: SourcesDocument3 pagesAspirin and Salicylates: SourcesahmedNo ratings yet
- Compliled DrugstudyDocument15 pagesCompliled DrugstudyApril Jan D. Alagon0% (1)
- Running Head: Pharmacology 1Document5 pagesRunning Head: Pharmacology 1jacobNo ratings yet
- Price List Generik PT Bernofarm Per 18 April THN 2011Document3 pagesPrice List Generik PT Bernofarm Per 18 April THN 2011Mandha UmamiiNo ratings yet
- Menghitung DosisDocument17 pagesMenghitung Dosisbaekhyunwoo1010No ratings yet
- Vere Labs: VL-Delta 8 THC Cartridge 1Document1 pageVere Labs: VL-Delta 8 THC Cartridge 1Michael WalkerNo ratings yet
- KlienDocument47 pagesKlientareq.sefatNo ratings yet
- HCG - Human Chorionic GonadotropinDocument2 pagesHCG - Human Chorionic GonadotropinOvidiu IgnatNo ratings yet
- BPL Annual 2019 20Document192 pagesBPL Annual 2019 20Ehsan Ul Karim Aonkon (181011286)No ratings yet
- PT - Permata Delta Agung: Halaman: (All)Document35 pagesPT - Permata Delta Agung: Halaman: (All)abdul husainNo ratings yet
- PRELIM EXAM - International BusinessDocument4 pagesPRELIM EXAM - International BusinessVel JuneNo ratings yet
- DRUG STUDY-Magnesium SulfateDocument2 pagesDRUG STUDY-Magnesium SulfateCarissa Mae Tapec Estrada80% (5)
- Immunization Training GuideDocument91 pagesImmunization Training Guidezenagit123456100% (1)
- Original Article: AbstractDocument4 pagesOriginal Article: AbstractAndikaPratamaPutraNo ratings yet
- Appropriateness For Ldts Companion DX Assays: Perspectives On To Be Used AsDocument16 pagesAppropriateness For Ldts Companion DX Assays: Perspectives On To Be Used AsfdablogNo ratings yet
- Apotik ApotikDocument66 pagesApotik Apotikdessy wilantariNo ratings yet
- 50 Most Commonly Used DrugsDocument1 page50 Most Commonly Used DrugsElizabeth uNo ratings yet
- Thrombolytics & Anti Platelet DrugsDocument38 pagesThrombolytics & Anti Platelet DrugsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- CiprofloxacinDocument6 pagesCiprofloxacinNasser AlhajjNo ratings yet
- Drugalertnov 23Document14 pagesDrugalertnov 23rashidhasan2001No ratings yet
- Rapid Tranquillisation Training PresentationDocument42 pagesRapid Tranquillisation Training PresentationmindpinkNo ratings yet
- Daftar Inventaris ApotekDocument3 pagesDaftar Inventaris ApotekMei Kurniawati TaharaNo ratings yet
- Ospolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)Document7 pagesOspolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)ddandan_2No ratings yet
- Pharmacology ReviewDocument64 pagesPharmacology ReviewRichard BakerNo ratings yet
- Anaesthetic Drug Crib Sheet-8 PDFDocument1 pageAnaesthetic Drug Crib Sheet-8 PDFKevin Ariel Tiopan SimanjuntakNo ratings yet
- Contoh Form ChecklistDocument39 pagesContoh Form ChecklistYastika YarsalNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka: Medicinal Chemistry - I Q.P. CODE: 5014Document1 pageRajiv Gandhi University of Health Sciences, Karnataka: Medicinal Chemistry - I Q.P. CODE: 5014Monica100% (1)