
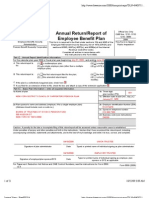
US Internal Revenue Service: f5500 - 2001
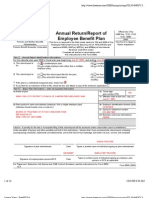
US Internal Revenue Service: f5500 - 2001
You might also like
- Best Buy Order DetailsDocument2 pagesBest Buy Order DetailsWilliams Jones100% (1)
- Netflix 401 (K) PlanDocument51 pagesNetflix 401 (K) PlanoaifoiweuNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Ch. 02 Bank Reconciliation Intermediate Accounting Volume 1 2021 Edition ValixDocument7 pagesCh. 02 Bank Reconciliation Intermediate Accounting Volume 1 2021 Edition ValixNathalie GetinoNo ratings yet
- Mercury NewsDocument87 pagesMercury NewskmccoynycNo ratings yet
- Tratamentul Total Al CanceruluiDocument71 pagesTratamentul Total Al CanceruluiAntal98% (98)
- Logo Brand BSIDocument16 pagesLogo Brand BSIDicky Riskiawan0% (1)
- US Internal Revenue Service: f5500 - 2002Document6 pagesUS Internal Revenue Service: f5500 - 2002IRSNo ratings yet
- Retirement & Pension Plan For NYCDCC Employees 2006Document13 pagesRetirement & Pension Plan For NYCDCC Employees 2006Latisha WalkerNo ratings yet
- Carpenters Annuity Fund 2007Document19 pagesCarpenters Annuity Fund 2007Latisha WalkerNo ratings yet
- Carpenters Annuity Fund 2006Document20 pagesCarpenters Annuity Fund 2006Latisha WalkerNo ratings yet
- Retirement & Pension Plan For NYCDCC Employees 2007Document13 pagesRetirement & Pension Plan For NYCDCC Employees 2007Latisha WalkerNo ratings yet
- 2006 Form 5500 Carpenter Pension PlanDocument22 pages2006 Form 5500 Carpenter Pension PlanLatisha WalkerNo ratings yet
- Retirement Plan of Trustees 2007Document14 pagesRetirement Plan of Trustees 2007Latisha WalkerNo ratings yet
- 2007 Form 5500 Carpenter Pension PlanDocument21 pages2007 Form 5500 Carpenter Pension PlanLatisha WalkerNo ratings yet
- Carpenters Welfare Fund 2006Document16 pagesCarpenters Welfare Fund 2006Latisha WalkerNo ratings yet
- Carpenters Welfare Fund 2007Document18 pagesCarpenters Welfare Fund 2007Latisha WalkerNo ratings yet
- Carpenters Vacation Fund 2007Document8 pagesCarpenters Vacation Fund 2007Latisha WalkerNo ratings yet
- Carpenters Vacation Fund 2006Document14 pagesCarpenters Vacation Fund 2006Latisha WalkerNo ratings yet
- Union Security Trust Fund 2007Document10 pagesUnion Security Trust Fund 2007Latisha WalkerNo ratings yet
- US Internal Revenue Service: f5500sb - 1999Document8 pagesUS Internal Revenue Service: f5500sb - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sb - 2003Document7 pagesUS Internal Revenue Service: f5500sb - 2003IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 1999Document2 pagesUS Internal Revenue Service: f5500sr - 1999IRSNo ratings yet
- Retirement Plan of Trustees 2006Document13 pagesRetirement Plan of Trustees 2006Latisha WalkerNo ratings yet
- Filing PDFDocument82 pagesFiling PDFjgalenNo ratings yet
- Attention:: WWW - Efast.dol - GovDocument4 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- Form 5500 Annual Return/Report of Employee Benefit Plan: X X X X X X X X X X X XDocument12 pagesForm 5500 Annual Return/Report of Employee Benefit Plan: X X X X X X X X X X X XkmccoynycNo ratings yet
- NRA 2015 Defined Benefit Plan 5500Document19 pagesNRA 2015 Defined Benefit Plan 5500jpeppardNo ratings yet
- US Internal Revenue Service: f5500st - 1999Document2 pagesUS Internal Revenue Service: f5500st - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 2000Document2 pagesUS Internal Revenue Service: f5500sr - 2000IRSNo ratings yet
- US Internal Revenue Service: f5500 - 1995Document6 pagesUS Internal Revenue Service: f5500 - 1995IRSNo ratings yet
- US Internal Revenue Service: f5500 - 1991Document6 pagesUS Internal Revenue Service: f5500 - 1991IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 2001Document2 pagesUS Internal Revenue Service: f5500sr - 2001IRSNo ratings yet
- Union Security Trust Fund 2006Document10 pagesUnion Security Trust Fund 2006Latisha WalkerNo ratings yet
- NRA 2016 401 (K) - Form 5500Document15 pagesNRA 2016 401 (K) - Form 5500jpeppardNo ratings yet
- US Internal Revenue Service: f5500sf - 1999Document1 pageUS Internal Revenue Service: f5500sf - 1999IRSNo ratings yet
- 20240429132130NAL0014058224001Document10 pages20240429132130NAL0014058224001Sherloc HolmesNo ratings yet
- Nal 0027478945001Document7 pagesNal 0027478945001firedancer1943No ratings yet
- DOL RDWSU 2020 Form 5500Document205 pagesDOL RDWSU 2020 Form 5500seanredmondNo ratings yet
- NRA Defined Benefit Plan - 2016 5500Document26 pagesNRA Defined Benefit Plan - 2016 5500jpeppardNo ratings yet
- Pension PlanDocument49 pagesPension PlanPriscilla TranNo ratings yet
- Form 5500-SF 2017: Short Form Annual Return/Report of Small Employee Benefit PlanDocument3 pagesForm 5500-SF 2017: Short Form Annual Return/Report of Small Employee Benefit PlanoaifoiweuNo ratings yet
- US Internal Revenue Service: f5500 - 1994Document6 pagesUS Internal Revenue Service: f5500 - 1994IRSNo ratings yet
- US Internal Revenue Service: F5500si - 2002Document6 pagesUS Internal Revenue Service: F5500si - 2002IRSNo ratings yet
- US Internal Revenue Service: f5500cr - 1995Document6 pagesUS Internal Revenue Service: f5500cr - 1995IRSNo ratings yet
- Attention:: WWW - Efast.dol - GovDocument7 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- US Internal Revenue Service: f5500 - 1996Document6 pagesUS Internal Revenue Service: f5500 - 1996IRSNo ratings yet
- US Internal Revenue Service: f5500cr - 1991Document6 pagesUS Internal Revenue Service: f5500cr - 1991IRSNo ratings yet
- Attention:: WWW - Efast.dol - GovDocument4 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- US Internal Revenue Service: f5500cr - 1997Document6 pagesUS Internal Revenue Service: f5500cr - 1997IRSNo ratings yet
- US Internal Revenue Service: F5500se - 1999Document3 pagesUS Internal Revenue Service: F5500se - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 2003Document2 pagesUS Internal Revenue Service: f5500sr - 2003IRSNo ratings yet
- US Internal Revenue Service: f5500sp - 2000Document1 pageUS Internal Revenue Service: f5500sp - 2000IRSNo ratings yet
- US Internal Revenue Service: f5500sp - 1991Document1 pageUS Internal Revenue Service: f5500sp - 1991IRSNo ratings yet
- US Internal Revenue Service: f5500sp - 1999Document1 pageUS Internal Revenue Service: f5500sp - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sf - 1997Document1 pageUS Internal Revenue Service: f5500sf - 1997IRSNo ratings yet
- US Internal Revenue Service: f5500cr - 1994Document6 pagesUS Internal Revenue Service: f5500cr - 1994IRSNo ratings yet
- US Internal Revenue Service: F8453e - 1994Document2 pagesUS Internal Revenue Service: F8453e - 1994IRSNo ratings yet
- US Internal Revenue Service: I5500sp - 2003Document1 pageUS Internal Revenue Service: I5500sp - 2003IRSNo ratings yet
- US Internal Revenue Service: f5500sf - 1993Document1 pageUS Internal Revenue Service: f5500sf - 1993IRSNo ratings yet
- US Internal Revenue Service: F5500ssa - 1999Document2 pagesUS Internal Revenue Service: F5500ssa - 1999IRSNo ratings yet
- US Internal Revenue Service: F5500si - 2003Document3 pagesUS Internal Revenue Service: F5500si - 2003IRSNo ratings yet
- US Internal Revenue Service: f5500sb - 1994Document3 pagesUS Internal Revenue Service: f5500sb - 1994IRSNo ratings yet
- Form 5500 Employee Benefit Plan AuditsDocument13 pagesForm 5500 Employee Benefit Plan AuditsCA Rajendra Prasad ANo ratings yet
- US Internal Revenue Service: 2290rulesty2007v4 0Document6 pagesUS Internal Revenue Service: 2290rulesty2007v4 0IRSNo ratings yet
- 2008 Objectives Report To Congress v2Document153 pages2008 Objectives Report To Congress v2IRSNo ratings yet
- 2008 Data DictionaryDocument260 pages2008 Data DictionaryIRSNo ratings yet
- 2008 Credit Card Bulk Provider RequirementsDocument112 pages2008 Credit Card Bulk Provider RequirementsIRSNo ratings yet
- Account Statement From 3 Jan 2020 To 26 Feb 2020: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceDocument2 pagesAccount Statement From 3 Jan 2020 To 26 Feb 2020: TXN Date Value Date Description Ref No./Cheque No. Debit Credit Balancebhairav ghimireNo ratings yet
- 12 02 20Document47 pages12 02 20Rommel John SandovalNo ratings yet
- Tax Ii NotesDocument40 pagesTax Ii NotesMARFENo ratings yet
- Estmt - 2021 08 27Document6 pagesEstmt - 2021 08 27Andrea IñiguezNo ratings yet
- Attachment PAYMENT AND SETTLEMENT SYSTEM ACT 2007 Lyst8740Document10 pagesAttachment PAYMENT AND SETTLEMENT SYSTEM ACT 2007 Lyst8740Vaishali SinghNo ratings yet
- Deposit Confirmation/Renewal AdviceDocument1 pageDeposit Confirmation/Renewal AdviceTuhin ChakrabortyNo ratings yet
- Payment Acknowledgement Payment Acknowledgement: PrintDocument1 pagePayment Acknowledgement Payment Acknowledgement: PrintS KkNo ratings yet
- CHALLAN FORM No.32 ADocument3 pagesCHALLAN FORM No.32 AMIan Muzamil0% (1)
- Cma Inter GR 1 Financial Accounting Ebook June 2021 OnwardsDocument358 pagesCma Inter GR 1 Financial Accounting Ebook June 2021 OnwardsSarath KumarNo ratings yet
- Quantity Description Category Weight (LB) Length (CM) Width (CM) Height (CM) Weight Vol. (LB)Document1 pageQuantity Description Category Weight (LB) Length (CM) Width (CM) Height (CM) Weight Vol. (LB)Ardiyansyah NugrahaNo ratings yet
- MC 3 Topic 4 Def Tax Question A232Document4 pagesMC 3 Topic 4 Def Tax Question A232thanusri0103No ratings yet
- Capital GainDocument4 pagesCapital GainqwertyNo ratings yet
- True False False True True True False True True True True True True True True True True False False True True True False True TrueDocument5 pagesTrue False False True True True False True True True True True True True True True True False False True True True False True TrueDong RoselloNo ratings yet
- Final-General Banking .Document27 pagesFinal-General Banking .Salman AhmedNo ratings yet
- Financial Crimes - ACC 404 Fraud Examination - 19 October 2021Document98 pagesFinancial Crimes - ACC 404 Fraud Examination - 19 October 2021Bernadette Ruiz AlbinoNo ratings yet
- Bahasa Inggris HukumDocument9 pagesBahasa Inggris HukumlorensiusNo ratings yet
- Salem Five Direct Consumer Banking Fee ScheduleDocument2 pagesSalem Five Direct Consumer Banking Fee ScheduleshoppingonlyNo ratings yet
- Gasbill 4978636878 202007 20200714214937Document1 pageGasbill 4978636878 202007 20200714214937salmansaleemNo ratings yet
- Climax TextDocument2 pagesClimax TextRajkumarNo ratings yet
- HRA Form (Revised)Document1 pageHRA Form (Revised)Arunabha_GNo ratings yet
- Reliance Retail Limited: Sr. No. Item Name Hsn/Sac Qty Price/Unit Discount ValueDocument3 pagesReliance Retail Limited: Sr. No. Item Name Hsn/Sac Qty Price/Unit Discount ValuemukeshNo ratings yet
- Settlement Instruction: 账户名称 Account Name: 账户号码 Account No.Document1 pageSettlement Instruction: 账户名称 Account Name: 账户号码 Account No.thitijv6048No ratings yet
- Invoice 5314971552Document2 pagesInvoice 5314971552sumankrbiswas8No ratings yet
- Chapter-11 Compound InterestDocument25 pagesChapter-11 Compound InterestscihimaNo ratings yet
- Chapter 3 AccountingDocument11 pagesChapter 3 AccountingĐỗ ĐăngNo ratings yet
- May 2018 SGV SDGSDDocument26 pagesMay 2018 SGV SDGSDBien Bowie A. CortezNo ratings yet
- Account Statement: NSDL Payments BankDocument3 pagesAccount Statement: NSDL Payments BankPUNAM DEVINo ratings yet

























































































Download as pdf or txt
You might also like
- Best Buy Order DetailsDocument2 pagesBest Buy Order DetailsWilliams Jones100% (1)
- Netflix 401 (K) PlanDocument51 pagesNetflix 401 (K) PlanoaifoiweuNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Ch. 02 Bank Reconciliation Intermediate Accounting Volume 1 2021 Edition ValixDocument7 pagesCh. 02 Bank Reconciliation Intermediate Accounting Volume 1 2021 Edition ValixNathalie GetinoNo ratings yet
- Mercury NewsDocument87 pagesMercury NewskmccoynycNo ratings yet
- Tratamentul Total Al CanceruluiDocument71 pagesTratamentul Total Al CanceruluiAntal98% (98)
- Logo Brand BSIDocument16 pagesLogo Brand BSIDicky Riskiawan0% (1)
- US Internal Revenue Service: f5500 - 2002Document6 pagesUS Internal Revenue Service: f5500 - 2002IRSNo ratings yet
- Retirement & Pension Plan For NYCDCC Employees 2006Document13 pagesRetirement & Pension Plan For NYCDCC Employees 2006Latisha WalkerNo ratings yet
- Carpenters Annuity Fund 2007Document19 pagesCarpenters Annuity Fund 2007Latisha WalkerNo ratings yet
- Carpenters Annuity Fund 2006Document20 pagesCarpenters Annuity Fund 2006Latisha WalkerNo ratings yet
- Retirement & Pension Plan For NYCDCC Employees 2007Document13 pagesRetirement & Pension Plan For NYCDCC Employees 2007Latisha WalkerNo ratings yet
- 2006 Form 5500 Carpenter Pension PlanDocument22 pages2006 Form 5500 Carpenter Pension PlanLatisha WalkerNo ratings yet
- Retirement Plan of Trustees 2007Document14 pagesRetirement Plan of Trustees 2007Latisha WalkerNo ratings yet
- 2007 Form 5500 Carpenter Pension PlanDocument21 pages2007 Form 5500 Carpenter Pension PlanLatisha WalkerNo ratings yet
- Carpenters Welfare Fund 2006Document16 pagesCarpenters Welfare Fund 2006Latisha WalkerNo ratings yet
- Carpenters Welfare Fund 2007Document18 pagesCarpenters Welfare Fund 2007Latisha WalkerNo ratings yet
- Carpenters Vacation Fund 2007Document8 pagesCarpenters Vacation Fund 2007Latisha WalkerNo ratings yet
- Carpenters Vacation Fund 2006Document14 pagesCarpenters Vacation Fund 2006Latisha WalkerNo ratings yet
- Union Security Trust Fund 2007Document10 pagesUnion Security Trust Fund 2007Latisha WalkerNo ratings yet
- US Internal Revenue Service: f5500sb - 1999Document8 pagesUS Internal Revenue Service: f5500sb - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sb - 2003Document7 pagesUS Internal Revenue Service: f5500sb - 2003IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 1999Document2 pagesUS Internal Revenue Service: f5500sr - 1999IRSNo ratings yet
- Retirement Plan of Trustees 2006Document13 pagesRetirement Plan of Trustees 2006Latisha WalkerNo ratings yet
- Filing PDFDocument82 pagesFiling PDFjgalenNo ratings yet
- Attention:: WWW - Efast.dol - GovDocument4 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- Form 5500 Annual Return/Report of Employee Benefit Plan: X X X X X X X X X X X XDocument12 pagesForm 5500 Annual Return/Report of Employee Benefit Plan: X X X X X X X X X X X XkmccoynycNo ratings yet
- NRA 2015 Defined Benefit Plan 5500Document19 pagesNRA 2015 Defined Benefit Plan 5500jpeppardNo ratings yet
- US Internal Revenue Service: f5500st - 1999Document2 pagesUS Internal Revenue Service: f5500st - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 2000Document2 pagesUS Internal Revenue Service: f5500sr - 2000IRSNo ratings yet
- US Internal Revenue Service: f5500 - 1995Document6 pagesUS Internal Revenue Service: f5500 - 1995IRSNo ratings yet
- US Internal Revenue Service: f5500 - 1991Document6 pagesUS Internal Revenue Service: f5500 - 1991IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 2001Document2 pagesUS Internal Revenue Service: f5500sr - 2001IRSNo ratings yet
- Union Security Trust Fund 2006Document10 pagesUnion Security Trust Fund 2006Latisha WalkerNo ratings yet
- NRA 2016 401 (K) - Form 5500Document15 pagesNRA 2016 401 (K) - Form 5500jpeppardNo ratings yet
- US Internal Revenue Service: f5500sf - 1999Document1 pageUS Internal Revenue Service: f5500sf - 1999IRSNo ratings yet
- 20240429132130NAL0014058224001Document10 pages20240429132130NAL0014058224001Sherloc HolmesNo ratings yet
- Nal 0027478945001Document7 pagesNal 0027478945001firedancer1943No ratings yet
- DOL RDWSU 2020 Form 5500Document205 pagesDOL RDWSU 2020 Form 5500seanredmondNo ratings yet
- NRA Defined Benefit Plan - 2016 5500Document26 pagesNRA Defined Benefit Plan - 2016 5500jpeppardNo ratings yet
- Pension PlanDocument49 pagesPension PlanPriscilla TranNo ratings yet
- Form 5500-SF 2017: Short Form Annual Return/Report of Small Employee Benefit PlanDocument3 pagesForm 5500-SF 2017: Short Form Annual Return/Report of Small Employee Benefit PlanoaifoiweuNo ratings yet
- US Internal Revenue Service: f5500 - 1994Document6 pagesUS Internal Revenue Service: f5500 - 1994IRSNo ratings yet
- US Internal Revenue Service: F5500si - 2002Document6 pagesUS Internal Revenue Service: F5500si - 2002IRSNo ratings yet
- US Internal Revenue Service: f5500cr - 1995Document6 pagesUS Internal Revenue Service: f5500cr - 1995IRSNo ratings yet
- Attention:: WWW - Efast.dol - GovDocument7 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- US Internal Revenue Service: f5500 - 1996Document6 pagesUS Internal Revenue Service: f5500 - 1996IRSNo ratings yet
- US Internal Revenue Service: f5500cr - 1991Document6 pagesUS Internal Revenue Service: f5500cr - 1991IRSNo ratings yet
- Attention:: WWW - Efast.dol - GovDocument4 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- US Internal Revenue Service: f5500cr - 1997Document6 pagesUS Internal Revenue Service: f5500cr - 1997IRSNo ratings yet
- US Internal Revenue Service: F5500se - 1999Document3 pagesUS Internal Revenue Service: F5500se - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 2003Document2 pagesUS Internal Revenue Service: f5500sr - 2003IRSNo ratings yet
- US Internal Revenue Service: f5500sp - 2000Document1 pageUS Internal Revenue Service: f5500sp - 2000IRSNo ratings yet
- US Internal Revenue Service: f5500sp - 1991Document1 pageUS Internal Revenue Service: f5500sp - 1991IRSNo ratings yet
- US Internal Revenue Service: f5500sp - 1999Document1 pageUS Internal Revenue Service: f5500sp - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sf - 1997Document1 pageUS Internal Revenue Service: f5500sf - 1997IRSNo ratings yet
- US Internal Revenue Service: f5500cr - 1994Document6 pagesUS Internal Revenue Service: f5500cr - 1994IRSNo ratings yet
- US Internal Revenue Service: F8453e - 1994Document2 pagesUS Internal Revenue Service: F8453e - 1994IRSNo ratings yet
- US Internal Revenue Service: I5500sp - 2003Document1 pageUS Internal Revenue Service: I5500sp - 2003IRSNo ratings yet
- US Internal Revenue Service: f5500sf - 1993Document1 pageUS Internal Revenue Service: f5500sf - 1993IRSNo ratings yet
- US Internal Revenue Service: F5500ssa - 1999Document2 pagesUS Internal Revenue Service: F5500ssa - 1999IRSNo ratings yet
- US Internal Revenue Service: F5500si - 2003Document3 pagesUS Internal Revenue Service: F5500si - 2003IRSNo ratings yet
- US Internal Revenue Service: f5500sb - 1994Document3 pagesUS Internal Revenue Service: f5500sb - 1994IRSNo ratings yet
- Form 5500 Employee Benefit Plan AuditsDocument13 pagesForm 5500 Employee Benefit Plan AuditsCA Rajendra Prasad ANo ratings yet
- US Internal Revenue Service: 2290rulesty2007v4 0Document6 pagesUS Internal Revenue Service: 2290rulesty2007v4 0IRSNo ratings yet
- 2008 Objectives Report To Congress v2Document153 pages2008 Objectives Report To Congress v2IRSNo ratings yet
- 2008 Data DictionaryDocument260 pages2008 Data DictionaryIRSNo ratings yet
- 2008 Credit Card Bulk Provider RequirementsDocument112 pages2008 Credit Card Bulk Provider RequirementsIRSNo ratings yet
- Account Statement From 3 Jan 2020 To 26 Feb 2020: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceDocument2 pagesAccount Statement From 3 Jan 2020 To 26 Feb 2020: TXN Date Value Date Description Ref No./Cheque No. Debit Credit Balancebhairav ghimireNo ratings yet
- 12 02 20Document47 pages12 02 20Rommel John SandovalNo ratings yet
- Tax Ii NotesDocument40 pagesTax Ii NotesMARFENo ratings yet
- Estmt - 2021 08 27Document6 pagesEstmt - 2021 08 27Andrea IñiguezNo ratings yet
- Attachment PAYMENT AND SETTLEMENT SYSTEM ACT 2007 Lyst8740Document10 pagesAttachment PAYMENT AND SETTLEMENT SYSTEM ACT 2007 Lyst8740Vaishali SinghNo ratings yet
- Deposit Confirmation/Renewal AdviceDocument1 pageDeposit Confirmation/Renewal AdviceTuhin ChakrabortyNo ratings yet
- Payment Acknowledgement Payment Acknowledgement: PrintDocument1 pagePayment Acknowledgement Payment Acknowledgement: PrintS KkNo ratings yet
- CHALLAN FORM No.32 ADocument3 pagesCHALLAN FORM No.32 AMIan Muzamil0% (1)
- Cma Inter GR 1 Financial Accounting Ebook June 2021 OnwardsDocument358 pagesCma Inter GR 1 Financial Accounting Ebook June 2021 OnwardsSarath KumarNo ratings yet
- Quantity Description Category Weight (LB) Length (CM) Width (CM) Height (CM) Weight Vol. (LB)Document1 pageQuantity Description Category Weight (LB) Length (CM) Width (CM) Height (CM) Weight Vol. (LB)Ardiyansyah NugrahaNo ratings yet
- MC 3 Topic 4 Def Tax Question A232Document4 pagesMC 3 Topic 4 Def Tax Question A232thanusri0103No ratings yet
- Capital GainDocument4 pagesCapital GainqwertyNo ratings yet
- True False False True True True False True True True True True True True True True True False False True True True False True TrueDocument5 pagesTrue False False True True True False True True True True True True True True True True False False True True True False True TrueDong RoselloNo ratings yet
- Final-General Banking .Document27 pagesFinal-General Banking .Salman AhmedNo ratings yet
- Financial Crimes - ACC 404 Fraud Examination - 19 October 2021Document98 pagesFinancial Crimes - ACC 404 Fraud Examination - 19 October 2021Bernadette Ruiz AlbinoNo ratings yet
- Bahasa Inggris HukumDocument9 pagesBahasa Inggris HukumlorensiusNo ratings yet
- Salem Five Direct Consumer Banking Fee ScheduleDocument2 pagesSalem Five Direct Consumer Banking Fee ScheduleshoppingonlyNo ratings yet
- Gasbill 4978636878 202007 20200714214937Document1 pageGasbill 4978636878 202007 20200714214937salmansaleemNo ratings yet
- Climax TextDocument2 pagesClimax TextRajkumarNo ratings yet
- HRA Form (Revised)Document1 pageHRA Form (Revised)Arunabha_GNo ratings yet
- Reliance Retail Limited: Sr. No. Item Name Hsn/Sac Qty Price/Unit Discount ValueDocument3 pagesReliance Retail Limited: Sr. No. Item Name Hsn/Sac Qty Price/Unit Discount ValuemukeshNo ratings yet
- Settlement Instruction: 账户名称 Account Name: 账户号码 Account No.Document1 pageSettlement Instruction: 账户名称 Account Name: 账户号码 Account No.thitijv6048No ratings yet
- Invoice 5314971552Document2 pagesInvoice 5314971552sumankrbiswas8No ratings yet
- Chapter-11 Compound InterestDocument25 pagesChapter-11 Compound InterestscihimaNo ratings yet
- Chapter 3 AccountingDocument11 pagesChapter 3 AccountingĐỗ ĐăngNo ratings yet
- May 2018 SGV SDGSDDocument26 pagesMay 2018 SGV SDGSDBien Bowie A. CortezNo ratings yet
- Account Statement: NSDL Payments BankDocument3 pagesAccount Statement: NSDL Payments BankPUNAM DEVINo ratings yet