
Circulationaha 105 597500
Circulationaha 105 597500
You might also like
- Reading: Healthy Lifestyle Role For All Society'Document4 pagesReading: Healthy Lifestyle Role For All Society'Tore CusimanoNo ratings yet
- Jaha 116 003196Document9 pagesJaha 116 003196Omar Nassir MoftahNo ratings yet
- Groenendaal Vandemeent2016Document11 pagesGroenendaal Vandemeent2016Soshi DaysNo ratings yet
- Management of Direct-Acting Oral Anticoagulants Surrounding Dental Procedures With Low-to-Moderate Risk of BleedingDocument6 pagesManagement of Direct-Acting Oral Anticoagulants Surrounding Dental Procedures With Low-to-Moderate Risk of BleedingOdontologia HmaspNo ratings yet
- S 025 LBLDocument16 pagesS 025 LBLarmanNo ratings yet
- Candesartan RBX PIDocument14 pagesCandesartan RBX PIshadab0123No ratings yet
- FAQ - FinerenoneDocument9 pagesFAQ - Finerenoneraea.dobsonNo ratings yet
- New Oral Anticoagulants A Practical Guide For PhysiciansDocument12 pagesNew Oral Anticoagulants A Practical Guide For PhysiciansSebastian PosadaNo ratings yet
- VorapaxarDocument21 pagesVorapaxarIoana GhirvuNo ratings yet
- Vorapaxar: General InformationDocument21 pagesVorapaxar: General InformationIoana GhirvuNo ratings yet
- Influence of Drugs Interacting With CYP3A4 On The Pharmacokinetics, Pharmacodynamics, and SafetyDocument13 pagesInfluence of Drugs Interacting With CYP3A4 On The Pharmacokinetics, Pharmacodynamics, and SafetyLuciana OliveiraNo ratings yet
- AlphaDocument6 pagesAlphaJoseph SantiagoNo ratings yet
- Ran Ola ZineDocument20 pagesRan Ola ZineHamza AlmaqtriNo ratings yet
- Warfarin Dan AspirinDocument10 pagesWarfarin Dan Aspirindita novia maharaniNo ratings yet
- Prevention of Gastrointestinal Bleeding in Patients Receiving Direct Oral Anticoagulants OpenDocument24 pagesPrevention of Gastrointestinal Bleeding in Patients Receiving Direct Oral Anticoagulants Openfitra annisaNo ratings yet
- An Open-Label, Phase 1 Study To Evaluate The Effects of Hepatic Impairment On Edoxaban Pharmacokinetics and PharmacodynamicsDocument11 pagesAn Open-Label, Phase 1 Study To Evaluate The Effects of Hepatic Impairment On Edoxaban Pharmacokinetics and PharmacodynamicsHendrawan RahmanNo ratings yet
- Nuevos anticoagulantes-BLOODDocument7 pagesNuevos anticoagulantes-BLOODnakroliNo ratings yet
- TrandolaprilDocument28 pagesTrandolaprilYeyenJaejoongNo ratings yet
- Anticoagulants TransaminasesDocument5 pagesAnticoagulants TransaminasesSony Eka NugrahaNo ratings yet
- Drugs and Renal DiseasesDocument31 pagesDrugs and Renal DiseasesStanley Tatenda MukonoNo ratings yet
- Notes 1Document24 pagesNotes 1coosa liquorsNo ratings yet
- MILsgsdgds VDocument4 pagesMILsgsdgds Vgarywall.ukNo ratings yet
- Telmisartan (Vaidyanathan)Document14 pagesTelmisartan (Vaidyanathan)Antonio SanchezNo ratings yet
- Penyesuaian Dosis Regimen Pada Pasien Dengan Gangguan Fungsi GinjalDocument19 pagesPenyesuaian Dosis Regimen Pada Pasien Dengan Gangguan Fungsi GinjalChamidRiyadiNo ratings yet
- Patisiran Pharmacokinetics, Pharmacodynamics, and Exposure-Response Analyses in The Phase 3 APOLLO Trial in Patients With Hereditary Transthyretin-Mediated (hATTR) AmyloidosisDocument13 pagesPatisiran Pharmacokinetics, Pharmacodynamics, and Exposure-Response Analyses in The Phase 3 APOLLO Trial in Patients With Hereditary Transthyretin-Mediated (hATTR) AmyloidosisMihaela BerindeieNo ratings yet
- HW3 PharmacologyDocument8 pagesHW3 PharmacologyMICHAEL GABRIEL JIMENEZNo ratings yet
- ACOS BloodDocument7 pagesACOS Bloodpablin1788No ratings yet
- Chandok Et Al, 2010Document8 pagesChandok Et Al, 2010Cika Zahrah DewisoniaNo ratings yet
- Newer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugDocument5 pagesNewer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugLouiseNo ratings yet
- Bleeding Is Out, Your Own Blood Is in 2014Document4 pagesBleeding Is Out, Your Own Blood Is in 2014viaereaNo ratings yet
- Lec - No.12 (Carbamazipine)Document13 pagesLec - No.12 (Carbamazipine)phd0780No ratings yet
- Pregabalin Hospital PharmacyDocument16 pagesPregabalin Hospital Pharmacyaditya100% (1)
- PIIS1053077018310437Document5 pagesPIIS1053077018310437andi rahmatNo ratings yet
- Farmako PDFDocument16 pagesFarmako PDFIsney HanindyaNo ratings yet
- CCO Pancreatic Advances PDFDocument4 pagesCCO Pancreatic Advances PDFSyedNo ratings yet
- Anticoag 2015november FullDocument14 pagesAnticoag 2015november FullRosanna FiorilloNo ratings yet
- Profil Farmakikinetik Pantoprazole InjeksiDocument17 pagesProfil Farmakikinetik Pantoprazole InjeksitikaNo ratings yet
- Prescribing in Patients With Liver Disease: Rakesh K TandonDocument4 pagesPrescribing in Patients With Liver Disease: Rakesh K Tandonjoydeep chakrabortyNo ratings yet
- Effect of Rivaroxaban Vs Enoxaparin On Major Cardiac Adverse Events and Bleeding Risk in The Acute Phase of Acute Coronary Syndrome PDFDocument13 pagesEffect of Rivaroxaban Vs Enoxaparin On Major Cardiac Adverse Events and Bleeding Risk in The Acute Phase of Acute Coronary Syndrome PDFKardiologi ManadoNo ratings yet
- JAPI0073 p84-88Document5 pagesJAPI0073 p84-88Subhashini KNo ratings yet
- Drugs and Kidney DiseasesDocument46 pagesDrugs and Kidney Diseasesمرتضى محمد فاضل جرجوكNo ratings yet
- CarvedilolDocument7 pagesCarvedilolHelen QuirogaNo ratings yet
- Mefenamic Acid Capsules, USP 250 MG RX Only: Reference ID: 3928117Document20 pagesMefenamic Acid Capsules, USP 250 MG RX Only: Reference ID: 3928117Riska AuliahNo ratings yet
- Neuro-Oncology PracticeDocument16 pagesNeuro-Oncology Practice6ydn87w6gpNo ratings yet
- Bipolar Disorders and Carbamazepine PharmacokinetiDocument5 pagesBipolar Disorders and Carbamazepine PharmacokinetiAgr YuroNo ratings yet
- Bipolar Disorders and Carbamazepine PharmacokinetiDocument6 pagesBipolar Disorders and Carbamazepine PharmacokinetiluthfiahNo ratings yet
- Procainamide Hydrochloride: Major UseDocument3 pagesProcainamide Hydrochloride: Major UseDosi SiliNo ratings yet
- Effect of Rosuvastatin On Warfarin Pharmacodynamics and PharmacokineticsDocument9 pagesEffect of Rosuvastatin On Warfarin Pharmacodynamics and PharmacokineticsLuciana OliveiraNo ratings yet
- Dacarbazine Monograph 1june2013 FormattedDocument7 pagesDacarbazine Monograph 1june2013 FormattedRobert ChristevenNo ratings yet
- Medi 95 E2881Document5 pagesMedi 95 E2881Betari YoscarNo ratings yet
- Randomized Controlled Clinical Trial of Corticosteroids Plus Ace-Inhibitors With Long-Term Follow-Up in Proteinuric Iga NephropathyDocument7 pagesRandomized Controlled Clinical Trial of Corticosteroids Plus Ace-Inhibitors With Long-Term Follow-Up in Proteinuric Iga Nephropathyguugle gogleNo ratings yet
- Lancet 2010 376 489Document2 pagesLancet 2010 376 489CClaaudianagoisNo ratings yet
- Novel Oral Anticoagulants in The Management of Coronary Artery DiseaseDocument8 pagesNovel Oral Anticoagulants in The Management of Coronary Artery DiseaseqiraniNo ratings yet
- Nateglinide Tablets: GeriatricDocument2 pagesNateglinide Tablets: GeriatricUlfa AlyaNo ratings yet
- Reemplazo de Cadera FrontalDocument10 pagesReemplazo de Cadera FrontalffffffffffffNo ratings yet
- Schizophr Bull 1998 Young 381 90Document10 pagesSchizophr Bull 1998 Young 381 90Kadelsy BristolNo ratings yet
- Putri RamadhanDocument44 pagesPutri RamadhanRama MulyadiNo ratings yet
- 949-Texto Del Artículo-7086-1-10-20231207Document8 pages949-Texto Del Artículo-7086-1-10-20231207mplp2721No ratings yet
- Hep 24519 PDFDocument5 pagesHep 24519 PDFLaras Bani WasesoNo ratings yet
- Diagnostic and Therapeutic Advances in Hepatology Terlipressin: An Asset For Hepatologists!Document5 pagesDiagnostic and Therapeutic Advances in Hepatology Terlipressin: An Asset For Hepatologists!Laras Bani WasesoNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Bmjopen 2018 026362Document7 pagesBmjopen 2018 026362Kevin HartonoNo ratings yet
- Journal Alergi Terhadap DepresiDocument31 pagesJournal Alergi Terhadap DepresiKevin HartonoNo ratings yet
- DermatitisDocument9 pagesDermatitisKevin HartonoNo ratings yet
- Biochemistry & Pharmacology: Open Access: The Morphine and Codeine Equianalgesic 'SDocument5 pagesBiochemistry & Pharmacology: Open Access: The Morphine and Codeine Equianalgesic 'SKevin HartonoNo ratings yet
- Review Current Concepts in The Pathogenesis and Treatment of Chronic Suppurative Otitis MediaDocument14 pagesReview Current Concepts in The Pathogenesis and Treatment of Chronic Suppurative Otitis MediaKevin HartonoNo ratings yet
- Final Presentation Journal OtitisDocument34 pagesFinal Presentation Journal OtitisKevin HartonoNo ratings yet
- RHU Situanional ReportDocument8 pagesRHU Situanional ReportErnest AtonNo ratings yet
- Evolution of Life On Earth: General Biology 2Document10 pagesEvolution of Life On Earth: General Biology 2Geox NikeeNo ratings yet
- Growth Evaluation and Meat Assessment of Native Pig in Romblon Province, PhilippinesDocument7 pagesGrowth Evaluation and Meat Assessment of Native Pig in Romblon Province, PhilippinesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
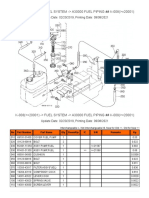
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- The Magic Mushroom Growers GuideDocument61 pagesThe Magic Mushroom Growers GuideDaniel Marsh83% (6)
- Leela Residences at Bhartiya City - Amenities: Common LobbyDocument4 pagesLeela Residences at Bhartiya City - Amenities: Common LobbyFrancis XavierNo ratings yet
- Perkins Spares 80,100Document10 pagesPerkins Spares 80,100ramsey222No ratings yet
- Fluor CarbonDocument3 pagesFluor CarbonHrishikesh DhawadshikarNo ratings yet
- Migraine DiaryDocument1 pageMigraine DiaryEmily KirbyNo ratings yet
- Activated Carbon From BambooDocument19 pagesActivated Carbon From BambooErik WeeksNo ratings yet
- Fresh and Simple PDFDocument3 pagesFresh and Simple PDFthivashnee padayacheeNo ratings yet
- Andovercontinuumul 864 Bacnetsmokecontrolsystemdesignguide 101134Document124 pagesAndovercontinuumul 864 Bacnetsmokecontrolsystemdesignguide 101134Chong CongNo ratings yet
- Chapter 21 Electric Charge - Gui SVDocument5 pagesChapter 21 Electric Charge - Gui SVHậu Vũ100% (1)
- Domestic Dogs: Temporal Range: at Least 14,200 Years Ago - PresentDocument35 pagesDomestic Dogs: Temporal Range: at Least 14,200 Years Ago - PresentirayoNo ratings yet
- Mass. Proposed AddendumsDocument25 pagesMass. Proposed AddendumsKirk HartleyNo ratings yet
- Raising Permit: Office of The Building OfficialDocument2 pagesRaising Permit: Office of The Building OfficialJc JüsäyänNo ratings yet
- Timing Protection in AUTOSAR ISO 26262Document10 pagesTiming Protection in AUTOSAR ISO 26262Joseph KymmNo ratings yet
- Zoology Mammals (Rabbit)Document3 pagesZoology Mammals (Rabbit)PerrieNo ratings yet
- Caring For Your African American/Biracial Child's HairDocument32 pagesCaring For Your African American/Biracial Child's Hair4kidslikemeNo ratings yet
- Pentavitin - DSMDocument3 pagesPentavitin - DSMRnD Roi SuryaNo ratings yet
- The Best Things To Do in Binghamton NYDocument4 pagesThe Best Things To Do in Binghamton NYShashank SangwanNo ratings yet
- Focus Level 3 Table of Contents PDFDocument2 pagesFocus Level 3 Table of Contents PDFDaria KudosLamNo ratings yet
- TirupathiDocument14 pagesTirupathiEkta Adlakha100% (1)
- String of Pearls Slide ShowDocument23 pagesString of Pearls Slide Showjimhtolbert434No ratings yet
- Beer & Wine Osd PresDocument18 pagesBeer & Wine Osd PresAnand100% (1)
- Nameplate PDFDocument8 pagesNameplate PDFobida adailehNo ratings yet
- Astrological Study of Infertility - ConclusionDocument9 pagesAstrological Study of Infertility - ConclusionAnamika SNo ratings yet
- Essay C DraftDocument7 pagesEssay C Draftapi-242837115No ratings yet
- The Importance of Macronutrients & Micronutrients in PlantDocument25 pagesThe Importance of Macronutrients & Micronutrients in Plantmarinihassim100% (5)






























































































Download as pdf or txt
You might also like
- Reading: Healthy Lifestyle Role For All Society'Document4 pagesReading: Healthy Lifestyle Role For All Society'Tore CusimanoNo ratings yet
- Jaha 116 003196Document9 pagesJaha 116 003196Omar Nassir MoftahNo ratings yet
- Groenendaal Vandemeent2016Document11 pagesGroenendaal Vandemeent2016Soshi DaysNo ratings yet
- Management of Direct-Acting Oral Anticoagulants Surrounding Dental Procedures With Low-to-Moderate Risk of BleedingDocument6 pagesManagement of Direct-Acting Oral Anticoagulants Surrounding Dental Procedures With Low-to-Moderate Risk of BleedingOdontologia HmaspNo ratings yet
- S 025 LBLDocument16 pagesS 025 LBLarmanNo ratings yet
- Candesartan RBX PIDocument14 pagesCandesartan RBX PIshadab0123No ratings yet
- FAQ - FinerenoneDocument9 pagesFAQ - Finerenoneraea.dobsonNo ratings yet
- New Oral Anticoagulants A Practical Guide For PhysiciansDocument12 pagesNew Oral Anticoagulants A Practical Guide For PhysiciansSebastian PosadaNo ratings yet
- VorapaxarDocument21 pagesVorapaxarIoana GhirvuNo ratings yet
- Vorapaxar: General InformationDocument21 pagesVorapaxar: General InformationIoana GhirvuNo ratings yet
- Influence of Drugs Interacting With CYP3A4 On The Pharmacokinetics, Pharmacodynamics, and SafetyDocument13 pagesInfluence of Drugs Interacting With CYP3A4 On The Pharmacokinetics, Pharmacodynamics, and SafetyLuciana OliveiraNo ratings yet
- AlphaDocument6 pagesAlphaJoseph SantiagoNo ratings yet
- Ran Ola ZineDocument20 pagesRan Ola ZineHamza AlmaqtriNo ratings yet
- Warfarin Dan AspirinDocument10 pagesWarfarin Dan Aspirindita novia maharaniNo ratings yet
- Prevention of Gastrointestinal Bleeding in Patients Receiving Direct Oral Anticoagulants OpenDocument24 pagesPrevention of Gastrointestinal Bleeding in Patients Receiving Direct Oral Anticoagulants Openfitra annisaNo ratings yet
- An Open-Label, Phase 1 Study To Evaluate The Effects of Hepatic Impairment On Edoxaban Pharmacokinetics and PharmacodynamicsDocument11 pagesAn Open-Label, Phase 1 Study To Evaluate The Effects of Hepatic Impairment On Edoxaban Pharmacokinetics and PharmacodynamicsHendrawan RahmanNo ratings yet
- Nuevos anticoagulantes-BLOODDocument7 pagesNuevos anticoagulantes-BLOODnakroliNo ratings yet
- TrandolaprilDocument28 pagesTrandolaprilYeyenJaejoongNo ratings yet
- Anticoagulants TransaminasesDocument5 pagesAnticoagulants TransaminasesSony Eka NugrahaNo ratings yet
- Drugs and Renal DiseasesDocument31 pagesDrugs and Renal DiseasesStanley Tatenda MukonoNo ratings yet
- Notes 1Document24 pagesNotes 1coosa liquorsNo ratings yet
- MILsgsdgds VDocument4 pagesMILsgsdgds Vgarywall.ukNo ratings yet
- Telmisartan (Vaidyanathan)Document14 pagesTelmisartan (Vaidyanathan)Antonio SanchezNo ratings yet
- Penyesuaian Dosis Regimen Pada Pasien Dengan Gangguan Fungsi GinjalDocument19 pagesPenyesuaian Dosis Regimen Pada Pasien Dengan Gangguan Fungsi GinjalChamidRiyadiNo ratings yet
- Patisiran Pharmacokinetics, Pharmacodynamics, and Exposure-Response Analyses in The Phase 3 APOLLO Trial in Patients With Hereditary Transthyretin-Mediated (hATTR) AmyloidosisDocument13 pagesPatisiran Pharmacokinetics, Pharmacodynamics, and Exposure-Response Analyses in The Phase 3 APOLLO Trial in Patients With Hereditary Transthyretin-Mediated (hATTR) AmyloidosisMihaela BerindeieNo ratings yet
- HW3 PharmacologyDocument8 pagesHW3 PharmacologyMICHAEL GABRIEL JIMENEZNo ratings yet
- ACOS BloodDocument7 pagesACOS Bloodpablin1788No ratings yet
- Chandok Et Al, 2010Document8 pagesChandok Et Al, 2010Cika Zahrah DewisoniaNo ratings yet
- Newer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugDocument5 pagesNewer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugLouiseNo ratings yet
- Bleeding Is Out, Your Own Blood Is in 2014Document4 pagesBleeding Is Out, Your Own Blood Is in 2014viaereaNo ratings yet
- Lec - No.12 (Carbamazipine)Document13 pagesLec - No.12 (Carbamazipine)phd0780No ratings yet
- Pregabalin Hospital PharmacyDocument16 pagesPregabalin Hospital Pharmacyaditya100% (1)
- PIIS1053077018310437Document5 pagesPIIS1053077018310437andi rahmatNo ratings yet
- Farmako PDFDocument16 pagesFarmako PDFIsney HanindyaNo ratings yet
- CCO Pancreatic Advances PDFDocument4 pagesCCO Pancreatic Advances PDFSyedNo ratings yet
- Anticoag 2015november FullDocument14 pagesAnticoag 2015november FullRosanna FiorilloNo ratings yet
- Profil Farmakikinetik Pantoprazole InjeksiDocument17 pagesProfil Farmakikinetik Pantoprazole InjeksitikaNo ratings yet
- Prescribing in Patients With Liver Disease: Rakesh K TandonDocument4 pagesPrescribing in Patients With Liver Disease: Rakesh K Tandonjoydeep chakrabortyNo ratings yet
- Effect of Rivaroxaban Vs Enoxaparin On Major Cardiac Adverse Events and Bleeding Risk in The Acute Phase of Acute Coronary Syndrome PDFDocument13 pagesEffect of Rivaroxaban Vs Enoxaparin On Major Cardiac Adverse Events and Bleeding Risk in The Acute Phase of Acute Coronary Syndrome PDFKardiologi ManadoNo ratings yet
- JAPI0073 p84-88Document5 pagesJAPI0073 p84-88Subhashini KNo ratings yet
- Drugs and Kidney DiseasesDocument46 pagesDrugs and Kidney Diseasesمرتضى محمد فاضل جرجوكNo ratings yet
- CarvedilolDocument7 pagesCarvedilolHelen QuirogaNo ratings yet
- Mefenamic Acid Capsules, USP 250 MG RX Only: Reference ID: 3928117Document20 pagesMefenamic Acid Capsules, USP 250 MG RX Only: Reference ID: 3928117Riska AuliahNo ratings yet
- Neuro-Oncology PracticeDocument16 pagesNeuro-Oncology Practice6ydn87w6gpNo ratings yet
- Bipolar Disorders and Carbamazepine PharmacokinetiDocument5 pagesBipolar Disorders and Carbamazepine PharmacokinetiAgr YuroNo ratings yet
- Bipolar Disorders and Carbamazepine PharmacokinetiDocument6 pagesBipolar Disorders and Carbamazepine PharmacokinetiluthfiahNo ratings yet
- Procainamide Hydrochloride: Major UseDocument3 pagesProcainamide Hydrochloride: Major UseDosi SiliNo ratings yet
- Effect of Rosuvastatin On Warfarin Pharmacodynamics and PharmacokineticsDocument9 pagesEffect of Rosuvastatin On Warfarin Pharmacodynamics and PharmacokineticsLuciana OliveiraNo ratings yet
- Dacarbazine Monograph 1june2013 FormattedDocument7 pagesDacarbazine Monograph 1june2013 FormattedRobert ChristevenNo ratings yet
- Medi 95 E2881Document5 pagesMedi 95 E2881Betari YoscarNo ratings yet
- Randomized Controlled Clinical Trial of Corticosteroids Plus Ace-Inhibitors With Long-Term Follow-Up in Proteinuric Iga NephropathyDocument7 pagesRandomized Controlled Clinical Trial of Corticosteroids Plus Ace-Inhibitors With Long-Term Follow-Up in Proteinuric Iga Nephropathyguugle gogleNo ratings yet
- Lancet 2010 376 489Document2 pagesLancet 2010 376 489CClaaudianagoisNo ratings yet
- Novel Oral Anticoagulants in The Management of Coronary Artery DiseaseDocument8 pagesNovel Oral Anticoagulants in The Management of Coronary Artery DiseaseqiraniNo ratings yet
- Nateglinide Tablets: GeriatricDocument2 pagesNateglinide Tablets: GeriatricUlfa AlyaNo ratings yet
- Reemplazo de Cadera FrontalDocument10 pagesReemplazo de Cadera FrontalffffffffffffNo ratings yet
- Schizophr Bull 1998 Young 381 90Document10 pagesSchizophr Bull 1998 Young 381 90Kadelsy BristolNo ratings yet
- Putri RamadhanDocument44 pagesPutri RamadhanRama MulyadiNo ratings yet
- 949-Texto Del Artículo-7086-1-10-20231207Document8 pages949-Texto Del Artículo-7086-1-10-20231207mplp2721No ratings yet
- Hep 24519 PDFDocument5 pagesHep 24519 PDFLaras Bani WasesoNo ratings yet
- Diagnostic and Therapeutic Advances in Hepatology Terlipressin: An Asset For Hepatologists!Document5 pagesDiagnostic and Therapeutic Advances in Hepatology Terlipressin: An Asset For Hepatologists!Laras Bani WasesoNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Bmjopen 2018 026362Document7 pagesBmjopen 2018 026362Kevin HartonoNo ratings yet
- Journal Alergi Terhadap DepresiDocument31 pagesJournal Alergi Terhadap DepresiKevin HartonoNo ratings yet
- DermatitisDocument9 pagesDermatitisKevin HartonoNo ratings yet
- Biochemistry & Pharmacology: Open Access: The Morphine and Codeine Equianalgesic 'SDocument5 pagesBiochemistry & Pharmacology: Open Access: The Morphine and Codeine Equianalgesic 'SKevin HartonoNo ratings yet
- Review Current Concepts in The Pathogenesis and Treatment of Chronic Suppurative Otitis MediaDocument14 pagesReview Current Concepts in The Pathogenesis and Treatment of Chronic Suppurative Otitis MediaKevin HartonoNo ratings yet
- Final Presentation Journal OtitisDocument34 pagesFinal Presentation Journal OtitisKevin HartonoNo ratings yet
- RHU Situanional ReportDocument8 pagesRHU Situanional ReportErnest AtonNo ratings yet
- Evolution of Life On Earth: General Biology 2Document10 pagesEvolution of Life On Earth: General Biology 2Geox NikeeNo ratings yet
- Growth Evaluation and Meat Assessment of Native Pig in Romblon Province, PhilippinesDocument7 pagesGrowth Evaluation and Meat Assessment of Native Pig in Romblon Province, PhilippinesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- The Magic Mushroom Growers GuideDocument61 pagesThe Magic Mushroom Growers GuideDaniel Marsh83% (6)
- Leela Residences at Bhartiya City - Amenities: Common LobbyDocument4 pagesLeela Residences at Bhartiya City - Amenities: Common LobbyFrancis XavierNo ratings yet
- Perkins Spares 80,100Document10 pagesPerkins Spares 80,100ramsey222No ratings yet
- Fluor CarbonDocument3 pagesFluor CarbonHrishikesh DhawadshikarNo ratings yet
- Migraine DiaryDocument1 pageMigraine DiaryEmily KirbyNo ratings yet
- Activated Carbon From BambooDocument19 pagesActivated Carbon From BambooErik WeeksNo ratings yet
- Fresh and Simple PDFDocument3 pagesFresh and Simple PDFthivashnee padayacheeNo ratings yet
- Andovercontinuumul 864 Bacnetsmokecontrolsystemdesignguide 101134Document124 pagesAndovercontinuumul 864 Bacnetsmokecontrolsystemdesignguide 101134Chong CongNo ratings yet
- Chapter 21 Electric Charge - Gui SVDocument5 pagesChapter 21 Electric Charge - Gui SVHậu Vũ100% (1)
- Domestic Dogs: Temporal Range: at Least 14,200 Years Ago - PresentDocument35 pagesDomestic Dogs: Temporal Range: at Least 14,200 Years Ago - PresentirayoNo ratings yet
- Mass. Proposed AddendumsDocument25 pagesMass. Proposed AddendumsKirk HartleyNo ratings yet
- Raising Permit: Office of The Building OfficialDocument2 pagesRaising Permit: Office of The Building OfficialJc JüsäyänNo ratings yet
- Timing Protection in AUTOSAR ISO 26262Document10 pagesTiming Protection in AUTOSAR ISO 26262Joseph KymmNo ratings yet
- Zoology Mammals (Rabbit)Document3 pagesZoology Mammals (Rabbit)PerrieNo ratings yet
- Caring For Your African American/Biracial Child's HairDocument32 pagesCaring For Your African American/Biracial Child's Hair4kidslikemeNo ratings yet
- Pentavitin - DSMDocument3 pagesPentavitin - DSMRnD Roi SuryaNo ratings yet
- The Best Things To Do in Binghamton NYDocument4 pagesThe Best Things To Do in Binghamton NYShashank SangwanNo ratings yet
- Focus Level 3 Table of Contents PDFDocument2 pagesFocus Level 3 Table of Contents PDFDaria KudosLamNo ratings yet
- TirupathiDocument14 pagesTirupathiEkta Adlakha100% (1)
- String of Pearls Slide ShowDocument23 pagesString of Pearls Slide Showjimhtolbert434No ratings yet
- Beer & Wine Osd PresDocument18 pagesBeer & Wine Osd PresAnand100% (1)
- Nameplate PDFDocument8 pagesNameplate PDFobida adailehNo ratings yet
- Astrological Study of Infertility - ConclusionDocument9 pagesAstrological Study of Infertility - ConclusionAnamika SNo ratings yet
- Essay C DraftDocument7 pagesEssay C Draftapi-242837115No ratings yet
- The Importance of Macronutrients & Micronutrients in PlantDocument25 pagesThe Importance of Macronutrients & Micronutrients in Plantmarinihassim100% (5)