Download as pdf or txt
You might also like
- Condylar Hyperplasia of The Temporomandibular Joint: Types, Treatment, and Surgical ImplicationsDocument13 pagesCondylar Hyperplasia of The Temporomandibular Joint: Types, Treatment, and Surgical ImplicationsIsa TorresNo ratings yet
- A Classification System For Conditions Causing Condylar HyperplasiaDocument29 pagesA Classification System For Conditions Causing Condylar HyperplasiaDaniel CoêlhoNo ratings yet
- Clasifiacion de Hiperplasia Condilar WooolforDocument47 pagesClasifiacion de Hiperplasia Condilar WooolforSantos TicaNo ratings yet
- High Condylectomy For The Treatment of Mandibular Condylar Hyperplasia: A Systematic Review of The LiteratureDocument12 pagesHigh Condylectomy For The Treatment of Mandibular Condylar Hyperplasia: A Systematic Review of The Literaturemarcela0426No ratings yet
- Condylar HyperplasiaDocument43 pagesCondylar HyperplasiaAhmadfattah Ramadan0% (1)
- Condylar Hyperplasia: Current Thinking: ReviewDocument9 pagesCondylar Hyperplasia: Current Thinking: ReviewSantos TicaNo ratings yet
- Unilateral Condylar Hyperplasia: A Case Report and Review of LiteratureDocument4 pagesUnilateral Condylar Hyperplasia: A Case Report and Review of LiteratureCésar Mauricio VilchezNo ratings yet
- Condylar Hyperplasia: Current ThinkingDocument8 pagesCondylar Hyperplasia: Current ThinkingFiorella Plasencia EsquivelNo ratings yet
- Wolford 2009Document10 pagesWolford 2009Mary MontoyaNo ratings yet
- Chondrosarcoma of The Jaw: A Closer Look at Its ManagementDocument7 pagesChondrosarcoma of The Jaw: A Closer Look at Its ManagementHagar AlaaNo ratings yet
- Art CXDocument9 pagesArt CXMilena RamirezNo ratings yet
- Antegonial NotchDocument3 pagesAntegonial NotchpveginaduNo ratings yet
- Congenital Deformities and Developmental Abnormalities of The Mandibular Condyle in The Temporomandibular JointDocument8 pagesCongenital Deformities and Developmental Abnormalities of The Mandibular Condyle in The Temporomandibular JointMarcelaGutiérrezCarranzaNo ratings yet
- Condylar HyperplasiaDocument20 pagesCondylar HyperplasiaSamuel Flores CalderonNo ratings yet
- Chronic Recurrent Multifocal Osteomyelitis in Association With Pyoderma GangraenosumDocument7 pagesChronic Recurrent Multifocal Osteomyelitis in Association With Pyoderma GangraenosumDha Dina SevofrationNo ratings yet
- Facial Asymmetry Due To Condylar Hyperplasia PDFDocument3 pagesFacial Asymmetry Due To Condylar Hyperplasia PDFIndah Hafniar HasibuanNo ratings yet
- Asimetrii MandibulareDocument25 pagesAsimetrii MandibulareBranici OanaNo ratings yet
- Craniofacial DeformitiesDocument12 pagesCraniofacial DeformitiessarahekmateanNo ratings yet
- Craniofacial Syndromes: Learning Objectives: After Studying This Article, The Participant Should Be AbleDocument26 pagesCraniofacial Syndromes: Learning Objectives: After Studying This Article, The Participant Should Be AblePutri Natasia KinskiNo ratings yet
- Review Article: Hemangiomas and Vascular Malformations: Current Theory and ManagementDocument11 pagesReview Article: Hemangiomas and Vascular Malformations: Current Theory and ManagementDewi AngrianaNo ratings yet
- Orthodontics and Pediatric DentistryDocument62 pagesOrthodontics and Pediatric DentistryAnggaHumalaBeltsazarNapitupuluNo ratings yet
- Cherubism: A Case Report and Review of LiteratureDocument4 pagesCherubism: A Case Report and Review of LiteratureAisha DewiNo ratings yet
- Soft Tissue Tumors6 - 0Document16 pagesSoft Tissue Tumors6 - 0Romy MinascurtaNo ratings yet
- Infantile Hemangiomas: A Review: Pediatric Ophthalmology UpdateDocument9 pagesInfantile Hemangiomas: A Review: Pediatric Ophthalmology UpdateYipno Wanhar El MawardiNo ratings yet
- Vascular Lesions in NeonatesDocument15 pagesVascular Lesions in NeonatesYogeshRavalNo ratings yet
- Osteocondroma & OsteochondromatosisDocument24 pagesOsteocondroma & OsteochondromatosisrazalihamidNo ratings yet
- Lateral Neck SwellingDocument62 pagesLateral Neck Swellingசுபத்ரா சந்திரசேகர்No ratings yet
- Craniofacial Syndromes.33Document26 pagesCraniofacial Syndromes.33andrew kilshawNo ratings yet
- Querubismo Marzo JOMSDocument6 pagesQuerubismo Marzo JOMSJerson Huamán BernalNo ratings yet
- Cazzolla2018 PDFDocument5 pagesCazzolla2018 PDFMarouaBOUFLIJANo ratings yet
- TMJ Disorders (1) BNW FinalDocument87 pagesTMJ Disorders (1) BNW Finalshamshada2000No ratings yet
- Cervicofacial Vascular Anomalies. I. Hemangiomas and Other Benign Vascular TumorsDocument9 pagesCervicofacial Vascular Anomalies. I. Hemangiomas and Other Benign Vascular TumorsBikash ShresthaNo ratings yet
- Cherubism Combined With EpilepsyDocument7 pagesCherubism Combined With EpilepsywwhhjNo ratings yet
- Spinal Cord EnhancementDocument3 pagesSpinal Cord EnhancementGabriel PinillaNo ratings yet
- Jurnal BM Dok JulDocument7 pagesJurnal BM Dok JulFajar RamadhanNo ratings yet
- Uoi 114 HDocument6 pagesUoi 114 HashajangamNo ratings yet
- Hemihypertrophy: A K C Leung, J H S Fong, A G LeongDocument4 pagesHemihypertrophy: A K C Leung, J H S Fong, A G LeongZacky Aulia MursiNo ratings yet
- Facial AsymmetryDocument41 pagesFacial AsymmetryRahul GoteNo ratings yet
- AbstractDocument1 pageAbstractbalamanoharNo ratings yet
- Orthodontic Treatmentafter High Condylectomyin Patientswith Unilateral Condylar HyperplasiaDocument9 pagesOrthodontic Treatmentafter High Condylectomyin Patientswith Unilateral Condylar HyperplasiaOrtodoncia UNAL 2020No ratings yet
- Diagnóstico DeficienteDocument6 pagesDiagnóstico Deficientelucasschuelter01No ratings yet
- Facial Asymmetry - Etiology, Evaluation, and ManagementDocument11 pagesFacial Asymmetry - Etiology, Evaluation, and ManagementAhmad AssariNo ratings yet
- MicrosomiaDocument16 pagesMicrosomiaAriana AmarilesNo ratings yet
- HEMANGIOMADocument4 pagesHEMANGIOMAROSEN NNo ratings yet
- AAOS2002 TumorDocument59 pagesAAOS2002 TumorHizkyas KassayeNo ratings yet
- Retromolar Embryonal Rhabdomyosarcoma: A CaseDocument6 pagesRetromolar Embryonal Rhabdomyosarcoma: A CaseNabila RizkikaNo ratings yet
- Jurnal 2Document7 pagesJurnal 2faridiswantoNo ratings yet
- Facial Hemihypertrophy and Facial Hemiatrophy: Report of 2 CasesDocument3 pagesFacial Hemihypertrophy and Facial Hemiatrophy: Report of 2 CasesBimalKrishnaNo ratings yet
- Craniopharyngioma: Case SummaryDocument3 pagesCraniopharyngioma: Case SummaryeugeniaNo ratings yet
- Mod Path Ol 2015131Document17 pagesMod Path Ol 2015131Mariana UsatiiNo ratings yet
- Radiologia Espacio Masticador 2020Document11 pagesRadiologia Espacio Masticador 2020Marcela GNo ratings yet
- Lancet NeDocument10 pagesLancet NeKrisTianz OkaNo ratings yet
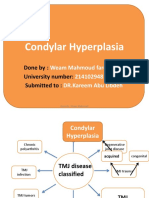
- Condylar Hyperplasia: Done By: University Number: Submitted ToDocument69 pagesCondylar Hyperplasia: Done By: University Number: Submitted Tomehak malhotraNo ratings yet
- Kirim Ira CantikDocument7 pagesKirim Ira CantikirastefanaticNo ratings yet
- Lymphatic Malformations Diagnosis and ManagementDocument8 pagesLymphatic Malformations Diagnosis and ManagementMutiara KantikaNo ratings yet
- Differential Diagnosis of A Neck Mass - UpToDate PDFDocument16 pagesDifferential Diagnosis of A Neck Mass - UpToDate PDFDr.Anurag FursuleNo ratings yet
- RhabdomyosarcomaDocument9 pagesRhabdomyosarcomaNugroho Tri WibowoNo ratings yet
- Differential Diagnosis of A Neck Mass - UpToDateDocument16 pagesDifferential Diagnosis of A Neck Mass - UpToDatezzellowknifeNo ratings yet
- Cell Wars: The Dynamics of Oncology: Battlefield Micro: The Epic Struggle Against CancerFrom EverandCell Wars: The Dynamics of Oncology: Battlefield Micro: The Epic Struggle Against CancerNo ratings yet
- Multiple Myeloma and Other Plasma Cell NeoplasmsFrom EverandMultiple Myeloma and Other Plasma Cell NeoplasmsMeletios A. DimopoulosNo ratings yet
- D 661Document20 pagesD 661CristianNo ratings yet
- S.No Description Qty Unit Assumed by HWPL: Scope of Work - Supply PSSDocument14 pagesS.No Description Qty Unit Assumed by HWPL: Scope of Work - Supply PSSASR REDDYNo ratings yet
- The Hamburger Ate Boy Isn't Acceptable (Odd) But The Boy Ate The Hamburger Is Hamburger Doesn't Have This Property and The Noun Boy DoesDocument6 pagesThe Hamburger Ate Boy Isn't Acceptable (Odd) But The Boy Ate The Hamburger Is Hamburger Doesn't Have This Property and The Noun Boy DoesDania SaviraNo ratings yet
- 14th Jan 330pm NuptialsDocument30 pages14th Jan 330pm Nuptialsvivsubs18No ratings yet
- Worksheet MixedDocument11 pagesWorksheet MixedBaby AleiraNo ratings yet
- 2020 79th PNWIMC Annual Conference AnnouncementDocument2 pages2020 79th PNWIMC Annual Conference AnnouncementnwberryfoundationNo ratings yet
- Road Roller Sakai SW880 Maint Serv MNLDocument95 pagesRoad Roller Sakai SW880 Maint Serv MNLGarick ParialpalacioNo ratings yet
- Topic 6 Circular Motion Test P1Document11 pagesTopic 6 Circular Motion Test P1Sabrina_LGXNo ratings yet
- Clean RoomDocument9 pagesClean Roomxyzscribd1988No ratings yet
- Guia de Aprendizaje-QuantifiersDocument8 pagesGuia de Aprendizaje-Quantifiersangelita berdugoNo ratings yet
- Gen - Physics 12 Q4 WK8Document18 pagesGen - Physics 12 Q4 WK8Mark Julius Felix PagudNo ratings yet
- FALLSEM2022-23 BCSE202L TH VL2022230103384 Reference Material I 22-07-2022 DSA Module1 1Document15 pagesFALLSEM2022-23 BCSE202L TH VL2022230103384 Reference Material I 22-07-2022 DSA Module1 1anisha sharmaNo ratings yet
- Adeline Mowbray by Amelia Opie PDFDocument171 pagesAdeline Mowbray by Amelia Opie PDFArmin NiknamNo ratings yet
- OTS Optical Tool Setter: Installation GuideDocument52 pagesOTS Optical Tool Setter: Installation GuideIrina BesliuNo ratings yet
- Fleming's Left Hand Rule (ForDocument8 pagesFleming's Left Hand Rule (Forb_geyl4286No ratings yet
- Space - The Final FrontierDocument51 pagesSpace - The Final FrontierAbdul Shakoor100% (1)
- Materi2012.1pre Print - Part1Document174 pagesMateri2012.1pre Print - Part1Hari TulusNo ratings yet
- Quiz - Lab Safety and ApparatusDocument1 pageQuiz - Lab Safety and ApparatusJohn Kristoffer RoblezaNo ratings yet
- Lo2012 TPFDocument114 pagesLo2012 TPFramjoceNo ratings yet
- Project Proposal - BSMA 1202 byDocument19 pagesProject Proposal - BSMA 1202 byFabbi FababairNo ratings yet
- Taiwan Panorama 2023 NovDocument128 pagesTaiwan Panorama 2023 NovKwang HwaNo ratings yet
- From Georges Sorel - Essays in Socialism and PhilosophyDocument411 pagesFrom Georges Sorel - Essays in Socialism and PhilosophyHugãoNo ratings yet
- EE Cleveland: Jesus and The Other Thief (Thief On The Cross)Document2 pagesEE Cleveland: Jesus and The Other Thief (Thief On The Cross)Samuel KadyakaleNo ratings yet
- Energy Challenges in SomaliaDocument14 pagesEnergy Challenges in SomaliaLiban Abdullahi AliNo ratings yet
- Hermite Cubic Spline CurveDocument4 pagesHermite Cubic Spline CurveKshitij SharmaNo ratings yet
- HIPPROSTHESISCATALOGDocument98 pagesHIPPROSTHESISCATALOGBrenda Martinez RomanNo ratings yet
- I/O Specifications: CPU Unit DescriptionsDocument10 pagesI/O Specifications: CPU Unit Descriptionsวรพงษ์ กอชัชวาลNo ratings yet
- Instruments Obs & Gynea PDFDocument19 pagesInstruments Obs & Gynea PDFVibes Usmlee100% (1)
- Slag Splashing Technique in Converter OperationDocument3 pagesSlag Splashing Technique in Converter Operationrabikant_25No ratings yet
- 3bhs823693 Zab E11 D Megastar TC SW Amc TableDocument99 pages3bhs823693 Zab E11 D Megastar TC SW Amc TablesepulcrijkdNo ratings yet