Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- Hesi Review For Health AssessmentDocument18 pagesHesi Review For Health AssessmentJennifer Portillo100% (19)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 1 s2.0 S0160252716300553 MainDocument7 pages1 s2.0 S0160252716300553 MainDiego Alejandro ZambranoNo ratings yet
- 1-S2.0-S1359178918303586-Main (1) (Abusador Mujer)Document22 pages1-S2.0-S1359178918303586-Main (1) (Abusador Mujer)Diego Alejandro ZambranoNo ratings yet
- 1 s2.0 S0145213420302854 MainDocument14 pages1 s2.0 S0145213420302854 MainDiego Alejandro ZambranoNo ratings yet
- Zalewskietal 2018 Identifying Novel Applications of DBT Emotion Regulation and ParentingDocument6 pagesZalewskietal 2018 Identifying Novel Applications of DBT Emotion Regulation and ParentingDiego Alejandro ZambranoNo ratings yet
- HMO Proposal For Individual Family Account REGULAR-UPDATED AS OF JULY 2...Document11 pagesHMO Proposal For Individual Family Account REGULAR-UPDATED AS OF JULY 2...Arron BuenavistaNo ratings yet
- Buhner MethodDocument13 pagesBuhner Method7candlesburning100% (2)
- Anterior Open BiteDocument7 pagesAnterior Open BiteGowri100% (1)
- PHD Thesis On Occupational StressDocument7 pagesPHD Thesis On Occupational Stresscindyturnertorrance100% (2)
- Primary Health CareDocument17 pagesPrimary Health CareKevins ChepsirNo ratings yet
- English. 101 Midterm Week 1 3A.Y. 2021 2022 First Sem PDFDocument75 pagesEnglish. 101 Midterm Week 1 3A.Y. 2021 2022 First Sem PDFZarah E. DinoyNo ratings yet
- LoadVoucher AspxDocument4 pagesLoadVoucher AspxEdnalyn CasasNo ratings yet
- Research Paper - Negative Effects of Video Games On ChildrenDocument2 pagesResearch Paper - Negative Effects of Video Games On ChildrenNicole JimelgaNo ratings yet
- SWMS Sample - Safe Work MethodDocument8 pagesSWMS Sample - Safe Work Methodsupasart100% (1)
- Complaint - Wall V Southwest AirlinesDocument94 pagesComplaint - Wall V Southwest AirlinesDaniel MillerNo ratings yet
- Uncertainity Illness Theory (Merle H.mishel)Document50 pagesUncertainity Illness Theory (Merle H.mishel)Taate Mohammed100% (1)
- Neochem BilirubinDocument1 pageNeochem BilirubinSamir MeddouraNo ratings yet
- Motivation Concepts: Kristine Angelie BelgadoDocument12 pagesMotivation Concepts: Kristine Angelie BelgadoKristine BelgadoNo ratings yet
- Ope. Q 2 Part 1Document3 pagesOpe. Q 2 Part 1Kevin DeswandaNo ratings yet
- CHN1 Worksheet1Document5 pagesCHN1 Worksheet1Chariza MayNo ratings yet
- Champion 12 2 Answer Key 2Document16 pagesChampion 12 2 Answer Key 2أمل دنياNo ratings yet
- Summer FW Performance EvaluationDocument13 pagesSummer FW Performance Evaluationapi-583667426No ratings yet
- Endocrinology Expected ValuesDocument88 pagesEndocrinology Expected ValuesSandra SánchezNo ratings yet
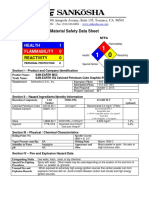
- Material Safety Data Sheet - SAN EARTHDocument3 pagesMaterial Safety Data Sheet - SAN EARTHPaulo CLNo ratings yet
- FS 100 Module 4 Output - Noya Done - 085821Document8 pagesFS 100 Module 4 Output - Noya Done - 085821Antonette NoyaNo ratings yet
- HPV Amostras AlternativasDocument6 pagesHPV Amostras Alternativasnathaliasantosx3No ratings yet
- AB Lounge 2 ManualDocument13 pagesAB Lounge 2 ManualStacy MinnsNo ratings yet
- Question Bankindian Ethos in Management Sem Vi 2019-2020 Mock TestDocument2 pagesQuestion Bankindian Ethos in Management Sem Vi 2019-2020 Mock TestShubhada AmaneNo ratings yet
- ANCC NCPD ManualDocument58 pagesANCC NCPD Manualshadi alshadafanNo ratings yet
- Biological Approach Dement and Kleitman (Sleep and Dreams) : Ms - Mariam El GabalawyDocument34 pagesBiological Approach Dement and Kleitman (Sleep and Dreams) : Ms - Mariam El GabalawyNeda ElewaNo ratings yet
- Learning Objective: Book 2 English For Professional NurseDocument3 pagesLearning Objective: Book 2 English For Professional NurseLestari RahayuNo ratings yet
- Nalco-Tri-Act 2813 MSDSDocument13 pagesNalco-Tri-Act 2813 MSDSSabih UllahNo ratings yet
- Case History PresentationDocument64 pagesCase History PresentationNitin FatingNo ratings yet
- MeaslesDocument2 pagesMeaslessaurabhkankariyaNo ratings yet