Download as pdf or txt
You might also like
- He Still Chose Me 2024Document4 pagesHe Still Chose Me 2024Susan Bauer Martire MagliocchiNo ratings yet
- Gottman Institute - Renew Your Love-Love Letter ExchangeDocument4 pagesGottman Institute - Renew Your Love-Love Letter ExchangeDiah RahmiNo ratings yet
- Catalog 2017Document88 pagesCatalog 2017Danilo Choir StuffNo ratings yet
- Mi Jesus Mi Amado, Sax EbDocument2 pagesMi Jesus Mi Amado, Sax EbLeo DNo ratings yet
- See, Nature Rejoicing: From The Ode To Queen MaryDocument10 pagesSee, Nature Rejoicing: From The Ode To Queen MaryMichael FabianNo ratings yet
- Uno para El Otro Tercer CieloDocument2 pagesUno para El Otro Tercer CieloeduardguitarproNo ratings yet
- Jay Z FT MR Hudson Forever YoungDocument2 pagesJay Z FT MR Hudson Forever YoungfernandoNo ratings yet
- Correré DrumsDocument2 pagesCorreré DrumsEdwin CujcuyNo ratings yet
- The Olive Tree PartituraDocument7 pagesThe Olive Tree PartituraTadeu MontenegroNo ratings yet
- Shine Barbie in The 12 Dancing PrincessesDocument3 pagesShine Barbie in The 12 Dancing PrincessesLucas PortelaNo ratings yet
- Otče Ťa Chválim: B Eb/B B F Eb/F B2 BDocument1 pageOtče Ťa Chválim: B Eb/B B F Eb/F B2 BdzadekNo ratings yet
- I Am A Child of GodDocument5 pagesI Am A Child of Godapi-19854402No ratings yet
- Cantemos Al Amor de Los AmoresDocument1 pageCantemos Al Amor de Los AmoresSaúl Hernández ÁlamoNo ratings yet
- Is There Room Sailiata Fano JR Is There Room Tenor 1Document3 pagesIs There Room Sailiata Fano JR Is There Room Tenor 1CRISTINA SOL ASARNo ratings yet
- A Standardized Program For Analyzing Temperament Its Development and Assessment in Gauging Individual Personality CharacteristicsDocument3 pagesA Standardized Program For Analyzing Temperament Its Development and Assessment in Gauging Individual Personality CharacteristicsJoshua StanNo ratings yet
- Is There Room Sailiata Fano JR Is There Roomtenor 2Document3 pagesIs There Room Sailiata Fano JR Is There Roomtenor 2CRISTINA SOL ASARNo ratings yet
- A Higher Call LyricsDocument7 pagesA Higher Call LyricsNota Belz100% (1)
- Amar Y Querer Eb PDFDocument3 pagesAmar Y Querer Eb PDFanon_808306552No ratings yet
- Las Mañanitas en SOLDocument1 pageLas Mañanitas en SOLEmma Jeannette RAmírezNo ratings yet
- Digno de AlabanzaDocument9 pagesDigno de AlabanzaDanilo Flores VillalobosNo ratings yet
- He Is My All Solo or Mezzo Baritone DuetDocument5 pagesHe Is My All Solo or Mezzo Baritone DuetIvan CabellonNo ratings yet
- When The Morning Comes: Q in The Sweet by and byDocument12 pagesWhen The Morning Comes: Q in The Sweet by and byMarcos Antonio MachadoNo ratings yet
- Canto Mi Vida TenDocument6 pagesCanto Mi Vida TenMiiry AkeNo ratings yet
- You Are The ChristDocument2 pagesYou Are The ChristEduardo Pastor100% (1)
- Aunque Ruja La Tormenta: PianoDocument2 pagesAunque Ruja La Tormenta: PianoSergio Fernandez100% (1)
- Oh How I Love Jesus: PianoDocument2 pagesOh How I Love Jesus: PianoNeanderNo ratings yet
- He Came For Me - TransposedDocument5 pagesHe Came For Me - TransposedDaniel LittellNo ratings yet
- 2009 12 0030 A Childs Prayer SpaDocument2 pages2009 12 0030 A Childs Prayer Spamoronick920100% (1)
- Porque Ele ViveDocument7 pagesPorque Ele ViveJonatasCostaNo ratings yet
- Sweet Hour of Prayer PDF Sheet MusicDocument5 pagesSweet Hour of Prayer PDF Sheet MusicLisandra SantinNo ratings yet
- Goodness of GodDocument7 pagesGoodness of GodDavidNo ratings yet
- Born To Wear A Crown SsatbDocument5 pagesBorn To Wear A Crown SsatbBabalola SundayNo ratings yet
- Santo, Santo, Santo (Variaciones) - Violin - IDocument1 pageSanto, Santo, Santo (Variaciones) - Violin - IMagetzy Mejia SoteloNo ratings yet
- Come Thou Fount (Above All Else) - Live (D)Document1 pageCome Thou Fount (Above All Else) - Live (D)Wim SupergansNo ratings yet
- Inyow: LDRL Cacdrgds GyefabDocument7 pagesInyow: LDRL Cacdrgds GyefabMark Albert Gatdula RaqueñoNo ratings yet
- 030201Document4 pages030201Nezer VergaraNo ratings yet
- 271 - Pdfsam - Guitarra Volumen 1 - Flor y Canto - JPR504 PDFDocument1 page271 - Pdfsam - Guitarra Volumen 1 - Flor y Canto - JPR504 PDFJuan Pablo GarcíaNo ratings yet
- Messiah - For Unto Us A Child Is Born PDFDocument10 pagesMessiah - For Unto Us A Child Is Born PDFMicaeli Rourke du PlessisNo ratings yet
- Bach BWV 538Document12 pagesBach BWV 538P-o FaalandNo ratings yet
- List of Recommended Songs For The Sundays of Lent Until Good FridayDocument28 pagesList of Recommended Songs For The Sundays of Lent Until Good FridayRussel Matthew PatolotNo ratings yet
- In The Upper Room: (TTBB and Cello)Document7 pagesIn The Upper Room: (TTBB and Cello)Pablo CastilloNo ratings yet
- 415 - Room at The Cross: Lead SheetDocument2 pages415 - Room at The Cross: Lead SheetSamuel ThibaultNo ratings yet
- To God Be The GloryDocument3 pagesTo God Be The GloryGarcia Emi0% (1)
- Love - Song-PianoDocument2 pagesLove - Song-PianorhodesjanNo ratings yet
- Amor de Mis Amores - Trumpet 1 - .PDF TRUM 1Document2 pagesAmor de Mis Amores - Trumpet 1 - .PDF TRUM 1Juanca Chugchilan100% (1)
- Dame Un Nuevo CorazónDocument3 pagesDame Un Nuevo CorazónPriscila TorresNo ratings yet
- This Is The DayDocument1 pageThis Is The DayruelbelloNo ratings yet
- Serenata Schubert. Dos Flautas y PianoDocument5 pagesSerenata Schubert. Dos Flautas y PianoconchiviolaNo ratings yet
- Hark! The Herald Angels Sing: Arr. Pentatonix 108Document15 pagesHark! The Herald Angels Sing: Arr. Pentatonix 108Anna ŚwięcickaNo ratings yet
- 向祢舉手 Lord I Stretch My Hands to You Jay AlthouseDocument5 pages向祢舉手 Lord I Stretch My Hands to You Jay Althouse蔡育霖No ratings yet
- Levanto Mis Manos EbDocument1 pageLevanto Mis Manos EbJAIRO EUCEDANo ratings yet
- Whole AgainDocument3 pagesWhole AgainLeon Odarniem Saniraf EtelpNo ratings yet
- The - Church's - One - Foundation - AURELIA Full Score-ChoralDocument7 pagesThe - Church's - One - Foundation - AURELIA Full Score-Choralpowell_scottNo ratings yet
- Cargador Bateria Chicago Electric 66783 PDFDocument12 pagesCargador Bateria Chicago Electric 66783 PDFRicardo JimenezNo ratings yet
- Born On Christmas Day (Coro de Niños) - Voz 3Document1 pageBorn On Christmas Day (Coro de Niños) - Voz 3SebastianIbarraNo ratings yet
- Modulo5. Behavior Change-2021Document20 pagesModulo5. Behavior Change-2021Armin Arceo DuranNo ratings yet
- Lifestyle Management S47: Evidence For The Bene FitsDocument50 pagesLifestyle Management S47: Evidence For The Bene FitsEvelyn CóndorNo ratings yet
- Diabetics Self Management PDFDocument56 pagesDiabetics Self Management PDFwsergio0072No ratings yet
- Foundations of Care: Education, Nutrition, Physical Activity, Smoking Cessation, Psychosocial Care, and ImmunizationDocument11 pagesFoundations of Care: Education, Nutrition, Physical Activity, Smoking Cessation, Psychosocial Care, and ImmunizationrakolovaNo ratings yet
- The Confidence in Diabetes Self-Care Scale (Adultos) (Alemania y USA)Document6 pagesThe Confidence in Diabetes Self-Care Scale (Adultos) (Alemania y USA)Verónica MelgarejoNo ratings yet
- Jadwal Ujian Proposal Skripsi - MaternitasDocument2 pagesJadwal Ujian Proposal Skripsi - MaternitasSokhifatun NajahNo ratings yet
- Defibrillation & Cardioversion: Ns. Retno Setyawati, M.Kep., SP - KMBDocument34 pagesDefibrillation & Cardioversion: Ns. Retno Setyawati, M.Kep., SP - KMBSokhifatun NajahNo ratings yet
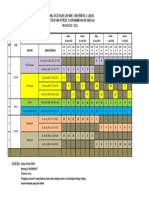
- Jadwal Osce Online Lab KMB 3, Maternitas 2, Gadar Semester V Dan Vi Prodi S1 Keperawatan Fik Unissula TAHUN 2020 / 2021Document1 pageJadwal Osce Online Lab KMB 3, Maternitas 2, Gadar Semester V Dan Vi Prodi S1 Keperawatan Fik Unissula TAHUN 2020 / 2021Sokhifatun NajahNo ratings yet
- Biostatik Siti Ulfatun N C 30901800172Document3 pagesBiostatik Siti Ulfatun N C 30901800172Sokhifatun NajahNo ratings yet
- 07mjms25032018 Oa5Document11 pages07mjms25032018 Oa5Sokhifatun NajahNo ratings yet
- Calculation and Analyzing of Braces ConnectionsDocument71 pagesCalculation and Analyzing of Braces Connectionsjuliefe robles100% (1)
- Rai Community ProposalDocument11 pagesRai Community ProposalshekharNo ratings yet
- Student Handbook 2019-2020Document30 pagesStudent Handbook 2019-2020Gaetan HammondNo ratings yet
- BusEthSocResp Weeks 3-4Document6 pagesBusEthSocResp Weeks 3-4Christopher Nanz Lagura CustanNo ratings yet
- Coupling - Machine DesignDocument73 pagesCoupling - Machine DesignAk GamingNo ratings yet
- Afghan Girl: in Search of TheDocument2 pagesAfghan Girl: in Search of TheSon PhamNo ratings yet
- Photo Essay PDFDocument2 pagesPhoto Essay PDFMartha Glorie Manalo WallisNo ratings yet
- Simple Past Full ExercisesDocument6 pagesSimple Past Full Exercisespablo1130No ratings yet
- Becker Textilwerk: Preparation SheetDocument2 pagesBecker Textilwerk: Preparation Sheetabeer fatimaNo ratings yet
- Worksheet 8 Gread Number1Document3 pagesWorksheet 8 Gread Number1nknbjjqh5gNo ratings yet
- PETRONAS RETAILER Price List - W.E.F 10-10-23Document2 pagesPETRONAS RETAILER Price List - W.E.F 10-10-23Mujeeb SiddiqueNo ratings yet
- Office of The Punong Barangay Barangay Certification of AcceptanceDocument1 pageOffice of The Punong Barangay Barangay Certification of AcceptanceMah Jane DivinaNo ratings yet
- Notes On TennysonDocument2 pagesNotes On TennysonDonatella Di LelloNo ratings yet
- 1b Reading Output 2Document1 page1b Reading Output 2Elisha Maurelle AncogNo ratings yet
- CESPL - Profile1Document93 pagesCESPL - Profile1Satvinder Deep SinghNo ratings yet
- Forest Laws and Their Impact On Adivasi Economy in Colonial India1Document12 pagesForest Laws and Their Impact On Adivasi Economy in Colonial India1NidhiNo ratings yet
- Inorganic Chemistry 1 - Alkali Metals RevisioDocument7 pagesInorganic Chemistry 1 - Alkali Metals RevisioAshleyn Mary SandersNo ratings yet
- Chapter 14 NotesDocument21 pagesChapter 14 NotesnightdazeNo ratings yet
- Welcome To Good Shepherd Chapel: Thirty-Third Sunday in Ordinary TimeDocument4 pagesWelcome To Good Shepherd Chapel: Thirty-Third Sunday in Ordinary Timesaintmichaelpar7090No ratings yet
- Event Management NotesDocument24 pagesEvent Management Notesatoi firdausNo ratings yet
- Wild Amazon Cradle of Life Film TestDocument2 pagesWild Amazon Cradle of Life Film TestQuratulain MustafaNo ratings yet
- Chapter 13 Lecture 1 Career OptionsDocument24 pagesChapter 13 Lecture 1 Career OptionseltpgroupNo ratings yet
- Errata Sheet 1.7 - Dropzone Commander Official Update: NEW ADDITIONS/ CHANGES FROM VERSION 1.6 Highlighted in RedDocument2 pagesErrata Sheet 1.7 - Dropzone Commander Official Update: NEW ADDITIONS/ CHANGES FROM VERSION 1.6 Highlighted in RedTecnocastoroNo ratings yet
- The Power of Faith Confession & WorshipDocument38 pagesThe Power of Faith Confession & WorshipLarryDelaCruz100% (1)
- The Cannibalization of Jesus and The Persecution of The Jews.Document193 pagesThe Cannibalization of Jesus and The Persecution of The Jews.DrChris JamesNo ratings yet
- FAGL TcodesDocument3 pagesFAGL TcodesRahul100% (2)
- Factors Influencing Savings Mobilization by Commercial BanksDocument81 pagesFactors Influencing Savings Mobilization by Commercial BanksNicholas Gowon100% (7)
- Cape Sewing - Industrial Sewing TechnologyDocument33 pagesCape Sewing - Industrial Sewing TechnologyMonika GadgilNo ratings yet
- Neonatal Intubation: Past, Present, and Future: Practice GapsDocument9 pagesNeonatal Intubation: Past, Present, and Future: Practice GapskiloNo ratings yet
- CIRFormDocument3 pagesCIRFormVina Mae AtaldeNo ratings yet