Download as pdf or txt
You might also like
- Orthopedic DHA MCQDocument18 pagesOrthopedic DHA MCQAsif Newaz92% (12)
- How To Become Psychiatrist in MalaysiaDocument9 pagesHow To Become Psychiatrist in MalaysiaHamdi Ibrahim100% (1)
- Internal Medicine McqsDocument15 pagesInternal Medicine Mcqsunlimited world100% (2)
- Khalida - Clinical Significance of Early Repolarization On Long QT SyndromeDocument7 pagesKhalida - Clinical Significance of Early Repolarization On Long QT SyndromeraniakjsNo ratings yet
- Correccion Del QT 16 OKKDocument16 pagesCorreccion Del QT 16 OKKMilner GranadosNo ratings yet
- Alahmadi 2021Document21 pagesAlahmadi 2021NeaguNo ratings yet
- QT Dispersion Problems of Methodology AnDocument15 pagesQT Dispersion Problems of Methodology AnedNo ratings yet
- Antz Elev ItchDocument12 pagesAntz Elev ItchAdrianaNo ratings yet
- Genetic Biomarkers For The Risk of Seizures in Long QT SyndromeDocument9 pagesGenetic Biomarkers For The Risk of Seizures in Long QT SyndromeР. МөнхжинNo ratings yet
- Jurnal EkgDocument26 pagesJurnal EkgUsman ohorellaNo ratings yet
- Literature Review 2019Document15 pagesLiterature Review 2019Р. МөнхжинNo ratings yet
- QT SyndromeDocument7 pagesQT SyndromeRikhardo RkNo ratings yet
- 1 s2.0 S2666084923003509 MainDocument6 pages1 s2.0 S2666084923003509 MainThato PaulusNo ratings yet
- Flecainide ChallengeDocument7 pagesFlecainide ChallengehariNo ratings yet
- 1 s2.0 S0735109716003387 MainDocument12 pages1 s2.0 S0735109716003387 MainghhercockNo ratings yet
- 1 s2.0 S2667296021000586 MainDocument10 pages1 s2.0 S2667296021000586 MainLauraNo ratings yet
- Genetic Case 1Document44 pagesGenetic Case 1blue pianoNo ratings yet
- Psycopharmacology For PhysicianDocument2 pagesPsycopharmacology For PhysicianSyawal PratamaNo ratings yet
- Initial Diagnosis and Management of Acutely Elevated Intracranial PressureDocument8 pagesInitial Diagnosis and Management of Acutely Elevated Intracranial PressureGlessin MurilloNo ratings yet
- Pedoman Jacc Prolong QtcDocument20 pagesPedoman Jacc Prolong Qtchasan andrianNo ratings yet
- Long QT Syndrome: Diagnosis and Management: BackgroundDocument8 pagesLong QT Syndrome: Diagnosis and Management: BackgroundArizkie AlfiNo ratings yet
- Long QT SyndromeDocument9 pagesLong QT SyndromeRoberto SalazarNo ratings yet
- Diagnosis, Management and Therapeutic Strategies For Congenital Long QT SyndromeDocument7 pagesDiagnosis, Management and Therapeutic Strategies For Congenital Long QT SyndromeAndreea TeodorescuNo ratings yet
- Corrected QT Interval in Systemic Sclerosis Patients: Archives of Rheumatology & Arthritis ResearchDocument4 pagesCorrected QT Interval in Systemic Sclerosis Patients: Archives of Rheumatology & Arthritis ResearchAlexandruFlaviaNo ratings yet
- Lin 2009Document7 pagesLin 2009Nur Syamsiah MNo ratings yet
- Japanese StudyDocument11 pagesJapanese StudyР. МөнхжинNo ratings yet
- Benoid., 2005. Penelitian RCT Pada Kelainan Elektrolit Terhadap Prolong QTDocument6 pagesBenoid., 2005. Penelitian RCT Pada Kelainan Elektrolit Terhadap Prolong QThasan andrianNo ratings yet
- QT-interval - JAMA 2003Document8 pagesQT-interval - JAMA 2003Poligar49No ratings yet
- 1 Evaluation and Management of ShockDocument11 pages1 Evaluation and Management of ShockYESSICA CARENALGANo ratings yet
- Fully Automated Method For QT Interval Measurement in ECG: October 2006Document5 pagesFully Automated Method For QT Interval Measurement in ECG: October 2006Cristina DragomirNo ratings yet
- Ultrasound Imaging of Congestion in Heart Failure Examinations BeyondDocument10 pagesUltrasound Imaging of Congestion in Heart Failure Examinations BeyondAncylostoma DuodenaleNo ratings yet
- Manejo Alargamiento QTDocument10 pagesManejo Alargamiento QTManel EMNo ratings yet
- ST Elevation After Myocardial Infarction: What Does It Mean?Document2 pagesST Elevation After Myocardial Infarction: What Does It Mean?IqbalDzakyNo ratings yet
- Biomedical Signal Processing and ControlDocument10 pagesBiomedical Signal Processing and ControlSERGIO ANDRES ROMERO TORRESNo ratings yet
- Bhattacharya Olshansky 2019 Electrolytes and The Ecg IntervalsDocument3 pagesBhattacharya Olshansky 2019 Electrolytes and The Ecg IntervalsaisyahhelmadevithalibNo ratings yet
- 62 Full PDFDocument12 pages62 Full PDFrizkiaautikasariNo ratings yet
- David N.2007Document7 pagesDavid N.2007Giulia AndreeaNo ratings yet
- Guidance On ECG Monitoring in NDR CTB - ENGDocument22 pagesGuidance On ECG Monitoring in NDR CTB - ENGDokteranak CalangNo ratings yet
- Systemic Approach On Immediate Evaluation and Management of Hyperacute StrokeDocument25 pagesSystemic Approach On Immediate Evaluation and Management of Hyperacute StrokeDodik TugasworoNo ratings yet
- Articulo 4Document8 pagesArticulo 4JL MaravillasNo ratings yet
- SCCT Guidelines For CT in Congenital Heart Disease - Part 1 - 2015Document18 pagesSCCT Guidelines For CT in Congenital Heart Disease - Part 1 - 2015Andreea-Claudia RusuNo ratings yet
- RECONSIDERING VASOPRESSORS For CARDIOGENIC SHOCK Everything Should Be Made As Simple As Possible, But Not SimplerDocument33 pagesRECONSIDERING VASOPRESSORS For CARDIOGENIC SHOCK Everything Should Be Made As Simple As Possible, But Not Simpleralejandro montesNo ratings yet
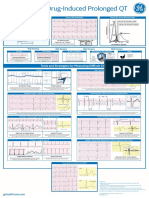
- Recognition of Drug-Induced ProloRev2Document1 pageRecognition of Drug-Induced ProloRev2rogeriocorreaNo ratings yet
- Predicting Outcomes in Acute Coronary Syndrome Using Biochemical MarkersDocument9 pagesPredicting Outcomes in Acute Coronary Syndrome Using Biochemical MarkersSitti Monica A. AmbonNo ratings yet
- Hemodynamic Monitoring in Cardiogenic Shock: ReviewDocument6 pagesHemodynamic Monitoring in Cardiogenic Shock: ReviewLeyden Chavez VergaraNo ratings yet
- 1 s2.0 S1934592522000673 MainDocument16 pages1 s2.0 S1934592522000673 MainDannis VNo ratings yet
- Emboli ParuDocument16 pagesEmboli ParuELF RaniNo ratings yet
- Perera Et Al 2023 Arrhythmia and Death Following Percutaneous Revascularization in Ischemic Left VentricularDocument10 pagesPerera Et Al 2023 Arrhythmia and Death Following Percutaneous Revascularization in Ischemic Left VentriculardiegoiglesiasNo ratings yet
- Corbacioglu SerefDocument6 pagesCorbacioglu SerefFabio Antonio Villadiego FontanillaNo ratings yet
- Joacp 38 208 PDFDocument7 pagesJoacp 38 208 PDFTan AwiNo ratings yet
- How To Detect Long QT in A Heartbeat - Clinical ViewDocument9 pagesHow To Detect Long QT in A Heartbeat - Clinical ViewAlberto MHNo ratings yet
- Pic No Es #Document13 pagesPic No Es #Tatiana FuenmayorNo ratings yet
- Kallergis 2012Document9 pagesKallergis 2012fairuzNo ratings yet
- PIIS2468644122001219Document3 pagesPIIS2468644122001219Rifda HsnyyhNo ratings yet
- Mohebi 2017Document26 pagesMohebi 2017Ioana GuțăNo ratings yet
- long-QT Syndrome Epinephrine Unmasks Latent Mutation Carriers With LQT1 Form of CongenitalDocument12 pageslong-QT Syndrome Epinephrine Unmasks Latent Mutation Carriers With LQT1 Form of Congenitalapi-26166949No ratings yet
- Llenado Capilar en Choque SépticoDocument3 pagesLlenado Capilar en Choque SépticoAlejandro Manzanares BalladaresNo ratings yet
- Follow-Up of 316 Molecularly Defined Pediatric Long-QT Syndrome PatientsDocument9 pagesFollow-Up of 316 Molecularly Defined Pediatric Long-QT Syndrome PatientsР. МөнхжинNo ratings yet
- CV Bun 2Document8 pagesCV Bun 2Cami ElenaNo ratings yet
- Acn3 6 310Document14 pagesAcn3 6 310ErdaNo ratings yet
- 1726-Article Text-23983-2-10-20220330Document6 pages1726-Article Text-23983-2-10-20220330CL X-RAY IMAGESNo ratings yet
- Masurarea QTDocument8 pagesMasurarea QTGabriela GheorgheNo ratings yet
- Clinical Handbook of Cardiac ElectrophysiologyFrom EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverNo ratings yet
- Fluids Electrolytes Visual NotesDocument8 pagesFluids Electrolytes Visual NotesVin Lorenzo CampbellNo ratings yet
- Grodno State Medical University: Assistant Lecturer of The Department of OphthalmologyDocument24 pagesGrodno State Medical University: Assistant Lecturer of The Department of OphthalmologyTeguh Imana NugrahaNo ratings yet
- Nizoral Shampoo - Google SearchDocument1 pageNizoral Shampoo - Google SearchHazel SilvaNo ratings yet
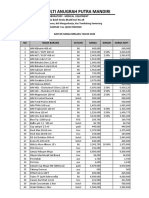
- Daftar Harga Rsud Salatiga 2020Document2 pagesDaftar Harga Rsud Salatiga 2020BomeNo ratings yet
- JurnalDocument16 pagesJurnalNurul RiskiNo ratings yet
- Flexor Tendon InjuriesDocument48 pagesFlexor Tendon InjuriesBela RonaldoeNo ratings yet
- Prevalence of Bacterial Pneumonia in Sheep in and Around Hyderabad, TelanganaDocument3 pagesPrevalence of Bacterial Pneumonia in Sheep in and Around Hyderabad, TelanganaKrishna ChaitanyaNo ratings yet
- EtatDocument121 pagesEtatBhoja Raj GAUTAMNo ratings yet
- The Role of Vitamin D in Athletic PerformanceDocument3 pagesThe Role of Vitamin D in Athletic PerformanceLeighton SmithNo ratings yet
- ARTIC MouldChart 2017 220623 162138Document8 pagesARTIC MouldChart 2017 220623 162138adellya tasya sukmaNo ratings yet
- Orthodontics: Vincent O. Kokich JR., D.M.D., M.S.DDocument1 pageOrthodontics: Vincent O. Kokich JR., D.M.D., M.S.DJa MishicaNo ratings yet
- Lockin Specs For Transport VentilatorDocument2 pagesLockin Specs For Transport VentilatorAlauddin SyahNo ratings yet
- Parents Sue City of New York Over Forced' Vaccination OrderDocument13 pagesParents Sue City of New York Over Forced' Vaccination Orderadan_infowarsNo ratings yet
- Reproduction, Technology, and The SocietyDocument38 pagesReproduction, Technology, and The SocietyJep LorenzoNo ratings yet
- Test DoseDocument4 pagesTest DoseibunqumairaNo ratings yet
- Preboards NP2Document6 pagesPreboards NP2Marco AglibotNo ratings yet
- Men, Women, and Depression - Undoing DepressionDocument3 pagesMen, Women, and Depression - Undoing DepressionlabebuNo ratings yet
- Role of Endoscopic Stent Insertion On Managmeent of Gastric Twist After Sleeve GastrectomyDocument6 pagesRole of Endoscopic Stent Insertion On Managmeent of Gastric Twist After Sleeve GastrectomyJorge SalazarNo ratings yet
- Sex Linked Inheritance Pedigree 2016Document37 pagesSex Linked Inheritance Pedigree 2016JacNo ratings yet
- History Taking: Ma. Sheila Blossom B. Bo RM, RN, MmeDocument14 pagesHistory Taking: Ma. Sheila Blossom B. Bo RM, RN, Mmejhayrus pletaNo ratings yet
- Multicalibrator: (Toll Free)Document1 pageMulticalibrator: (Toll Free)malik abbasNo ratings yet
- APA - DSM5 - Severity of Posttraumatic Stress Symptoms Adult PDFDocument3 pagesAPA - DSM5 - Severity of Posttraumatic Stress Symptoms Adult PDFStephanny Per EspitiaNo ratings yet
- PBSC - Meningitis LetterPBA2019 - Letterhead - FinalDocument1 pagePBSC - Meningitis LetterPBA2019 - Letterhead - FinalScott SuttonNo ratings yet
- Sports-Related InjuriesDocument2 pagesSports-Related Injurieslil trxshNo ratings yet
- Apf Clinic Aftercare InstructionsDocument4 pagesApf Clinic Aftercare InstructionsapNo ratings yet
- CancerDocument5 pagesCancerapi-3771269No ratings yet
- Mechanism of AutoimmunityDocument29 pagesMechanism of AutoimmunityMalliga SundareshanNo ratings yet