Download as pdf or txt
You might also like
- 1994 - Daily - Bankruptcy and Corporate Governance The Impact of Board Composition and StructureDocument16 pages1994 - Daily - Bankruptcy and Corporate Governance The Impact of Board Composition and Structureahmed sharkasNo ratings yet
- Sigmadrive Quick Reference Manual Rev 3.05.00mDocument57 pagesSigmadrive Quick Reference Manual Rev 3.05.00mРухулла АгакеримовNo ratings yet
- Presto Coffee Machine Manual EnglishDocument72 pagesPresto Coffee Machine Manual EnglishRehman ChNo ratings yet
- 00 Dynamic Marketing StrategyDocument4 pages00 Dynamic Marketing StrategyferrychrNo ratings yet
- Essentia Health Sports Medicine ContractDocument9 pagesEssentia Health Sports Medicine ContractDuluth News TribuneNo ratings yet
- Wasting Our Waterways ReportDocument61 pagesWasting Our Waterways ReportJackson SinnenbergNo ratings yet
- Factors Affecting Water Pollution A Review 2157 7625 1000225Document4 pagesFactors Affecting Water Pollution A Review 2157 7625 1000225adrian morenoNo ratings yet
- ECC IMP QuestionsDocument12 pagesECC IMP QuestionsSoban KasmaniNo ratings yet
- 1599668022strategies For Export Promotion of Popped Makhana in India Compressed 1Document5 pages1599668022strategies For Export Promotion of Popped Makhana in India Compressed 1castro dasNo ratings yet
- 2005-2006 Water News Delaware Water ResourcesDocument8 pages2005-2006 Water News Delaware Water ResourcesDelaware Water ResourcesNo ratings yet
- Marketing Strategy 5133 1Document5 pagesMarketing Strategy 5133 1B16 Prashant patilNo ratings yet
- All-Star Sports - Winter SeasonDocument12 pagesAll-Star Sports - Winter SeasonLNP MEDIA GROUP, Inc.No ratings yet
- Chapter 1: Kinnickinnic River Watershed Restoration Plan Executive SummaryDocument14 pagesChapter 1: Kinnickinnic River Watershed Restoration Plan Executive SummarySweet WaterNo ratings yet
- Chapter 2 Marketing Strategy PlanningDocument33 pagesChapter 2 Marketing Strategy PlanningĐặng Ngọc Yến TrâmNo ratings yet
- Marketing Strategy - Scotia WealthDocument24 pagesMarketing Strategy - Scotia WealthCarolina QuineteNo ratings yet
- 2019 Book TheSportsMedicinePhysician Páginas 501 536Document36 pages2019 Book TheSportsMedicinePhysician Páginas 501 536Beatriz PerdomoNo ratings yet
- Communication Process Project Group BrilliantDocument14 pagesCommunication Process Project Group BrilliantAsheba LevyNo ratings yet
- WMed Residency Match 2023Document3 pagesWMed Residency Match 2023WWMTNo ratings yet
- Sports SyllabusDocument4 pagesSports SyllabusSaif Ahmed LariNo ratings yet
- Certificate in Communication SkillsDocument5 pagesCertificate in Communication SkillsTetteh SamuelNo ratings yet
- Retail Marketing PrintableDocument27 pagesRetail Marketing PrintableMadena LifeNo ratings yet
- A Wearable Electrochemical Biosensor For The Monitoring of Metabolites and NutrientsDocument13 pagesA Wearable Electrochemical Biosensor For The Monitoring of Metabolites and NutrientsBAUTISTA DIPAOLA100% (1)
- Survey Report On Water Pollution in Bishnumati RiverDocument21 pagesSurvey Report On Water Pollution in Bishnumati RiverAbhas Dharananda RajopadhyayaNo ratings yet
- Water Pollution Through Energy Sector PDFDocument5 pagesWater Pollution Through Energy Sector PDFJan AshleyNo ratings yet
- Intership Report - by Tanya Mendiratta (2) - 1Document63 pagesIntership Report - by Tanya Mendiratta (2) - 1TanyaNo ratings yet
- 485 Type Photo-Electricity Smoke Fire Detector Alarm InstructionsDocument12 pages485 Type Photo-Electricity Smoke Fire Detector Alarm Instructionsganesanv8685100% (1)
- Royal Palm Services AnalysisDocument22 pagesRoyal Palm Services AnalysisM Tanzeel Rahman KhanNo ratings yet
- Internship Report On FX Unity Global LTD by Nakib AhmadDocument28 pagesInternship Report On FX Unity Global LTD by Nakib AhmadDipti GuptaNo ratings yet
- Medicine Ball - ProceduresDocument1 pageMedicine Ball - ProceduresDanielBC100% (1)
- 19me553 Industrial Training ReportDocument37 pages19me553 Industrial Training ReportParth MaldhureNo ratings yet
- Marketing Environment PDFDocument38 pagesMarketing Environment PDFDipti LakhotiaNo ratings yet
- Prescription - 1780912 - 12 11 2021 - Dr. Anindya Dutt - Apollo 2471636716100978Document2 pagesPrescription - 1780912 - 12 11 2021 - Dr. Anindya Dutt - Apollo 2471636716100978Debjit GangulyNo ratings yet
- Ti 01-2010Document27 pagesTi 01-2010Deepak ShuklaNo ratings yet
- Greeting Custom Around The WorldDocument2 pagesGreeting Custom Around The WorldKadek WidyaNo ratings yet
- Teaching Guide 3 1 3Document40 pagesTeaching Guide 3 1 3The Pro UMERNo ratings yet
- Traditional and Contemporary Techniques For Optimizing Root Canal IrrigationDocument9 pagesTraditional and Contemporary Techniques For Optimizing Root Canal IrrigationrintanfsNo ratings yet
- đất nc học Buổi 1Document2 pagesđất nc học Buổi 1Anh DuongNo ratings yet
- Guidelines For Management of Patients With A Short BowelDocument12 pagesGuidelines For Management of Patients With A Short BowelMarselya GaniNo ratings yet
- Spring 2002 Water News Delaware Water ResourcesDocument8 pagesSpring 2002 Water News Delaware Water ResourcesDelaware Water ResourcesNo ratings yet
- Selection Criteria Website 2022Document12 pagesSelection Criteria Website 2022api-245089582No ratings yet
- Internship ReportDocument50 pagesInternship ReportSachinNo ratings yet
- ME8793 Process Planning and Cost EStimation UNIT 5 NotesDocument26 pagesME8793 Process Planning and Cost EStimation UNIT 5 NotesLEO PRAVIN PNo ratings yet
- T1 - What Is Marketing - Lecture Slides (Required) - Narrated SlidesDocument59 pagesT1 - What Is Marketing - Lecture Slides (Required) - Narrated Slidesan nguyenNo ratings yet
- Epidemiology of ObesityDocument32 pagesEpidemiology of ObesityamsabavanNo ratings yet
- International Marketing PADocument9 pagesInternational Marketing PAkangruiNo ratings yet
- Will Artificial Intelligence Take Over Humanresources Recruitment and Selection?Document10 pagesWill Artificial Intelligence Take Over Humanresources Recruitment and Selection?NikolinaOršičekNo ratings yet
- Coffee Marketing ResearchDocument9 pagesCoffee Marketing ResearchbojaNo ratings yet
- Stationing Smart Contract As A ContractDocument44 pagesStationing Smart Contract As A ContractVinayak GuptaNo ratings yet
- ALTTC Project Report FullDocument24 pagesALTTC Project Report FullKrishna ShahNo ratings yet
- Seeber K.G.2015. SimultaneousInterpretingDocument18 pagesSeeber K.G.2015. SimultaneousInterpretingSalah SalemNo ratings yet
- Geotagging Manual 2013Document101 pagesGeotagging Manual 2013Jezell De Torres-dela CruzNo ratings yet
- Description: Data Cable, U/UTP, Category 6, AWG23, Euroclass CDocument2 pagesDescription: Data Cable, U/UTP, Category 6, AWG23, Euroclass Cosmanovic2020No ratings yet
- DIET Hassan Science EM Q Bank 2022-23Document60 pagesDIET Hassan Science EM Q Bank 2022-23masoodmohsinNo ratings yet
- Pre-Form Stair Installation GuideDocument32 pagesPre-Form Stair Installation GuideYoussef NaoumNo ratings yet
- UTI GuidelineDocument10 pagesUTI Guidelinecatalin petreNo ratings yet
- Retail MarketingDocument25 pagesRetail MarketingFayaaz KhanNo ratings yet
- Marketing Communications MOD001178: Anglia Ruskin UniversityDocument21 pagesMarketing Communications MOD001178: Anglia Ruskin UniversityJayc LeeNo ratings yet
- GO 680 Protest and Mass Demonstration ResponseDocument8 pagesGO 680 Protest and Mass Demonstration ResponseNews10NBCNo ratings yet
- U2-M4-lhizaBeing A Team Player (06-14-05)Document26 pagesU2-M4-lhizaBeing A Team Player (06-14-05)John Lester Burca MagdaraogNo ratings yet
- 2017-2018 Sports Qualifying Physical Examination Clearance FormDocument4 pages2017-2018 Sports Qualifying Physical Examination Clearance FormChris HuntNo ratings yet
- Simulation Study of LPG Cooking BurnerDocument3 pagesSimulation Study of LPG Cooking BurnerBensinghdhas Sathiya Dhas100% (1)
- BM 4 - Bricks & BlocksDocument30 pagesBM 4 - Bricks & BlocksArch Reem AlzyoudNo ratings yet
- Exercise 1. You Have Been Given A Form Which Shows The Details of Technical Jobs Carried OutDocument2 pagesExercise 1. You Have Been Given A Form Which Shows The Details of Technical Jobs Carried OutNgo Gia Huy (K15 HCM)No ratings yet
- Metal Oxide Varistor Elbow M o V e Surge Arrester Catalog Ca235025enDocument8 pagesMetal Oxide Varistor Elbow M o V e Surge Arrester Catalog Ca235025enale_1905No ratings yet
- Luserne Tree InformationDocument26 pagesLuserne Tree Informationpierre van wykNo ratings yet
- Cells Teachers Guide Discovery EducationDocument38 pagesCells Teachers Guide Discovery EducationKari Kristine Hoskins BarreraNo ratings yet
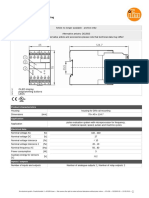
- Datasheet DD2603Document3 pagesDatasheet DD2603RONALD TERRAZASNo ratings yet
- RDSO Controlled Items Transferred To Other Production Units & COREDocument5 pagesRDSO Controlled Items Transferred To Other Production Units & CORERakesh RoshanNo ratings yet
- Acute Rheumatic Fever - Clinical Manifestations and Diagnosis - UpToDateDocument15 pagesAcute Rheumatic Fever - Clinical Manifestations and Diagnosis - UpToDateDannyGutierrezNo ratings yet
- 6 Fem3343 M6 - Prinsip Dan Nilai Etika 27mac18Document38 pages6 Fem3343 M6 - Prinsip Dan Nilai Etika 27mac18Ron ChongNo ratings yet
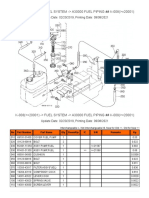
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- Chapter 14 Test Bank - Version1Document25 pagesChapter 14 Test Bank - Version1mjjongh103No ratings yet
- 59 Why Nuts and Bolts Come Loose V1Document2 pages59 Why Nuts and Bolts Come Loose V1civicbladeNo ratings yet
- Tecan Sunrise Absorbance Reader Analyser - User ManualDocument74 pagesTecan Sunrise Absorbance Reader Analyser - User Manualomer oartbNo ratings yet
- Calibration of Dosimeters Used in Radiation TherapyDocument122 pagesCalibration of Dosimeters Used in Radiation TherapySOHON SINHA MAHAPATRANo ratings yet
- Literature of Exile in Goli Taraqqi's Short StoriesDocument23 pagesLiterature of Exile in Goli Taraqqi's Short StoriesmarvehNo ratings yet
- Appendix 66 Rpci Updated Ues JehanDocument58 pagesAppendix 66 Rpci Updated Ues JehanOmar Gulam JrNo ratings yet
- ASIYADocument3 pagesASIYASOFIKUL HUUSAINNo ratings yet
- Organic Reactions Volume 26Document183 pagesOrganic Reactions Volume 26lerayerNo ratings yet
- Bacteria ProfileDocument18 pagesBacteria ProfileNOR-FATIMAH BARATNo ratings yet
- The Importance of Macronutrients & Micronutrients in PlantDocument25 pagesThe Importance of Macronutrients & Micronutrients in Plantmarinihassim100% (5)
- Mushroom BoardsDocument4 pagesMushroom BoardsRemyaNo ratings yet
- CPM 0250 Water Pumping System Using River Force DevDocument9 pagesCPM 0250 Water Pumping System Using River Force DevmanjunathNo ratings yet
- International StandardDocument8 pagesInternational Standardnazrul islamNo ratings yet
- Astrological Study of Infertility - ConclusionDocument9 pagesAstrological Study of Infertility - ConclusionAnamika SNo ratings yet
- Caring For Your African American/Biracial Child's HairDocument32 pagesCaring For Your African American/Biracial Child's Hair4kidslikemeNo ratings yet
- Bosch ManualDocument56 pagesBosch Manualjhon manuel de jesus100% (1)
- Pentavitin - DSMDocument3 pagesPentavitin - DSMRnD Roi SuryaNo ratings yet
- 2007-Current MaxxForce Engine Breakout Harness Reference (EGES545)Document14 pages2007-Current MaxxForce Engine Breakout Harness Reference (EGES545)Enrrique Lara100% (1)
- Final DraftDocument37 pagesFinal DraftMorareng MariettaNo ratings yet